Download to read offline

![• Blue nevus (BN) and related entities are a
heterogeneous group of congenital and
acquired melanocytic tumors that
encompasses dendritic (“common”) blue
nevus (DBN), cellular blue nevus (CBN), and
variants, as atypical cellular blue nevus (ACBN)
and malignant BN/melanoma (Murali et al.,
2009) [1].](https://image.slidesharecdn.com/bluenevus-180403145321/85/Blue-nevus-3-320.jpg)
![• The scalp and the extremities are less commonly
affected. Unusual clinical features of blue nevi
include congenital, familial, eruptive, plaque-like,
targetoid, and linear forms (Causeret et al., 1977)
[12]. The term “agminated BN” has been availed
for multiple blue nevi sometimes arising within
amongolian spot. Generally, all lesions are
belonging to the BN family and it represents
demographic and clinical characteristics which
are similar to those of common and cellular blue
nevi. “](https://image.slidesharecdn.com/bluenevus-180403145321/85/Blue-nevus-7-320.jpg)
![• Hypochromic” variants of blue nevi do not
seem to be “ancient” blue nevi because of the
young age of most of the patients. These
variants of BN are very rarely recognized as
such on clinical grounds: in fact, the paucity of
melanin often imparts a grayish or even a
grayish- brown color (Butler et al.,1967) [13].
Epithelioid BN also is similar to BN from a
clinical point of view, but is histopathologically
distinctive.](https://image.slidesharecdn.com/bluenevus-180403145321/85/Blue-nevus-8-320.jpg)



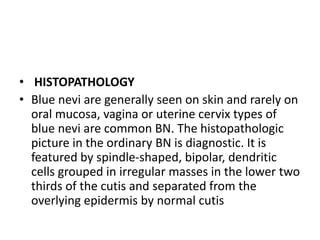
Blue nevi are melanocytic tumors appearing as blue, gray, brown, or black nodules, often confused with pigmented nevi or melanoma. They include variations such as common blue nevus and cellular blue nevus, each with specific characteristics and histopathological features. Typically found on the skin, their presentation and diagnosis can be varied, with some exceptional forms noted in different locations.