
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to CAC Protocol Impact of smoking and calorie intake on bone fracture healing
Similar to CAC Protocol Impact of smoking and calorie intake on bone fracture healing (20)
CAC Protocol Impact of smoking and calorie intake on bone fracture healing
- 1. PROTOCOL The Impact of Smoking and Calorie Intake on Bone Fracture Healing in Osteoporotic Patients 4th year project report, submitted to the University of Manchester in partial fulfilment of the MPharm degree Richmond Arcillas 7990554 richmond.arcillas@student.manchester.ac.uk 7th May 2015 School of Pharmacy and Pharmaceutical Sciences Project Supervisor: Prof Leon Aarons
- 2. I Executive summary Introduction: Osteoporosis is one of the major causes of fractures in the elderly population worldwide. Osteoporotic patients who are admitted into hospital with fragility fractures – especially of the hip – are associated with longer hospital stay, permanent disability, and other complications such as infections. Bone fracture healing is a complex process and orthopaedic studies have been conducted to assess the effects of environmental factors such as smoking and nutrition on fracture healing. Evidence from human orthopaedic studies suggest that smoking negatively impacts fracture healing, as shown by longer healing times, higher rates of surgical non-union and post-operative complications. Evidence from experimental animal model studies suggest that dietary protein, calcium, phosphorous, and vitamin D have a positive influence on fracture healing, however, there is limited evidence on their impact based on human studies. Aims: The aim of this study is to assess the impact of smoking and calorie intake on the rate of bone fracture healing in a cohort of osteoporotic patients. Methods: This study is a non-blinded prospective cohort study of 500 osteoporotic patients recruited from the inpatient and outpatient fracture clinics in the Manchester Royal Infirmary. The rates of fracture healing of 250 smokers will be compared with 250 non-smokers matched by age, sex, ethnicity, BMI, and fracture classification. The calorie intakes of the non-smoking group will be assessed. The primary outcome measurement is time to union fracture healing. Secondary outcome measurements will be quality of life, duration of hospital stay, and presence of infections. The effect of smoking and calorie intake at a
- 3. The impact of smoking and calorie intake on bone fracture healing II cellular level is outside the scope of this study. Data will be analysed using an unpaired comparison test. Implications to public health and pharmacy: This research will help to emphasise the need for clinicians to make fracture patients become more aware of the negative effects of smoking and the importance of nutritional intake on the rate of fracture healing. Gaining a better understanding of the impact of calorie intake can possibly lead to the implementation of recommended nutritional intakes into guidelines on the management of fragility fractures. Optimisation of fracture healing requires a holistic approach from the multidisciplinary team and appropriate patient counselling on smoking and nutritional intake during a fracture can also help patients to further improve the rate of fracture healing so that they are able to return to their pre-fracture state of independence in performing day-to-day tasks, as soon as possible.
- 4. The impact of smoking and calorie intake on bone fracture healing III Table of contents Executive summary…………………………………………………………………..I 1 Introduction…………………………………………………………………….......1 1.1 Osteoporosis…………………………………………………………….1 1.2 Fragility Fractures……………………………………………………….1 1.3 Bone structure and function…………………………………………....2 1.4 Bone modelling and remodelling………………………………………4 2 Literature review …………………………...……………………………….…….6 2.1 Bone fracture healing………………………………………..…………6 2.2 Smoking and bone fracture healing…………………………………..8 2.3 Calorie intake and bone fracture healing………..……….…………10 2.4 Rationale for the study………..………………………………………11 3 Methods/Design………………………………………………………….………12 3.1 Study aims………………………….……………………………..……12 3.2 Study design…………...………………………………………….…...12 3.3 Study population......................................................................…...13 3.4 Research procedures………………………...…………….…………15 3.5 Ethics……………………………………………………………………18 3.6 Sample size calculation and data analysis…………………..……..19 3.7 Timeline of the study…………………………………………..………20
- 5. The impact of smoking and calorie intake on bone fracture healing IV 4 Discussion………………………………………………………...…………...…22 4.1 Limitations of the study…………………………..…………………...22 4.2 Impact of research………………………..…………………………...24 5 Acknowledgements……………..……………………………………………….26 6 References……………………………………………………………………….27 7 Appendices……………………………………………………………………….33 7.1 Appendix 1 – Brief information sheet for eligible patients…….…….33 7.2 Appendix 2 – Full information leaflet for participants………..………35 7.3 Appendix 3 – Consent form………………………………….….…….41 7.4 Appendix 4 – Self-completion questionnaire at baseline……...……43
- 6. The impact of smoking and calorie intake on bone fracture healing V Declaration “I understand the nature of plagiarism and that it is serious academic offence. I confirm that no material in the project has been plagiarised.” Signed: Richmond Arcillas Date: 06/05/2015
- 7. The impact of smoking and calorie intake on bone fracture healing 1 1. Introduction 1.1 Osteoporosis Osteoporosis causes approximately nine million fractures annually worldwide1 and more than 300,000 patients in the UK are admitted to secondary care with fragility fractures each year.2 Osteoporosis is a progressive systemic skeletal disease caused by an imbalance in the bone remodelling process resulting in weak, fragile bones. It is characterised by low bone mass, deterioration of bone micro-structure, and increased skeletal fragility and fracture risk. Fragility fractures can cause patients severe pain and disability thus affecting their quality of life; and are associated with an increased risk of morbidity and mortality.3 Direct medical costs of fragility fractures could potentially rise to £2.2 billion by 2025,4 mostly relating to hip fracture care, thus putting a huge strain on the UK National Health Service. The risk of osteoporosis increases with age but women are approximately four times more likely than men to develop the disease,5 mainly due to an increased rate of bone loss after menopause when the ovaries stop producing oestrogen.3,5,6 The problems associated with an ageing population is that the incidence of osteoporosis and fragility fractures will increase, especially for hip fractures, which is predicted to rise from 91,500 fractures in 2015 to 101,000 in 2020.2 1.2 Fragility fractures A ‘fracture’ is a medical term used to describe a broken or cracked bone. Fragility fractures result from mechanical forces that would not normally result in a fracture, known as low-level trauma.6 The World Health Organisation has
- 8. The impact of smoking and calorie intake on bone fracture healing 2 measured low-level trauma as forces equivalent to a fall from a standing height or less.3 There are a number of factors that can predispose an individual to fragility fractures. A major risk factor is reduced bone density, however, other risk factors include: age, sex, oestrogen deficiency, previous fractures, family history of osteoporosis, and the use of oral or systemic glucocorticoids.3 An individual’s lifestyle can also influence their risk of developing osteoporosis, such as lack of exercise, low calcium and vitamin D intake, smoking, and excessive alcohol consumption.5,6 Fragility fractures occur most commonly in the vertebrae (spine), proximal femur (hip), and distal radius (wrist), as well as in the humerus (arm), pelvis, ribs, and in other bones.3 Hip fractures are the most common in the elderly population and typically results from a fall.2 It is currently the biggest challenge in the epidemic of osteoporotic fractures: patients with a fractured neck of femur nearly always require hospitalisation, and are associated with a prolonged hospital admission – 20% of cases are fatal, 50% are permanently disabled, and only 30% of cases fully recover.2 1.3 Bone structure and function An adult human skeleton comprises of 206 bones which have a variety of functions. Firstly, the skeleton acts as a scaffold to provide structural support and to protect vital internal organs including the heart, brain, and lungs from damage. They also provide a site for muscles to attach in order to facilitate movement, and serve as a storage for various growth factors, cytokines, and minerals such as calcium and phosphate.7,8,9 The bones help maintain calcium
