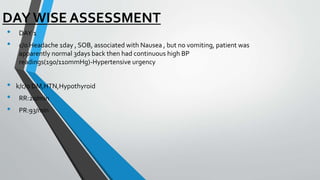
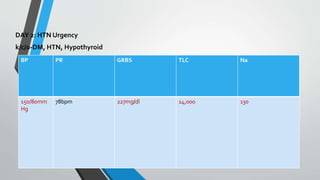
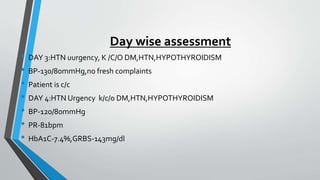
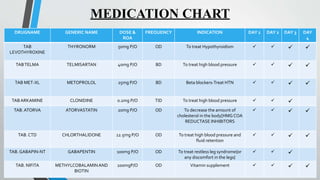
The document provides a detailed medical evaluation of a 61-year-old female patient diagnosed with hypertensive urgency, presenting with symptoms such as headaches and high blood pressure readings. It includes vital signs, laboratory results, medication lists, and day-wise assessments over four days, detailing changes in her condition and treatment. Goals of therapy focus on maintaining normal blood pressure, improving hemoglobin levels, and patient counseling on dietary and lifestyle changes.