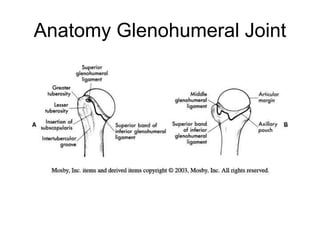
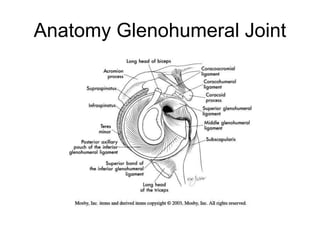
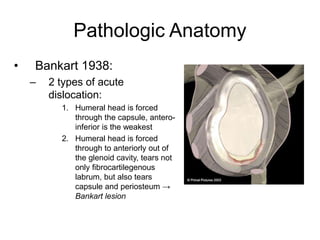
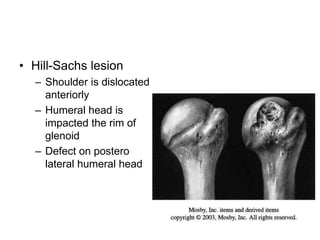
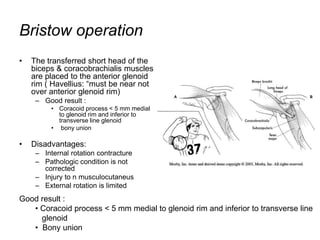
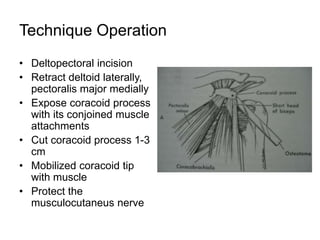
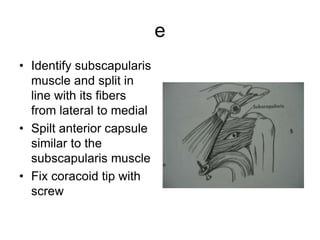
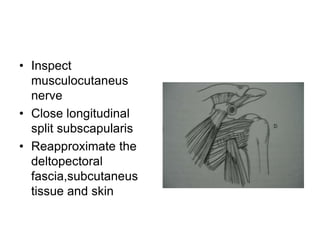
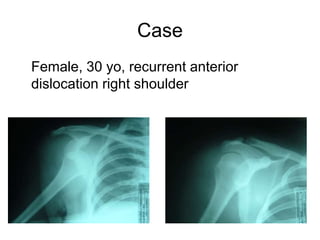
This document outlines the Bristow procedure for treating recurrent anterior shoulder dislocations. It begins with an introduction describing the shoulder's anatomy and instability issues. It then discusses the Bankart lesion pathology and surgical treatment goals. The Bristow operation is described as transferring the short head of the biceps and coracobrachialis muscles to the anterior glenoid rim to add stability. The technique involves exposing the coracoid process and fixing it to the glenoid rim. Post-operative care includes immobilization, progressive range of motion exercises, and return to sports after 3-6 months. The case example is of a 30-year-old female with recurrent right shoulder dislocations to be treated with this procedure.