- 9. The impact of smoking and calorie intake on bone fracture healing 3 homeostasis and acid-base balance,9 and provide the right environment for the production of red and white blood cells within the bone marrow spaces through a process known as haematopoiesis.7,8,9 Bones are predominantly made up of calcium salts and other minerals, which are bound together by strong collagen (protein) fibres.5 Bones can be divided into two types: cortical and trabecular. Cortical bone, which comprises 80% of the skeleton, is dense and forms the thick outer part of the bone surrounding the marrow space, thus providing mechanical strength and protection.9,10 In contrast, trabecular bone, which forms the other 20% of the skeletal mass, is composed of a spongier, honeycomb-like structure comprising of trabecular plates and rods distributed within the bone marrow compartment.9 Trabecular bone has a higher turnover rate and is more metabolically active compared to cortical bone, however, both can provide supplies of mineral at times of deficiency.10 The ratio of cortical and trabecular bones vary in composition between various locations, with osteoporotic fractures occurring more frequently at sites with greater trabecular bone composition,7 such as the vertebra, proximal femur, and distal radius.3 The skeleton is a complex, living, metabolically active organ that is continuously adapting throughout life and undergoes constant regeneration (bone turnover), through bone modelling (construction) and remodelling (reconstruction).7,11 These mechanisms help to repair any micro-damage to the bones and maintain calcium homeostasis,7 enabling us to achieve peak bone density during growth and to preserve it thereafter in adulthood.12
- 10. The impact of smoking and calorie intake on bone fracture healing 4 1.4 Bone modelling and remodelling Bone modelling is the process by which bones adapt their overall shape and structure in response to mechanical forces or physiological influences, resulting in the gradual adjustment of the skeleton to the forces it encounters.9,11 Bone remodelling is the lifelong process by which bone is continuously renewed in order to maintain bone strength and mineral homeostasis.9 This homeostatic equilibrium involves the continuous resorption of old bone tissue by osteoclasts, replacement with newly synthesised bone tissue matrix by osteoblasts, and subsequent mineralisation of the matrix to form new bone.5,9 This process not only helps to prevent the accumulation of old bone by repairing micro-damages in the bone matrix,10 but also plays an important role in maintaining plasma- calcium homeostasis.9,10 The remodelling cycle comprises of four phases: activation, resorption, reversal, and formation. This cycle is composed of a tightly coupled group of osteoclasts and osteoblasts,9 and is mediated by osteocytes which are highly abundant throughout the skeleton.7 It is suggested by Seeman and Delmas12 that apoptosis of osteocytes produce the signals necessary to initiate remodelling and thus targets a particular site that is in need of repair. The activation phase involves the interaction between osteoclast and osteoblast pre-cursor cells in order to accelerate osteoclastogenesis (production of osteoclasts).13,14 The initial activation of osteoblast pre-cursor cells (known as lining cells) result from various triggers including: micro- fractures, and the presence of insulin growth factor-I, tumour necrosis factor-α, parathyroid hormone, and interlukin-6 in the bone microenvironment.13 This
- 11. The impact of smoking and calorie intake on bone fracture healing 5 leads to an increase in expression of Receptor Activator of Nuclear κB Ligand (RANKL) on the surface of their own cells.13 RANKL then binds with its receptor, Receptor Activator of Nuclear κB (RANK), which are expressed on osteoclast precursor cells, in order to enhance the nuclear κB signalling pathway.10,13 This RANKL/RANK interaction between coupled osteoblast and osteoclast pre- cursor cells trigger the differentiation, migration, and fusion into large multinucleated osteoclasts.10,14 Once differentiated, osteoclast cells adhere on to the mineralised bone surface and initiate resorption by releasing lysosomal enzymes such as cathepins K, and hydrogen ions, which dissolves bone at low pH.13,14 The reversal phase transitions bone resorption to bone formation. This phase is not well understood but it is thought to involve the recruitment of mononuclear cells onto the bone surface in order for new bone to be formed.9,13,14 Finally, during the formation phase, osteoblast cells are recruited to the resorbed area and fill the cavity with new bone matrix that is subsequently mineralised, in order to complete the bone remodelling cycle.13 In osteoporosis, coupling is lost which leads to a reduced osteoblast activity and/or an increased osteoclast activity.13 This imbalance between bone resorption and bone formation leads to a lower peak bone mass,7 which progressively worsens with age, with the highest rate of bone loss occurring after the age of 65 years.15
- 12. The impact of smoking and calorie intake on bone fracture healing 6 2. Literature review 2.1 Bone fracture healing Bone fracture healing is a complex physiological process that involves various cell types and proteins coordinated to regenerate and unite fractures. In order to assess the impact of certain environmental factors such as smoking and calorie intake on bone fracture healing, we need to have an understanding of the physiological processes involved in fracture healing. The stages of fracture healing was first classified by John Hunter in the 1700s and is still used as the main framework for describing bone fracture healing. It initially involved four distinct overlapping stages: inflammation, soft callus, hard callus, and remodelling.16 Current understanding now divides fracture healing into three stages: inflammation, repair, and remodelling;16,17,18,19-20 which underpins the same biology as Hunter’s four-stage classification. The inflammatory stage occurs alongside wound healing in response to trauma.16 Firstly, a haematoma develops at the fracture site within the first few hours and days following an injury.17 Osteocytes at the fracture ends die as a result of nutrient deprivation and is noted to play a passive role in repair.16 Inflammatory cells such as macrophages, lymphocytes, and leucocytes are then recruited into the fracture site and release pro-inflammatory cytokines which induce extracellular bone matrix synthesis, stimulate the development of new blood vessels (angiogenesis), and recruit endogenous fibroblasts and mesenchymal cells.20 These recruited mesenchymal cells then differentiate into specialised cells, i.e. fibroblasts, chrondoblasts, and osteoblasts, which help build new connective tissue, cartilage, and bone tissue, respectively, on the
- 13. The impact of smoking and calorie intake on bone fracture healing 7 fracture gap.16,18 Osteoclasts also play a role in removing damaged material through resorption of dead calcified bone.16 The reparative stage begins several days after the initial inflammatory response.16 Fibroblasts begin to lay down connective tissue which helps to support angiogenesis.17 As this progresses, a collagen matrix is laid down while new bone matrix is formed and subsequently mineralised, leading to the formation of a soft, new bone substance known as a soft callus, around the fracture site.16,17 This soft callus is very weak during the first 4 to 6 weeks of the healing process and therefore requires adequate protection.17 As the bone weaves together over the next 6-12 weeks, the soft callus eventually solidify and harden into a hard callus.18 The final remodelling stage completes fracture healing by restoring the bone to its original shape, structure, and mechanical strength.17 In this stage, osteoclasts slowly resorb the callus until the original shape of the cortex is restored and osteoblast cells lay down new bone where it is needed, in order to remodel the woven bone into stronger lamellar bone.22 A study in an osteoporotic rat model produced by ovariectomy and low calcium diet found that osteoporosis influences the late period of fracture healing.23 Rats were monitored over a 12 week period and at 12 weeks, newly generated bones in the group with osteoporosis showed a decreased bone mineral density on the fracture site compared to the control group. Furthermore, the authors concluded that oestrogen deficiency and low calcium intake do not markedly affect the early healing process but largely effect the later stage of fracture healing.
