Download to read offline

![DEFINITION
DEFINITION:- Breast cancer is a malignancy originating from breast tissue. This chapter
distinguishes between early stages, which are potentially curable, and metastatic breast cancer
(MBC), which is usually incurable.
EPIDEMIOLOGY:-
The strongest risk factors for breast cancer are female gender and increasing age. Additional
risk factors include endocrine factors (e.g., early menarche, nulliparity, late age at first birth,
hormone replacement therapy), genetic factors (e.g., personal and family history, mutations of
tumor suppresser genes [BRCA1 and BRCA2]), and environmental and lifestyle factors (e.g.,
radiation exposure).
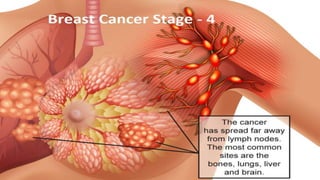
Breast cancer cells often spread undetected by contiguity, lymph channels, and through the
blood early in the course of the disease, resulting in metastatic disease after local therapy. The
most common metastatic sites are lymph nodes, skin, bone, liver, lungs, and brain.](https://image.slidesharecdn.com/breatcancer-200405203245/85/Breat-cancer-2-320.jpg)






Breast cancer is a malignancy originating from breast tissue, with risk factors including female gender, age, and genetic predispositions. The document discusses the clinical presentation, diagnosis, staging, and various treatment options for early, locally advanced, and metastatic breast cancer, emphasizing the goals of treatment and prognostic factors. It also highlights the evolving nature of breast cancer therapy, including the use of systemic, adjuvant, and targeted therapies.









































































