Polymyositis is an idiopathic inflammatory myopathy that causes symmetrical, proximal muscle weakness; elevated skeletal muscle enzyme levels; and characteristic electromyography (EMG) and muscle biopsy findings
Dr Abdullah Ansari
PG-2 (Medicine)
AMU ALIGARH
A general approach to periodic paralysis....
(including hypokalemic periodic paralysis and thyrotoxic periodic paralysis, and other “Channelopathies” or “Membranopathies)
Pathophysiology
Epidemiology
Primary or familial periodic paralysis
Secondary periodic paralysis
Conventional classification of periodic paralysis
Classification of primary periodic paralysis based on ion-channel abnormalities
Clinical approach to a case of periodic paralysis
History of muscle weakness
Age of onset
Family history
Timing
Intensity
History of administration of certain drugs
Clinical examination
Differential Diagnosis
Laboratory investigations
Serum K+
CPK and serum myoglobin
ECG
EMG
Nerve conduction studies
Provocative Testing
Muscle biopsy
Treatment
Prognosis
Case Presentation of a patient presented with polyradiculoneuropathy and bilateral bulbar palsy. Detailed evaluation finally pinpoints to Guillian barre syndrome.
Anatomy of pituitary glands,its secretions and disorders due to its imbalance.
Adrenal gland anatomy,its secretions and tumors of adrenal gland and disorders associated with it.
Dr Abdullah Ansari
PG-2 (Medicine)
AMU ALIGARH
A general approach to periodic paralysis....
(including hypokalemic periodic paralysis and thyrotoxic periodic paralysis, and other “Channelopathies” or “Membranopathies)
Pathophysiology
Epidemiology
Primary or familial periodic paralysis
Secondary periodic paralysis
Conventional classification of periodic paralysis
Classification of primary periodic paralysis based on ion-channel abnormalities
Clinical approach to a case of periodic paralysis
History of muscle weakness
Age of onset
Family history
Timing
Intensity
History of administration of certain drugs
Clinical examination
Differential Diagnosis
Laboratory investigations
Serum K+
CPK and serum myoglobin
ECG
EMG
Nerve conduction studies
Provocative Testing
Muscle biopsy
Treatment
Prognosis
Case Presentation of a patient presented with polyradiculoneuropathy and bilateral bulbar palsy. Detailed evaluation finally pinpoints to Guillian barre syndrome.
Anatomy of pituitary glands,its secretions and disorders due to its imbalance.
Adrenal gland anatomy,its secretions and tumors of adrenal gland and disorders associated with it.
Septicemia is a life threatening complication this is also called as the blood infection. this is an infection that occurs when bacteria enters the blood stream and spread elsewhere in the body such as lungs and skin.
These bacteria affects the bodily function of the blood as it is responsible for carrying of oxygen, nutrients to your cells and it also carry's waste and carbon dioxide.
More than 90,000 people die every year in India due to sepsis.
SOAP NOTE SAMPLE FORMAT FOR MRCName LPDateTime 1315.docxpbilly1
SOAP NOTE SAMPLE FORMAT FOR MRC
Name: LP
Date:
Time: 1315
Age: 30
Sex: F
SUBJECTIVE
CC:
“I am having vaginal itching and pain in my lower abdomen.”
HPI:
Pt is a 30y/o AA female, who is a new patient that has recently moved to Miami. She seeks treatment today after unsuccessful self-treatment of vaginal itching, burning upon urination, and lower abdominal pain. She is concerned for the presence of a vaginal or bladder infection, or an STD. Pt denies fever. She reports the itching and burning with urination has been present for 3 weeks, and the abdominal pain has been intermittent since months ago. Pt has tried OTC products for the itching, including Monistat and Vagisil. She denies any other urinary symptoms, including urgency or frequency. She describes the abdominal pain as either sharp or dull. The pain level goes as high as 8 out of 10 at times. 200mg of PO Advil PRN reduces the pain to a 7/10. Pt denies any aggravating factors for the pain. Pt reports that she did start her menstrual cycle this morning, but denies any other discharge other that light bleeding beginning today. Pt denies douching or the use of any vaginal irritants. She reports that she is in a stable sexual relationship, and denies any new sexual partners in the last 90 days. She denies any recent or historic known exposure to STDs. She reports the use of condoms with every coital experience, as well as this being her only form of contraceptive. She reports normal monthly menstrual cycles that last 3-4 days. She reports dysmenorrhea, which she also takes Advil for. She reports her last PAP smear was in 7/2016, was normal, and reports never having an abnormal PAP smear result. Pt denies any hx of pregnancies. Other medical hx includes GERD. She reports that she has an Rx for Protonix, but she does not take it every day. Her family hx includes the presence of DM and HTN.