- 14. The impact of smoking and calorie intake on bone fracture healing 8 In contrast, a more recent study has been conducted in a rat osteoporotic model which demonstrated the influence of bone loss on the early phase of fracture healing.24 The authors found that under osteoporotic conditions, fracture callus healing was delayed alongside a reduction in callus strength. Although this study provides evidence on the effect of excessive bone loss towards the early fracture healing process in osteoporotic rats, its long-term effects have not been evaluated. Differences in conclusions from these studies could be due to differences in the length of monitoring and the outcomes measured, but both studies suggest that osteoporosis could alter the bone fracture healing process. 2.2 Smoking and bone fracture healing There have been a number of studies documenting the negative effect of smoking on the healing process and fracture-related morbidities. Patel et al.25 conducted a systematic review of 17 orthopaedic studies, of which, 13 concluded that smoking has a negative influence on fracture healing. For instance, five tibia studies found that smokers took significantly longer to heal than non-smokers.26,27,28,29-30 A comparison study by Brown et al.31 investigating the relationship between smoking and the rate of surgical non-union (i.e. permanent failure of healing following a fracture) in 50 patients that undertook spinal fusion reported a higher rate of surgical non-union in smokers than the non-smoking control group (40% vs 8%). The findings were statistically significant and appeared to be independent of age, sex, or race. The authors hypothesised that this higher rate of non-union in smokers may be due to blood gas levels, as smokers showed a significant deficiency in the mean p02 (78.5%; normal range: 95-97%) and O2
- 15. The impact of smoking and calorie intake on bone fracture healing 9 saturation levels (92.9%; normal range: >95%) because of an increased carbon monoxide and smoking-induced arterial constriction.31,32 The effects of smoking on the healing time is also shown on a study focusing on tibia shaft fractures by Schmitz et al.33 In this study, a higher rate of union healing at follow-up was observed in non-smokers than smokers (84% vs 58%). Also, 103 out of 146 patients had a complete follow-up to union but in this group of patients, the average time of clinical healing was much longer in patients who smoked compared to the patients who did not smoke (269 days vs 136 days). Interestingly, statistical differences in the observed healing rates were observed for those receiving intramedullary or external fixation, but not in patients treated with cast immobilisation. Nonetheless, the tibias of smokers treated with cast immobilisation took 62% longer to heal. The authors concluded that patients who smoke and require treatment with intramedullary nailing or external fixation require more time to heal than those who do not smoke. Further studies have also observed a higher frequency of post-operative complications such as delayed healing, infection, and non-union fracture healing among smokers.34 Studies conducted by Folk, et al.36 and Abidi, et al.,37 which both investigated calcaneal (heel bone) fractures, have observed a longer healing period post-surgery in patients that smoked. Furthermore, there was a higher rate of post-operative local wound complications such as sloughing or deep infection in patients who smoked. Therefore, the studies concluded that smoking should be contraindicated in surgery.34
- 16. The impact of smoking and calorie intake on bone fracture healing 10 2.3 Calorie intake and bone fracture healing A calorie is defined as a unit of energy supplied from food.38 Calories are contained in all sources of food, including carbohydrates, fats, sugars, or proteins. There have not been many studies, especially in humans, investigating the association of calorie intake and fracture healing. However, experimental animal studies39,40,41 in the 1980s have looked at the effect of dietary protein and mineral on fracture healing. Einhorn, Bonnarens and Burstein39 showed that dietary protein, calcium, phosphorous, and vitamin D are important in fracture healing; and Hughes, et al.40 found that dietary supplementation with protein positively influenced bone mineralisation, body mass, and muscle mass in malnourished animals. The study by Pollak et al.41 in the injured rat model found that the group which had a low protein diet resulted in significantly weaker and stiff calluses despite adequate calorie intake; however, they also did not find a significant improvement in fracture healing with the high protein diet group. In humans, a study consisting of 490 hip-fracture patients reported that an albumin level of <3.5 gs/100ml was predictive for increased duration of hospital stay and in-hospital mortality following a fracture.42 This study found that patients with abnormal albumin and total lymphocyte count were 2.9 times more likely to stay in hospital for more than two weeks and 3.9 times more likely to die within one year post-surgery. However, these parameters were not predictive for patients developing post-operative complications. Malnourishment seem to negatively impact on the bone fracture healing process, but more human studies are required in gain a better understanding
- 17. The impact of smoking and calorie intake on bone fracture healing 11 of the clinical implications that deficiencies in nutrition will have on the rate of fracture healing in humans. 2.4 Rationale for the study There is a lot of evidence from human studies which assess the impact of smoking on bone fracture healing. The effects of smoking is thought to be due to vasoconstriction and platelet activation by nicotine, hypoxia-inducing effect of carbon monoxide, and the inhibition of oxidative metabolism by hydrogen cyanide.43 In contrast, limited studies have been conducted with regards to the impact of calorie intake, most of which were conducted in animal models. Various studies implied that adequate nutrition is required, especially in calcium, phosphorous, vitamin C and D, and protein levels, in order to aid the bone fracture healing process. Although it is unlikely that the majority of patients presenting with fractures will be malnourished, there is a higher likelihood that the elderly population presenting with fragility fractures will have some form of nutritional deficiency. It is therefore important to assess the nutritional intake of these patients in order to optimise the rate of fracture healing and to minimise complications. This research study will help to strengthen our current knowledge of the impact of smoking, as well as find new evidence of an association between calorie intake and bone fracture healing, so that health practitioners can help to optimise the management of fractures not only in osteoporotic patients, but also in the wider population.
