Download to read offline













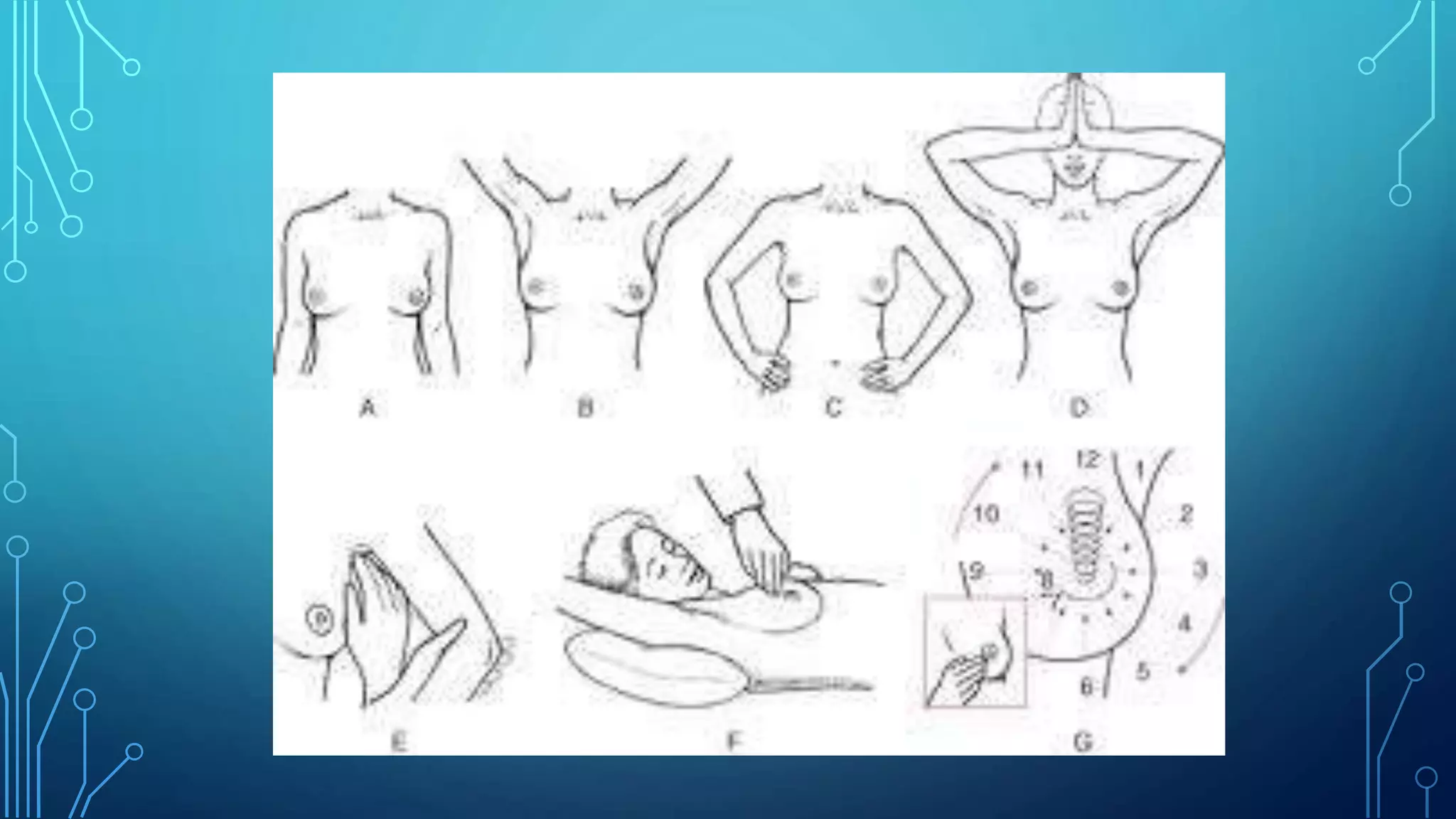
![PATIENT EXAMINED IN VARIOUS POSITIONS
• Semi-recumbent lying position (low)- Best position to find the tumor
• Sitting postion
• Hand lifting up position to look for Peau de orange, nipple retraction
• compressing the hands at hip - Alternately contracting and relaxing
the Pectoralis muscle to look for pectoralis major muscle involvement
(fixity) – [Swelling becomes prominent or not ]
• Leaning forward position helps to identify Chest wall involvement
(ribs, IC muscle, serratus anterior).(Breast falls equally on both sides if
not fixed)](https://image.slidesharecdn.com/breastexams-230917180021-06f83966/75/Breast-exams-pptx-14-2048.jpg)








































































Dr. Thana Ram Patel discusses breast exams. Screening tools for breast cancer include clinical breast exams, breast self exams, mammography, ultrasonography, FNAC, and cytology of nipple discharge. Breast cancer is the most common cancer in women worldwide and the most common cause of death from cancer among women. Early detection through screening can effectively treat most breast cancers. The document provides detailed instructions on performing clinical breast exams, including inspection of the breasts and palpation techniques.









































![Breast-Examination in pregnant woment[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/breast-examination1-251003133207-974f204a-thumbnail.jpg?width=640&height=640&fit=bounds)









































