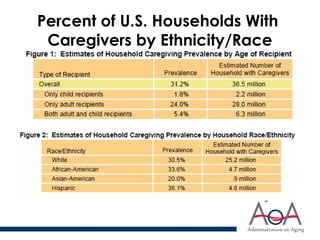
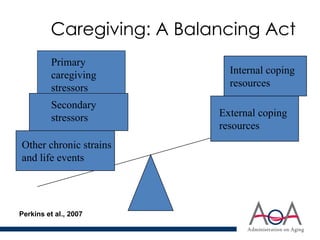
The document discusses the mental health needs of family caregivers, including the prevalence and impact of caregiving on health and well-being, and the factors contributing to caregiver strain versus resilience. It outlines effective interventions that can alleviate caregiver stress and improve mental health outcomes, emphasizing the importance of tailored support for caregivers. The document also highlights outreach strategies to engage caregivers and the significance of mental health referrals when needed.