- 18. The impact of smoking and calorie intake on bone fracture healing 12 3 Methods/Design 3.1Study aims To determine the impact of smoking and calorie intake on the rate of bone fracture healing in a cohort of osteoporotic patients. 3.2 Study design This study is a non-blinded prospective cohort study of 500 patients presenting with a fragility fracture who have been admitted to the out-patient fracture clinics or in-patient trauma and orthopaedic department in the Manchester Royal Infirmary (MRI) hospital. The primary outcome measurement is time to union fracture healing. Participants must provide written consent to be observed for 24 months or until they reach the primary outcome. This study will use the definitions used in a study conducted by Schmitz et al.,33 where clinical fracture union is defined as the ability to fully bear weight without pain at the fracture site, and radiographic union is the evidence of bridging of 3-4 cortices on standard antero-posterior lateral views. Delayed union is defined as a fracture taking >18 weeks to heal44 and non-union is defined as failure to achieve union within the final follow-up period. The total length of follow-up is based on a systematic review of 17 orthopaedic studies conducted by Patel et al.25 which identified a mean length of follow-up which ranged from 21.6 months to 41 months. Secondary outcomes will also be measured, specifically the presence of soft- tissue and deep post-surgical infections, duration of hospital stay, and quality of life. This is in order to gain a wider scope of the impact of smoking and calorie
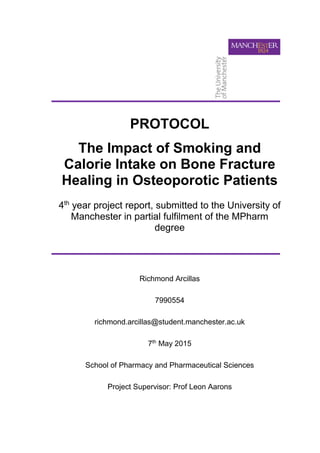
- 19. The impact of smoking and calorie intake on bone fracture healing 13 intake with regards to complications in the patient’s recovery, similar to other studies conducted by Adams et al.,27 Folk, et al.,36 and Abidi, et al.37 3.3 Study population The study will work closely with the Central Manchester University Hospitals Trust (CMFT) and the recruitment of volunteers will take place in the MRI hospital, Manchester. Orthopaedic surgeons and radiologists in the MRI hospital will be recruited for this study and will act as the gatekeepers. Eligible patients will be identified by the participating orthopaedic surgeons using an inclusion and exclusion criteria (see Figure 1). They will then be contacted initially in hospital and will be verbally informed of the study and receive a brief information sheet (Appendix 1). Patients who are interested in volunteering in the study will then be provided with full written information regarding the study, including: the purpose of the study, their rights, the procedures of data collection and how their data will be used, as well as reimbursement at follow- up periods (Appendix 2). Patients are also required to complete a written consent form (Appendix 3) and hand back to the research team in order to participate in the study. In order to be eligible, patients must have a diagnosed history of osteoporosis and have a current fragility fracture of the femur, distal radius, or knee as these will be the fractures of interest in the study. Controls will be appropriately matched by age, sex, ethnicity, BMI, and fracture classification. Patients will not be eligible for the research study if they refuse to provide written informed consent. Patients with co-morbidities including diabetes mellitus, anaemia, peripheral vascular disease, and hypothyroidism will also be
- 20. The impact of smoking and calorie intake on bone fracture healing 14 excluded as these have been found to further increase the risk of non-union in patients.45 Similarly, patients on long-term corticosteroid therapy and regular non-steroidal anti-inflammatory drug (NSAID) therapy will also be excluded as these too can elongate the healing process.45 Figure 1. Flow diagram defining the population of the study. Admission to out-patients fracture clinic (MRI). Admission to in-patients trauma and orthopaedic department (MRI). Confirmation of fracture cases by radiography. Inclusion criteria: Known diagnosis of osteoporosis. Current fracture of the femur, knee, or distal radius. Smokers and non- smokers. Exclusion criteria: Refusal to provide written informed consent. Other upper body fractures including: pelvis, humerus, and ribs. Other lower leg fractures, including foot and ankle. Diabetes mellitus, anaemia, peripheral vascular disease, hypothyroidism. Regular use of oral or systemic corticosteroid and non-steroidal anti- inflammatory drugs. 250 controls: identification of non-smoker patients with osteoporosis during the same study; matched with cases by age (2 year bands), sex (M/F), ethnicity, BMI, and fracture classification. 250 cases who are current smokers. Measurement of calorie intake (total calories per week). Collect information on confounders and effect modifiers, surgical or non-surgical interventions (e.g. cast immobilisation or intramedullary rod fixation), and co-morbidities, using PMR records. Measurement of smoking status (cigarettes per day). Provision of written informed consent. Primary outcome: time to union fracture healing. Secondary outcomes: quality of life, duration of hospital stay, and post-surgical infections.
- 21. The impact of smoking and calorie intake on bone fracture healing 15 3.4 Research procedures The study will comprise of an initial baseline measurement (during hospital admission), T2 follow-up (two weeks after discharge) and every 3 months thereafter for 24 months from the date of discharge (T3-T10) or until union fracture healing is achieved (see Table 1). This is similar to a study conducted by Adam et al.27 which had a mean follow-up of 21.6 months, however, trimonthly assessments will help to reduce inconvenience for the participants but still enable close monitoring of clinical outcomes. Participants will be reminded about their follow-up a week in advance by telephone call. The primary outcome of fracture union will be assessed using clinical and radiographic data; and the length of hospital stay due to fracture and presence of infections will also be measured. The participant’s study period will end at T10 follow-up or once union fracture healing has been confirmed. At baseline, the participants’ age, sex, BMI, co-morbidities, intervention (surgical or non-surgical) and fracture classification will be recorded by participating orthopaedic surgeons, using the patient’s most recent patient medical (PMR) and radiographic records. Only the gatekeepers may have access to these records. Furthermore, the participants will need to complete a questionnaire to assess their smoking history (Appendix 4). The calorie intake will not be recorded on baseline but will be recorded on the subsequent follow- up periods (T2-T10). This is because the calorie intake during the fracture, not before, is the point of interest in this study. For convenience, the questionnaire will be done via an electronic tablet and participants will be provided with an electronic diary to keep a record of their food intake and the amounts of cigarettes smoked daily. Participants will be reimbursed with £35 for the T2
- 22. The impact of smoking and calorie intake on bone fracture healing 16 follow-up and trimonthly follow-ups (T3-T10) and any additional catering and travelling expenses will be paid for, for their time and effort. Table 1. Data collection and reimbursement at relative time points. At two weeks follow-up after discharge (T2) and every trimonthly follow-up (T3- T10), participants will be assessed by a participating fully-trained diagnostic radiologist in the MRI hospital. They will also be required to complete the questionnaire on the same day. In addition, the patient’s current medications will be checked by the orthopaedic surgeons every 6 months using their PMR to look for any changes in medications made in between the follow-up periods. Baseline T2 T3 T4 T5 PMR Questionnaire (smoking status) Electronic diary Radiography Questionnaire £35 Radiography Questionnaire £35 PMR Radiography Questionnaire £35 Radiography Questionnaire £35 T6 T7 T8 T9 T10 PMR Radiography Questionnaire £35 Radiography Questionnaire £35 PMR Radiography Questionnaire £35 Radiography Questionnaire £35 Radiography Questionnaire £35
- 23. The impact of smoking and calorie intake on bone fracture healing 17 There will be 250 cases in each primary arm of the study, based on their smoking status (see Figure 2). Non-smokers will form the comparison group and will be defined as patients who stated that they had never smoked or had stopped smoking over six months ago. Smokers will be further divided into groups based on the average amount of cigarettes they smoke daily to allow for comparison of the outcomes between groups with varying numbers of cigarettes smoked. Participants will be asked to record the number of cigarettes they smoke each day using the electronic diary provided. The non-smoker arm will be further divided into groups based on their calorie intake. The calorie intake of the non-smoking group will be considered in this study as this will help to minimise any confounding effects of current smoking and enable comparison between groups with varying calorie intakes. Participants will be asked to record the type of food they consume each day using the electronic diary, and if possible, the number of calories they contain. The foods where calories have not been quantified will be searched up on a standard easy-to-use food database46 to enable their calories to be measured. The same database will be used throughout the whole study. 500 participants 250 smokers 250 non-smokers Primary and secondary outcomes Number of cigarettes smoked daily Amount of calories (kcal) consumed daily Primary and secondary outcomes Figure 2. Number of participants in each arm of the study.