Current Medications:
Protonix 40mg PO Daily for GERD
MTV OTC PO Daily
Advil 200mg OTC PO PRN for pain
PMHx:
Allergies:
NKA & NKDA
Medication Intolerances:
Denies
Chronic Illnesses/Major traumas
GERD
Hospitalizations/Surgeries
Denies
Family History
Father- DM & HTN; Mother- HTN; Older sister- DM & HTN; Maternal and paternal grandparents without known medical issues; 1 brother and 3 other sisters without known medical issues; No children.
Social History
Lives alone. Currently in a stable sexual relationship with one man. Works for DEFACS. Reports occasional alcohol use, but denies tobacco or illicit drug use.
ROS
General
Denies weight change, fatigue, fever, night sweats
Cardiovascular
Denies chest pain and edema. Reports rare palpitations that are relieved by drinking water
Skin
Denies any wounds, rashes, bruising, bleeding or skin discolorations, any changes in lesions
Respiratory
Denies cough. Reports dyspnea that accompanies the rare palpitations and is also relieved by drinking water
Eyes
Denies corrective lenses, blurring, visual changes of an.
Pneumonia is an inflammatory condition of the lung
affecting primarily the microscopic air sacs known as
alveoli.
Pneumonia is the most common infectious cause of death
in the United States.
It occurs in persons of all ages, although the clinical
manifestations are most severe in the very young, the
elderly, and the chronically ill.
Pneumonia is usually caused by infection with viruses or
bacteria and less commonly by other microorganisms,
certain medications and conditions such as autoimmune
Diseases
Definition
COPD is a disease characterized by the presence of airflow obstruction due to chronic bronchitis or emphysema; the air flow obstruction is generally progressive may be accompanied by airway hyper activity
Signs and Symptoms
Shortness of breath, especially during physical activities
Wheezing
Chest tightness
Having to clear your throat first thing in the morning, due to excess mucus in your lungs
DEFINITION:
A crater(ulcer) in the lining of the beginning of the small intestine (duodenum).
CAUSES OF DUODENAL ULCER
Infection with helicobacter pylori
Anti-inflammatory medicines
Other factors such as smoking, stress and drinking
Tuberculosis (TB) is a contagious, airborne disease that typically affects the lungs. TB is caused by a bacterium called Mycobacterium tuberculosis. If the infection is not treated quickly, the bacteria can travel through the bloodstream to infect other organs and tissues.
Sometimes, the bacteria will travel to the meninges, which are the membranes surrounding the brain and spinal cord. Infected meninges can result in a life-threatening condition known as meningeal tuberculosis. Meningeal tuberculosis is also known as tubercular meningitis or TB meningitis
A Tracheoesophageal fistula (TEF) is an abnormal connection (fistula) between the Oesophagus and the trachea. TEF is a common congenital abnormality.
Oesophageal atresia is failure of oesophagus to form a continuous passage from the pharynx to the stomach
TEF is an abnormal connection between the trachea and the oesophagus
Seizures which affect initially only one hemisphere of the brain. Symptoms include:
Contractions on just one side of the body
unusual head or eye movements
Numbness, tingling, or a feeling that something is crawling on the skin
Abdominal pain
Rapid heart rate or pulse
Sweating
Nausea
Diabetic foot is one of the most significant and devastating complications of diabetes and is defined as a foot affected by ulceration that is associated with nephropathy and peripheral arterial disease of the lower limb in a patient with diabetes.
Alcoholic liver disease is a term that encompasses the hepatic manifestations of alcohol overconsumption, including fatty liver, alcoholic hepatitis, and chronic hepatitis with hepatic fibrosis or cirrhosis.
