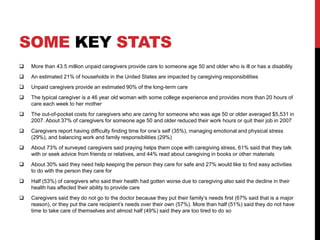
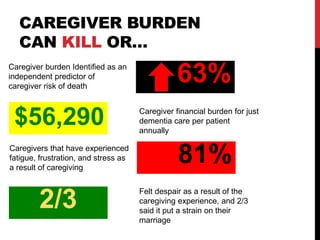
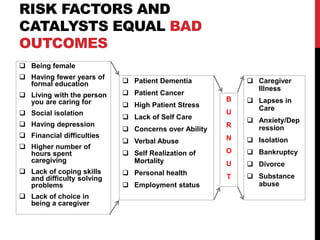
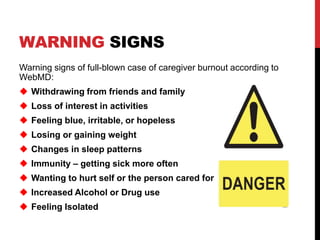
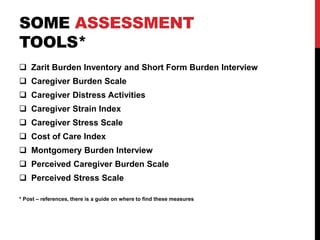
This document discusses caregiver burnout and provides strategies to mitigate it. It defines burnout as physical, emotional, and mental exhaustion resulting from prolonged stress. Both professional and unpaid caregivers can experience burnout. Risk factors include social isolation, depression, financial difficulties, and lack of self-care. Warning signs include withdrawing from others and changes in sleep and health. Assessment tools can identify burnout levels. The document recommends caregivers schedule personal time, seek help, and participate in self-care activities to prevent burnout.