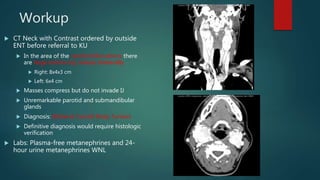
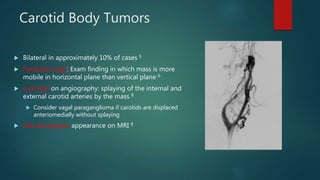
This document presents a history and physical examination (H&P) for a 47-year-old female patient referred for evaluation of a right neck mass. The mass had been present for 9 years and was recently growing steadily. Imaging revealed large enhancing bilateral carotid body tumors. Carotid body tumors are rare neuroendocrine tumors that typically arise from paraganglia near the carotid bifurcation. The patient underwent preoperative embolization followed by surgical resection of the right tumor via a transparotid approach, which resulted in temporary right vocal cord paralysis requiring a feeding tube.







































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