Appendicitis is an inflammation of the appendix, a finger-shaped pouch that projects from your colon on the lower right side of your abdomen.
It requires immediate medical treatment. If left untreated, it can cause your appendix to rupture. This can be a serious and even fatal complication.
Acute appendicitis is more common than chronic appendicitis. Learn more about the similarities and differences between these conditions.
DKA is a life-threatening condition that develops when cells in the body are unable to get the glucose they need for energy because deficiency of the insulin.
Without enough insulin, the body begins to break down fat as fuel.
This process produces a buildup of acids in the bloodstream called ketones, eventually leading to diabetic ketoacidosis if untreated.
Rabies is a zoonotic disease caused by RNA viruses.
Virus is transmitted in the saliva of rabid mammals via a bite.
After entry to the central nervous system, these viruses cause an acute progressive encephalomyelitis.
The incubation period usually ranges from 1 to 3 months after exposure, but can range from days to years.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
263778731218 Abortion Clinic /Pills In Harare ,sisternakatoto
263778731218 Abortion Clinic /Pills In Harare ,ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group of receptionists, nurses, and physicians have worked together as a teamof receptionists, nurses, and physicians have worked together as a team wwww.lisywomensclinic.co.za/
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Knee anatomy and clinical tests 2024.pdfvimalpl1234
This includes all relevant anatomy and clinical tests compiled from standard textbooks, Campbell,netter etc..It is comprehensive and best suited for orthopaedicians and orthopaedic residents.
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
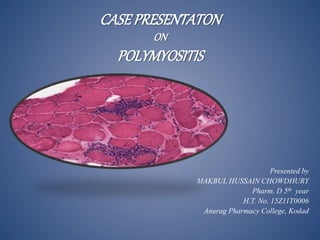
2. POLYMYOSITIS
Polymyositis is an idiopathic inflammatory myopathy that
causes symmetrical, proximal muscle weakness; elevated
skeletal muscle enzyme levels; and characteristic
electromyography (EMG) and muscle biopsy findings
3. TYPES
Bohan and Peter classify the idiopathic inflammatory myopathies
as follows :
I. Primary idiopathic polymyositis
II. Primary idiopathic dermatomyositis
III. Polymyositis or dermatomyositis associated with malignancy
IV. Childhood polymyositis or dermatomyositis
V. Polymyositis or dermatomyositis associated with another
connective-tissue disease
VI. Inclusion body myositis
VII. Miscellaneous (eg, eosinophilic myositis, myositis ossificans,
focal myositis, giant cell myositis)
4. Sign and Symptoms
Muscle pain and stiffness.
Muscle weakness, particularly in the belly (abdomen),
shoulders, upper arms, and hips.
Joint pain and stiffness.
Trouble catching your breath.
Problems with swallowing.
Irregular heart rhythms, if the heart muscle becomes inflamed
Etiology
Causes/Inheritance. In most cases, the cause of an
inflammatory myopathy like polymyositis (PM) is unclear
6. CASE STUDY
PATIENT NAME : Xxx
AGE: 30 yrs
GENDER :Female
DEPARTMENT : General medicine (FMW- I)
DOA : 23/01/19
CHIEF COMPLAINTS:
The patient XXX is a 30 years old female with following
complaints
Muscle pains From lower limbs, then upper limbs then whole
body There is also history of associated B/L knee joint pain but
no inflammation associated with it since 2 months.
Gen. Body weakness since 1 month.
Difficulty in swallowing since 10 days.
7. History of present Illness
There is no history of any associated fever, respiratory tract or
GIT infection in past few weeks, palpitation, heat or cold
intolerance, any change in urine color, cough, sputum.
There is also no history of use of any drugs for a long period,
also no history of any homeo or herbal medicine.
There is no h/o mouth ulcers alopacia, sun burns, change in
color of finger tips in cold.
8. Past History
There is no significant past medical or surgical history.
Family History
There is no family history of such illness and diabetes.
Drug History
No known allergy
Not using any kind of medicine for longer period of time.