- 24. The impact of smoking and calorie intake on bone fracture healing 18 3.5 Ethics The study will be submitted to the Northwest Centre for Research Ethics Committee’s for approval of conducting the research at the Manchester Royal Infirmary. Participants who agree to partake in this study must have the capacity to give informed consent. All questionnaires, clinical and radiographic data, and patient medical records (PMR) will be kept confidential throughout and after the study. Only the participating orthopaedic surgeons and radiologists, who will act as gatekeepers, will have access to the PMR records and relay the relevant data back to the research team for the purpose of the study. Participant information details will also be anonymised throughout and after data analysis. Instead, each participant will be given a randomly generated identification number. Participants and the participating orthopaedic surgeons and radiologists will also be given contact details of the research team if they wish to ask any questions at any point in time relating to the study. Participants will remain on their usual medications throughout the study, including any medications and supplementations indicated for osteoporosis as per NICE guidelines. However, participants will be told not to purchase and consume any over-the-counter NSAID such as ibuprofen, or aspirin for pain relief; however, this cannot be fully controlled when patients have been discharged. Furthermore, participants have the right to withdraw at any point of the study; however, they will receive no further reimbursement and their data may not be used.
- 25. The impact of smoking and calorie intake on bone fracture healing 19 3.6 Data analysis and sample size calculation The sample size for this study was calculated using equation 1 (see below),47 in order to detect a predicted 50% reduction of clinical union in smokers compared to non-smokers. Using a population size of 300,000 and a desired confidence level of 95% with a 5% margin of error, a minimum of 384 participants will be required in order to produce a power of 80%. An additional 116 participants will be recruited in this study to account for any drop outs or losses to follow-up during the study period, leading to a total of 500 participants. Two statisticians will also be recruited to perform the data analysis. An unpaired comparison test will be used to analyse the data in order to compare results between the non-smoking comparison group and the various smoking groups; and between the various calorie-intake groups within the non-smoking comparison group. Sample size = 𝒛 𝟐×𝒑(𝟏−𝒑) 𝒆 𝟐 𝟏 +( 𝒛 𝟐 ×𝒑(𝟏−𝒑) 𝒆 𝟐 𝑵 ) (Equation 1) Z = z-score(1.96 at 95% confidence level)48 P = response distribution (50%; 0.5) e = margin of error (5%; 0.05) N = population size (300,000) Desired confidence level z-score 80% 1.28 85% 1.44 90% 1.65 95% 1.96 99% 2.58
- 26. The impact of smoking and calorie intake on bone fracture healing 20 3.7 Timeline The study will last for 36 months in total. Recruitment of volunteers will begin after the CPRD and University approval, and will last for 12 months after taking into consideration the limited number of hospital beds. This is to ensure that there is enough time to recruit 500 volunteers and to receive written informed consent. A summary of the timescale of the study is shown in Table 2 below. Table 2. Summary of the study timescale. Data collection will begin approximately one month after the start of the recruitment process, or as soon as the participant provides informed consent, in order for baseline measurements to be taken during hospital admission. This will continue for a maximum of 24 months after discharge or until the primary Action Month 2 4 6 8 10 12 14 16 18 CPRD and University protocol and approval Recuitment Data collection Data cleaning and management Data analysis Report write-up and additional analysis Final publication Action 20 22 24 26 28 30 32 34 36 CPRD and University protocol and approval Recuitment Data collection Data cleaning and management Data analysis Report write-up and additional analysis Final publication
- 27. The impact of smoking and calorie intake on bone fracture healing 21 outcome of union fracture healing has been established. Data cleaning and management will run alongside data collection to minimise compilation of bulks of unorganised data at the end of data collection. Considering the amount of data that is being collected, data analysis will overlap the last four months of data collection so that analysis of data for the participants who have finished can begin, and will continue for a further two months after the end of the data collection process. Lastly, the report write-up and final publication will require approximately four months to complete.
- 28. The impact of smoking and calorie intake on bone fracture healing 22 4 Discussion 4.1 Limitations of the study Cohort studies require a large study population that need to be observed for a long period of time. This study is therefore expensive and the 24 month follow- up period requires long-term commitment from the participants and naturally has a higher rate of dropouts and chance of losing participants to follow-up. Furthermore, since the study population is observed prospectively, there will be unknown outcomes which would be difficult to predict and control. For instance, patients on long-term corticosteroids and regular NSAID treatment have been excluded from the study; however, participants may have their medications changed by their physicians throughout the study period, which could affect the outcome of results. It is also difficult to account for patients on nicotine replacement therapy (NRT) or have decided to switch to NRT as nicotine is thought to affect fracture healing.43 The non-smoking group is also defined based on the assumption that cessation for over 6 months after long-term smoking do not have any long-lasting or long-term effects on the bone fracture healing process, and therefore, this assumption has the possibility of affecting the results. The study population is not randomised and so it will be difficult to avoid confounding. Additionally, the study is subject to selection bias and variation between groups of participants cannot be controlled, especially for co- morbidities, which can potentially lead to biased results. The participants are not blinded in this study, which makes it difficult to control bias in the outcomes. Participants having full knowledge of what the research is assessing may be
- 29. The impact of smoking and calorie intake on bone fracture healing 23 enough to change their normal behaviours, but it is also difficult to blind participants with this particular study design. Furthermore, this study is limited to osteoporotic patients and is therefore not representative of the general population presenting with fractures. With regards to data collection, data gathered from the questionnaire could be subject to recall bias since retrospective data is used on the exposure of smoking and calorie intake. Since information about dietary intake is completely dependent on self-reports, it is difficult to assess the accuracy, as participants may not be able to record their daily intake on a regular basis or may be underreporting or underestimating the amount they consume. This means that the data may be inconsistent and unreliable. To help with the monitoring process, participants will be provided with an electronic diary. However, when combined with the length of follow-up, this strategy can potentially backfire and become tedious, thus discouraging participants from accurately monitoring their calorie intakes and smoking status, and possibly even contribute to the dropout rates or loss to follow-up. The margin of error from the secondary groups that will have their calorie intake assessed will also be higher in comparison to the primary groups of smoker vs non-smoker, since that particular group will be smaller. Lastly, patients attending the pre-operative clinic for elective surgery may be advised to stop or reduce smoking which could misrepresent the exposure on the study population and thus affect results. On the other hand, it is unethical to tell participants to continue smoking or drinking, therefore it is difficult to fully isolate the effect of the exposure on the outcome.
