INTRODUCTION
• Micturition isa process by which urine is voided from the urinary bladder.
• It is a reflex process. However, in grown up children and adults, it can be controlled voluntarily to someextent.
• Functional anatomy and nerve supply of urinary bladder are essential for the process of micturition. (Ref. K Sembulingam)
• Micturition is the processby which the urinary bladder empties when it becomes filled.
• This involves two main steps:
• First, the bladder fills progressively until the tension in its walls rises above a threshold level.
• The second step, which is a nervous reflex called the micturition reflex that empties the bladder or, if this fails, at least causes a conscious
desire to urinate.
• Althoughthe micturition reflex is an autonomic spinal cord reflex. (Ref. Guyton and Hall)
• Micturition is a process by which urine is voided from the urinary bladder.
• It is a reflex process. (Ref. Modern Physiology)
( Dr. Gyanendra Kumar Gupta)
4.
• 1. Kidneys:Filter blood and produce urine.
• 2. Ureters: Two narrow tubes that carry urine from each kidney to the urinary bladder.
• 3. Urinary bladder: A muscular sac that temporarily stores urine (capacity about 300-400 mL).
• 4. Urethra: The tube that carries urine from the bladder to the outside.
Organs Involved
(Ref. K Sembulingam)
5.
(Ref. Guyton andHall)
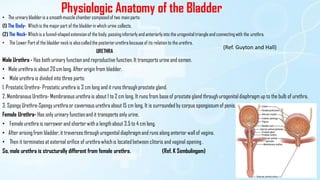
Physiologic Anatomy of the Bladder
• The urinary bladderis a smoothmusclechambercomposedof two main parts:
(1) The Body- Whichis the majorpart of the bladderin which urine collects.
(2) The Neck- Whichis a funnel-shapedextensionof the body, passinginferiorly and anteriorlyinto the urogenitaltriangleand connectingwith the urethra.
• The Lower Part of the bladderneckis alsocalledthe posteriorurethrabecauseof its relation to the urethra.
URETHRA
Male Urethra - Has both urinary function and reproductive function. It transports urine and semen.
• Male urethra is about 20 cm long. After origin from bladder.
• Male urethra is divided into three parts:
1. Prostatic Urethra- Prostatic urethra is 3 cm long and it runs through prostate gland.
2. Membranous Urethra- Membranous urethra is about 1 to 2 cm long. It runs from base of prostate gland through urogenital diaphragm up to the bulb of urethra.
3. Spongy Urethra-Spongy urethra or cavernous urethra about 15 cm long. It is surrounded by corpus spongiosum of penis.
Female Urethra- Has only urinary function and it transports only urine.
• Female urethra is narrower and shorterwith a length about 3.5 to 4 cm long.
• After arising from bladder, it traverses through urogenital diaphragmand runs along anterior wall of vagina.
• Then it terminates at external orifice of urethra whichis located between clitoris and vaginal opening .
So, male urethra is structurally different from female urethra. (Ref. K Sembulingam)
6.
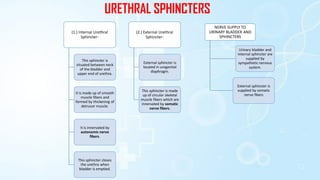
URETHRAL SPHINCTERS
(1.) InternalUrethral
Sphincter-
This sphincter is
situated between neck
of the bladder and
upper end of urethra.
It is made up of smooth
muscle fibers and
formed by thickening of
detrusor muscle.
It is innervated by
autonomic nerve
fibers.
This sphincter closes
the urethra when
bladder is emptied.
(2.) External Urethral
Sphincter-
External sphincter is
located in urogenital
diaphragm.
This sphincter is made
up of circular skeletal
muscle fibers which are
innervated by somatic
nerve fibers.
NERVE SUPPLY TO
URINARY BLADDER AND
SPHINCTERS
Urinary bladder and
internal sphincter are
supplied by
sympathetic nervous
system.
External sphincter is
supplied by somatic
nerve fibers
7.
2.
PARASYMPATHETIC
NERVE SUPPLY
Arise fromsecond,
third and fourth
sacral segments
(S2, S3 and S4) of
spinal cord. These fibers run through
hypogastric ganglion and
synapse with
postganglionic neurons
situated in close relation
to urinary bladder and
internal sphincter
It cause contraction of
detrusor muscle and
relaxation of internal
sphincter leading to
emptying of urinary
bladder. So
parasympathetic nerve
is called the nerve of
emptying or nerve of
micturition.