Personal history
Married for last 8 years
Never conceived
Not properly evaluated for infertility
Non smoker and non drinker
9. Menstrual History
She c/o oligo-menorrhea for last one year.
No h/o dysmenorrhea
No h/o dysprunea.
Vital Sign
B.P 110/70 mmHg
Pulse 82/min
R.R 20/min
Temp. 98`F
10. General Physical Examination
No erythematous rash at face
Shawl sign -ve
Heliotrope rash –ve
No signs of cushing’s disease
No skin changes
No signs of hyper/hypothyroidism
11. Musculoskeletal & Nervous system
Well oriented in time place and person
GCS 15/15
Mild tenderness in muscles of lower thigh
Plantars B/L down going
Power 1/5 at proximal muscles, 3/5 at distal muscles of lower
limbs
2/5 in proximal muscles of upper limb and 4/5 in lower limbs
12. Other Systemic Examination
Respiratory system:
Normal in shape, bilateral chest movements equal, and
bilaterla air entery equal. On auscultation normal vesicular
breathing with few bibasal inspiratory crackles not changing
character with cough.
CVS:
Apex beat in 5th intercostal space just lateral to mid clavicular
line non taping, non-heaving with S1+S2+
Abdomen:
Scaphoid, with umbilicus normal in shape and position, flanks
not filled and no visible veins or stria
soft, non tender, no visceromegaly
No shifting dullness
Bowel sounds 3/min
14. CBC
Content Name Value Normal Value
Hb 10.7 mg/dl 12.0 - 15.5 mg/dl
WBC 10800 per microliter of
blood
4000-11000 per
microliter of blood
PLT count 191000per microliter of
blood
150,000-450,000 per
microliter of blood
N 88% 40–80%
E 1% 1–6%
ESR 100 mm/ hr 0-29 mm/hr
15. Serum electrolytes
RFTS
Content Name Value Normal Value
Na 139 mmol/L 135-145 mmol/L
K 4.4 mmol/L 3.5-5 mmol/L
Cl 102mmol/L 95-105 mmol/L
Content Name Value Normal Value
Urea 60 mg/dL 7 to 20 mg/dL
Creatinine 1.2 0.6 to 1.2mg/dL
16. LFTs
Urine C/E
Content Name Value Normal Value
ALT 370 IU 7 - 56 IU
AST 490 IU 10 - 40IU
S. bilirubin 0.7mg/dL 0.1 to 1.2 mg/dL
Alk. PO4 204 IU/L 44 to 147 IU/L
Content Name Value Normal Value
Albumin nil 3.5 to 5.5 g/dL
Pus cells rare 0-4
RBC 9-10 4 cells
Crystals uric acid + 250 to 750 milligrams
per 24 hours
Blood ++ 4 RBC/HPF
pH 7.0 about 6.0
19. Drug Chart
Name Brand Name Dose Frequency ROA Time of
Administration
Tab prednisolon
(blood disorders)
Prednisolone 55mg OD Oral 23-26/01
Cap. Omeprazole
(proton pump
inhibitors)
Zegerid 40mg OD Oral 24-26/01
Tab. Paracetamol
(knee joint pain )
DOLO 650mg TDS Oral 23-24/01
Bisphosphonates(bon
e pain)
Fosamax™ 70 mg OD Oral 23-26/01
Ca supplements CALBO-D 200mg OD Oral 25-26/01
20. Patient Counseling
Regarding Disease
There is no known way to prevent polymyositis, because the
exact cause is not known. In some cases where medicines
may be to blame, stopping these medicines can prevent
future episodes of the condition. Don't stop taking any
medicine without your doctor's approval.
If your symptoms get worse or you notice new symptoms,
call your healthcare provider. If you have trouble breathing
or can't swallow normally, you may need emergency medical
help.
21. Patient Counseling
Regarding Medication
Corticosteroids.
Drugs such as prednisone can be very effective in controlling
polymyositis symptoms. But prolonged use of these drugs
can have serious and wide-ranging side effects, which is why
your doctor may gradually taper the dose of medication
down to lower levels.
Omeprazole
Do not crush, break, or chew the tablets. Swallow this
medication whole with a glass of water.