- 30. The impact of smoking and calorie intake on bone fracture healing 24 4.2 Impact of research Various studies have found a negative correlation between smoking and bone fracture healing in fracture patients. In contrast, there has not been a lot of research on the clinical impact of calorie intake on bone fracture healing in humans. Patients undergoing surgery for fractures are advised not to smoke on the morning of general surgery,29 however, there is a lack of advice given with regards to calorie or nutritional intake. Relating this to orthopaedics, it is important that factors that can compromise the process of fracture healing are minimised in order to optimise the management of fractures. This study will be one of the largest studies to be conducted in a cohort of osteoporotic patients. This can provide the foundation for the development of human studies to assess the impact of these two exposures, especially of calorie intake and nutrition, on the rate of bone fracture healing Conducting this study will help to provide further evidence on the negative impact of smoking to the rate of fracture healing in patients diagnosed with osteoporosis. There is a lack of understanding on the clinical impact of calorie intake on bone fracture healing; therefore, this study will help contribute new evidence towards the impact of calorie consumption on bone fracture healing in humans. Gaining a better understanding on the impact of these two environmental factors can lead to the implementation of recommended nutritional intakes into hospital or local guidelines on the management of fragility fractures. Optimisation of fracture healing requires a holistic approach from the multidisciplinary team and appropriate patient counselling on the risks of
- 31. The impact of smoking and calorie intake on bone fracture healing 25 smoking and the benefits of nutritional intake during a fracture can also help to improve the rate of fracture healing so that patients are able to quickly return to their pre-fracture state of independence in performing day-to-day tasks.
- 32. The impact of smoking and calorie intake on bone fracture healing 26 5 Acknowledgements I wish to thank Professor Leon Aarons from the University of Manchester for his guidance with writing this research protocol.
- 33. The impact of smoking and calorie intake on bone fracture healing 27 6 References 1) Johnell O, Kanis JA (2006). An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporosis International 17: 1726–33. 2) British Orthopaedic Association. The care of patients with fragility fracture. Second Edition. 2007. [cited 2015 Mar 16]. Available from: http://www.fractures.com/pdf/BOA-BGS-Blue-Book.pdf 3) National Institute for Health and Clinical Excellence. NICE [Internet]. London: National Institute for Health and Clinical Excellence; [updated 2015 Jan; cited 2015 Mar 16] Available from: https://www.nice.org.uk/guidance/cg146/chapter/introduction#ftn.footno te_2 4) Burge RT, Worley D, Johansen A, et al. The cost of osteoporotic fractures in the UK: projections for 2000–2020. Journal of Medical Economics 4: 51–52. 5) Arthritis Research UK [Internet]. 2013 [cited 2015 Mar 18]. Available from: http://www.arthritisresearchuk.org/arthritis- information/conditions/osteoporosis.aspx 6) National Osteoporosis Society. All about osteoporosis: A guide to bone health, fragile bones and fractures [Internet]. 2014 [cited 2015 Mar 18]. Available from: https://www.nos.org.uk/health- professionals/~/document.doc?id=1848 7) Rokib T, Bairstow D. Osteoporosis diagnosis and risk assessment. Clin phar 2014 May; 6: 87-91.
- 34. The impact of smoking and calorie intake on bone fracture healing 28 8) Blood and bone: two tissues whose fates are intertwined to create the hematopoietic stem-cell niche. Taichman RS Blood. 2005 Apr 1; 105(7):2631-9. 9) Clarke B. Normal Bone Anatomy and Physiology. Clin K Am Soc Nephrol 2008 Nov; 3(3): 131-39. 10) Hadjidakis DJ, Androulakis II. Bone remodelling. Ann N Y Acad Scie, 2006 Dec; 1092: 385-96. 11) Seeman E. Bone modelling and remodelling. Crit Rev Eukaryot Gen Expr 2009; 19(3): 219-33. 12) Seeman E, Delmas PD. Bone quality – the material and structural basis of bone strength and fragility. New Eng Jour of Med 2006; 354: 860-63. 13) Rucci N. Molecular biology of bone remodelling. Clin Cases Miner Bone Metab, 2008 Jan-Apr; 5(1): 49-56. 14) Raisz LG. Physiology and pathophysiology of bone remodelling. Clin Chem, 1999 Aug; 45(8): 1353-58. 15) Manolagas SC. Pathogenesiss of osteoporosis [Internet]. Uptodate, Inc.; 2015 [updated 2015 Jan 5; cited 2015 Mar 6]. Available from: www.uptodate.com/contents/pathogenesis-of-osteoporosis 16) Marzona L, Pavolini B. Play and players in bone fracture healing match. Clin Cases Miner Bone Metab. 2009 May-Aug; 6(2): 159-62. 17) Kalfas IH. Principles of Bone Healing. Neurosurg Focus. 2001; 10(4). 18) Brown SE. How to Speed Fracture Healing. [Internet]. New York: Center for Better Bones; [updated 2009; cited 2015 Mar 06]. Available from: http://www.betterbones.com/bonefracture/speedhealing.pdf
- 35. The impact of smoking and calorie intake on bone fracture healing 29 19) Einhorn TA. The Cell and Molecular Biology of Fracture Healing. Clin Ortho. 1998 Oct; 355: 7-21. 20) McKibbin B. The biology of fracture healing in long bones. J Bone Joint Surg Br. 1978 May; 60-B(2): 150-62. 21) Feghali CA, Wright TM. Cytokines in acute and chronic inflammation. Front Bioscis. 1997;2:12–26. 22) Marsh, DR and Li, G. The biology of fracture healing: Optimising outcome. British Medical Bulletin. 1999; 55(4):856-869. 23) Kubo T, Shiga T, Hashimoto J, Yoshioka M, Honjo H, Urabe M, Kitajima I, Semba I, Hirasawa Y. Osteoporosis influences the late period of fracture healing in a rat model prepared by ovariectomy and low calcium diet. J Steroid Biochem Mol Biol. 1999 Mar; 68(5-6): 197-202. 24) Namkung-Matthai H, Appleyard R, Jansen J, Hao Lin J, Maastricht S, Swain M, Mason RS. Murrell GAC, Diwan AD, Diamond T. Osteoporosis influences the early period of fracture healing in a rat osteoporotic model. Bone. 2001 Jan; 28(1): 80-86. 25) Patel RA, Wilson RF, Patel PA, Palmer RM. The effect of smoking on bone fracture healing: A systematic review. Bone Joint Res. 2013 Jun; 2(6): 102-11. 26) Schmitz MA, Finnegan M, Natarajan R, Champine J. Effect of smoking on tibial shaft fracture healing. Clin Orthop Relat Res. 1999 Aug; (365): 184-200. 27) Adams CI, Keating JF, Court-Brown CM. Cigarette smoking and open tibial fractures. Injury. 2001 Jan; 32(1): 61-65.
