Downloaded 20 times



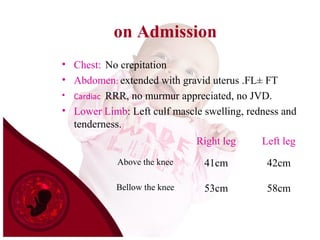



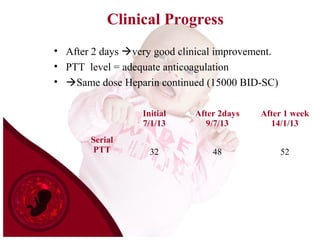
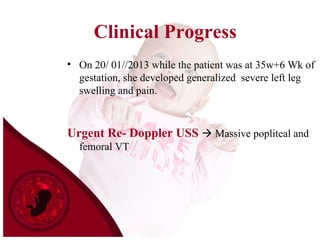
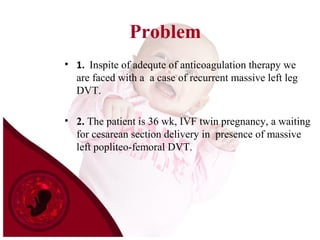
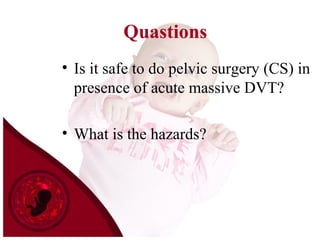



Mrs. S.A. is a 26-year old pregnant woman at 34 weeks of an IVF twin pregnancy who presented with left leg swelling and pain. She was diagnosed with left calf DVT. Despite anticoagulation therapy, she developed a recurrent massive left leg DVT. Given the increased risk of pulmonary embolism during delivery, doctors decided to place an IVC filter and perform a cesarean section. The procedures and pregnancy outcome were uncomplicated. Placement of an IVC filter can effectively reduce the risk of pulmonary embolism in high-risk pregnant patients with DVT.













































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









