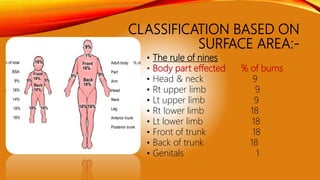
1) Burns are injuries caused by heat or chemicals and can be classified based on depth and surface area affected.
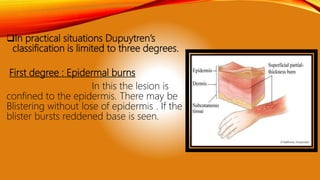
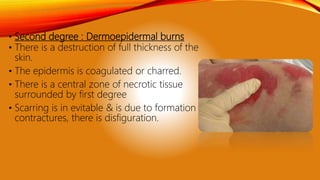
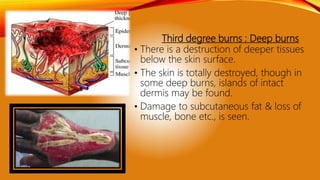
2) First degree burns involve only the epidermis, second degree extend deeper to the dermis, and third degree destroy the entire skin.
3) Complications can include shock, infection, organ failure and death in severe cases.
4) Treatment depends on severity but generally involves cooling the burn, pain relief, wound care, fluid resuscitation and antibiotics to prevent infection.