- 36. The impact of smoking and calorie intake on bone fracture healing 30 28) Gaston MS, Simpson AHRW. Inhibition of fracture healing. J Bone Joint Surg Br. 2007 Dec; 89-B(12): 1553-60. 29) W-Dahl A, Toksvig-Larsen S. Cigarette smoking delays bone healing: a prospective study of 200 patients operated on by the hemicallotasis technique. Acta Orthop Scand 2004;75:347–351. 30) W-Dahl A, Toksvig-Larsen S. No delayed bone healing in Swedish male oral snuffers operated on by the hemicallotasis technique: a cohort study of 175 patients. Acta Orthop 2007;78:791–794. 31) Brown CW, Orme TJ, Richardson HD. The rate of pseudoarthrosis (surgical non-union) in patients who are smokers and patients who are nonsmokers: a comparison study. Spine (Phila Pa 1976). 1986 Nov; 11(9): 942-3. 32) Haverstock BD, Mandracchia VJ. Cigarette smoking and bone healing: implications in foot and ankle surgery. J Foot Ankle Surg. 1998 Jan-Feb; 37(1): 69-74. 33) Schmitz MA, Finnegan M, Natarajan R, Champine J. Effect of smoking on tibial shaft fracture healing. Clin Orthop Relat Res. 1999 Aug; (365): 184-200. 34) Abidi NA, Dhawan S, Gruen GS, Vogt MT, Conti SF: Wound-healing risk factors after open reduction and internal fixation of calcaneal fractures. Foot Ankle Int 1998;19:856–861. 35) Buckley RE, Tough S. Displaced intra-articular calcaneal fractures. J Am Acad Orthop Surg. 2004 May-Jun; 12(3): 172-78.
- 37. The impact of smoking and calorie intake on bone fracture healing 31 36) Abidi NA, Dhawan S, Gruen GS, Vogt MT, Conti SF: Wound-healing risk factors after open reduction and internal fixation of calcaneal fractures. Foot Ankle Int 1998;19:856–861. 37) Folk JW, Starr AJ, Early JS: Early wound complications of operative treatment of calcaneus fractures: Analysis of 190 fractures. J Orthop Trauma 1999; 13: 369–372. 38) Centers for Disease Control and Prevention [Internet]. Atlanta; 2015 [updated 2014 Jan 15; cited 2015 May 01]. Available from: http://www.cdc.gov/healthyweight/calories/ 39) Einhorn TA, Bonnarens F, Burstein AH. The contributions of dietary protein and mineral to the healing of experimental fractures. A biomechanical study. J Bone Joint Surg Am. 1986 Dec; 68(9): 1389-95. 40) Hughes MS, Kazmier P, Burd TA, Anglen J, Stoker AM, Kuroki K, Carson WL, Cook JL. Enhanced fracture and soft-tissue healing by means of anabolic dietary supplementation. J Bone Joint Surg Am. 2006 Nov; 88(11): 2386-94. 41) Pollak D, Floman Y, Simkin A, Avinezer A, Freund HR. The Effect of Protein Malnutrition and Nutritional Support on the Mechanical Properties of Fracture Healing in the Injured Rat. J Parenter Enteral Nutr. 1986 Nov; 10(6): 564-67. 42) Koval KJ, Maurer SG, Su ET, Aharonoff GB, Zuckerman JD. The effects of nutritional status on outcome after hip fracture. J Orthop Trauma 1999;13:164-9. 43) Sloan A, Hussain I, Maqsood M, Eremin O, El-Sheemy M. The effects of smoking on fracture healing. Surgeon. 2010 Apr; 8(2): 111-6.
- 38. The impact of smoking and calorie intake on bone fracture healing 32 44) Ellis H. The Speed of healing after fracture of the tibial shaft. J Bone Joint Surg Br. 1958 Feb; 40-B(1): 42-46. 45) Gaston MS, Simpson AHRW. Inhibition of fracture healing. J Bone Joint Surg Br. 2007 Dec; 89-B(12): 1553-60. 46) CalorieKing [Internet]. CalorieKing Wellness Solutions, Inc. 2015 [cited 06/05/2015]. Available from: http://www.calorieking.com/foods/ 47) Sample size calculator [Internet]. SurveyMonkey 2015 [cited 2015 Apr 16]. Available from: https://www.surveymonkey.com/blog/en/sample- size-calculator/
- 39. The impact of smoking and calorie intake on bone fracture healing 33 7 Appendix 7.1 Appendix 1 – Brief information sheet for eligible patients
- 40. The impact of smoking and calorie intake on bone fracture healing 34 The impact of smoking and calorie intake on bone fracture healing Hello, we are conducting a research study in the Manchester Royal Infirmary Hospital to assess the impact of smoking and calorie intake on the rate of bone fracture healing. We are looking for 500 volunteers with osteoporosis who are presenting with a current fracture of the hip, wrist, or knee. You have been given this brief information sheet because you are eligible to participate in this study. The study will comprise of periodic follow-ups at the Manchester Royal Infirmary Hospital after discharge in order to observe the progress of your fracture healing and to complete a questionnaire. We are also interested in your weekly calorie intake and smoking status as we are assessing their impact on the rate of bone fracture healing. It is completely voluntary to participate in this study but we will first need to receive a signed written consent form from you before the study can proceed. If you are interested in this study, please mention this to your doctor or orthopaedic surgeon so that they can provide you with a full information sheet. Many Thanks, Mr Richmond Arcillas University of Manchester School of Pharmacy Email: richmond.arcillas@student.manchester.ac.uk Tel: 0161 257 6861
- 41. The impact of smoking and calorie intake on bone fracture healing 35 7.2 Appendix 2 – Full information sheet for participants
- 42. The impact of smoking and calorie intake on bone fracture healing 36 The impact of smoking and calorie intake on bone fracture healing We appreciate you for taking interest in our research. Please take your time to read this sheet for full the information regarding our study. 1. Introduction You have been given this full information leaflet because you are eligible and have shown interest towards partaking in this study. It is important for us that you read this information leaflet thoroughly so that you understand the purpose of this study, what information we need from you, and what we will do with that information for the purpose of our research. Before you can participate, we will need you to sign and submit a written information consent form. Please do not hesitate to contact us using the details provided at the bottom of this leaflet if you wish to ask any other questions regarding the study before agreeing to take part. If you change your mind and decide not to participate in this study, the standard of treatment and care you will receive will not be affected. 2. Purpose of the study The purpose of this study is to assess how smoking and the amount of calories you consume will affect the time it takes for your fracture to heal. You have been chosen because we want to look at these effects particularly in the population with osteoporosis. From this, we hope to find ways in which we can improve the rate of fracture healing so that we can minimise the
- 43. The impact of smoking and calorie intake on bone fracture healing 37 length of hospital stay and help to return patients with fractures to the level of independence before the fracture, as soon as possible. 3. The research team I will be leading the research team on behalf of the University of Manchester, and will be working alongside participating orthopaedic surgeons and radiologists in Manchester Royal Infirmary, where the study will be conducted. You will be able to contact any member of the research team if you want to ask any further questions regarding the study. 4. Your role in the research study You will be required to complete a questionnaire at the start of the study regarding your smoking status. You will also have follow-ups with the radiologist in the Manchester Royal Infirmary so that we can X-ray your fracture in order to keep track of the progress of healing. The follow-ups will be at two weeks after your discharge from the hospital and every three months after discharge until your fracture has healed, for a maximum of 24 months (2 years). If your fracture has healed before 24 months then your participation in this study has completed and you will no longer be required to go to your follow-ups. Furthermore, you will be provided an electronic diary at the start of the study. In this study, we would like you to record the amount of cigarettes you smoke each day (if applicable). If you do not smoke or have stopped smoking over 6 months ago, then please keep track of the foods you consume each day, and whenever possible, the amount of calories you are consuming for each meal or snack.
- 44. The impact of smoking and calorie intake on bone fracture healing 38 At each follow-up period, you will be required to complete a questionnaire regarding your smoking status, calorie intake, and quality of life. This may take approximately 20 minutes. Please ensure that the information you provide is as accurate as possible so that results gained from this study is viable and is not misinterpreted. For each follow-up period, you will be reimbursed with £35 for your time and effort. All your travel expenses to and from Manchester Royal Infirmary will also be paid for, as well as any catering expenses in the hospital. 5. Confidentiality and data protection The data we receive from you will be used for comparison between other participants, so that we can assess the impact of smoking and calorie intake on the rate of bone fracture healing. The results will be written up in a report that will be peer-reviewed and possible be published in scientific journals. All questionnaires and your patient medical records will be kept confidential throughout and after the study. Only the participating orthopaedic surgeons and radiologists will have access to your medical records and will only provide me with the necessary information required for the purpose of the study. The information we require are: age, sex, BMI, other medical conditions, smoking status, fracture classification, and the method for treating the fracture. This is in order for us to group the participants accordingly so that we can limit the variation in the results due to these factors. Your information details, including your name and address will be anonymised for the purpose of data analysis. This means that your
- 45. The impact of smoking and calorie intake on bone fracture healing 39 information is used only for the purpose of the research and will not be able to be traced back to you. All electronic records will be stored in a secure password-encrypted system and any unused information will be destroyed at the end of the study. 6. Your rights Participation in this study is completely voluntary therefore you have the right to withdraw at any point throughout this study. If you choose to, then you will no longer receive further reimbursement and your data may not be used. However, you may keep any reimbursement prior to withdrawing from the study. You also have the right to request for the summary of our findings if you wish to see how we are interpreting your results. 7. Risk and benefits There are no significant risks apart from what you are normally exposed to on a day-to-day basis, if you partake in this study. This study is merely observational and we will only require you to report your calorie intake and smoking status during the follow-up periods. The X-ray scans the radiologist will be performing on you is safe and will not be detrimental to your health. We cannot guarantee that you will benefit from this study, however, you will be partaking in one of the largest studies of this kind and you will be contributing to future scientific research that may benefit patients with conditions similar to yours in the future.
- 46. The impact of smoking and calorie intake on bone fracture healing 40 8. Next step If you have read the information above and have decided to volunteer to take part in this study then please complete and sign the written consent form enclosed in this envelope. Please return it to your doctor or your orthopaedic surgeon so that we can provide you with a diary. Thank you very much for your time and consideration If you have any further questions regarding this study, then please contact: Mr Richmond Arcillas University of Manchester School of Pharmacy Email: richmond.arcillas@student.manchester.ac.uk Tel: 0161 257 6861
- 47. The impact of smoking and calorie intake on bone fracture healing 41 7.3 Appendix 3 – Consent form
- 48. The impact of smoking and calorie intake on bone fracture healing 42 Participant Consent Form Please complete this form and return to your orthopaedic surgeon. 1. I have read the information sheet thoroughly and I have asked any necessary questions regarding the study so that I have full understanding of what is required in participating in the study. 2. I understand the purpose of this study, how my data will be used, and my rights. 3. I understand that I will be required to attend the Manchester Royal Infirmary for follow-ups two weeks after my discharge, and every three months after discharge thereafter for a total of 24 months or until my fracture has healed. 4. I understand that participation in this study is completely voluntary and that I can withdraw from the study at any point throughout the study period. If I withdraw, I will no longer receive further reimbursements and my data may not be used. 5. I understand that my personal data will be used solely for the purpose of the research study and that any information will be kept confidential and anonymised, in accordance with the Data Protection Act 1998. 6. I promise that the information I provide throughout this study will be accurate and to the best of my knowledge. Name: Date: Signature: Contact details:
- 49. The impact of smoking and calorie intake on bone fracture healing 43 7.4 Appendix 4 – Self-completion questionnaire
- 50. The impact of smoking and calorie intake on bone fracture healing 44 Self-completion questionnaire N.B. this questionnaire is an example only. The questionnaire will be done online via an electronic tablet. BASELINE MEASUREMENT ID number Date of Birth Sex M F I prefer not to answer Which of the following best describes your Race? White/Caucasian Asian Indian Japanese Black, African American Chinese Korean American Indian or Alaska native Filipino Vietnamese Other race (please specify) Other Asian (please specify) I prefer not to answer 1. Smoking status a. Have you ever smoked a cigarette, even for just a few puffs? Yes [] No [] b. How often do you smoke? Please tick one box only I have never smoked []
- 51. The impact of smoking and calorie intake on bone fracture healing 45 I am not a current smoker [] I have quit smoking [] At least once a day [] At least once a week [] At least once a month [] Less than once a month [] c. If you ticked ‘I have quit smoking’ (b), how long has it been since you quit? Please tick one box only (otherwise leave this section blank) About a week ago [] Less than a month ago [] Less 3 months ago [] Less than 6 months ago [] Over 6 months ago [] Over a year ago [] Over 2 years ago [] d. If you have recently quit, are you on nicotine replacement therapy? Yes [] No[] e. If the answer to (d) was ‘yes’, please specify what nicotine replacement therapy you are on (otherwise leave this section blank) ………………………………………………………………………..… …………………………………………………………………………..