1.
SYMPATHETIC
NERVE
SUPPLY
Arise from first two
lumbarsegments (L1
and L2) of spinal
cord.
After leaving spinal
cord, the fibers pass
through lateral
sympathetic chain
without any synapse in
the sympathetic
ganglia and finally
terminate in
hypogastric ganglion.
Postganglionic fibers
arising from
hypogastric ganglion
form hypogastric nerve
which supplies the
detrusor muscle and
internal sphincter.
Sympathetic
(hypogastric)nerve
causes relaxation of
detrusor muscle and
constrictionof the
internal sphincter. It
results in filling of
urinary bladder and
so the sympathetic
nerve is called nerve
of filling.
3.
SOMATIC
NERVE
SUPPLY
External
sphincter is
innervated by
somatic nerve
called pudendal
nerve.
It arises from
second, third and
fourth sacral
segments of the
spinal cord.
Pudendal nerve
maintains the tonic
contraction of the
skeletal muscle fibers
of the external
sphincter and keeps
the external sphincter
constricted always.
It causes relaxation of
external sphincter
leading to voiding of
urine. Thus, the
pudendal nerve is
responsible for
voluntary control of
micturition.
8.
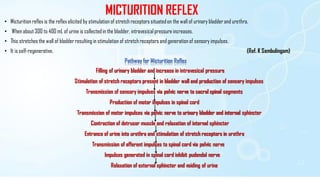
MICTURITION REFLEX
• Micturitionreflex is the reflex elicited by stimulation of stretch receptors situatedon the wall of urinary bladderand urethra.
• When about 300 to 400 mL of urine is collected in the bladder, intravesical pressure increases.
• This stretches the wall of bladderresulting in stimulation of stretch receptors and generation of sensory impulses.
• It is self-regenerative. (Ref. K Sembulingam)
Pathway for Micturition Reflex
Filling of urinary bladder and increase in intravesical pressure
Stimulation of stretch receptors present in bladder wall and production of sensory impulses
Transmission of sensory impulses via pelvic nerve to sacral spinal segments
Production of motor impulses in spinal cord
Transmission of motor impulses via pelvic nerve to urinary bladder and internal sphincter
Contraction of detrusor muscle and relaxation of internal sphincter
Entrance of urine into urethra and stimulation of stretch receptors in urethra
Transmission of afferent impulses to spinal cord via pelvic nerve
Impulses generated in spinal cord inhibit pudendal nerve
Relaxation of external sphincter and voiding of urine
9.
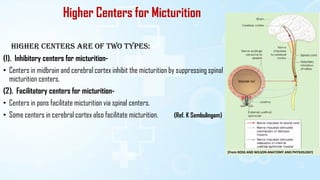
Higher Centers forMicturition
Higher centers are of two types:
(1). Inhibitory centers for micturition-
• Centers in midbrain and cerebral cortex inhibit the micturition by suppressing spinal
micturition centers.
(2). Facilitatory centers for micturition-
• Centers in pons facilitate micturition via spinal centers.
• Some centers in cerebral cortex also facilitate micturition. (Ref. K Sembulingam)
(From ROSS AND WILSON ANATOMY AND PHYSIOLOGY)
10.
(1.) ATONIC BLADDER:EFFECT OF DESTRUCTION OF SENSORYNERVE FIBERS-
• Atonic bladder flaccid neurogenic bladder, or hypoactive neurogenic bladder is the urinary bladder with loss of tone in detrusor muscle.
• It is caused by destruction of sensory (pelvic) nerve fibers of urinary bladder.
Causes for Atonic Bladder – (i) Spinal injury (ii) Syphilis
(2.) AUTOMATIC BLADDER-
• Automatic bladder is characterized by hyperactive micturition reflex with loss of voluntary control.
• So, even a small amount of urine collected in the bladder elicits the micturition reflex resulting in emptying of bladder.
• The voluntary control is lacking because of absence of inhibition or facilitation of micturition by higher centers.
(3.) UNINHIBITED NEUROGENIC BLADDER-
• This condition is characterizedby frequent and uncontrollable micturition.
• It is due to lesion in midbrain which causes continuous excitation of spinal micturition centers resulting in frequent and uncontrollable micturition.
(4.) NOCTURNAL MICTURITION-
1. Nocturnal micturition or nocturnal enuresis or bedwetting is the involuntary voiding of urine during night.
• It occurs due to the absence of voluntary control of micturition.
• It is a common and normal process in infants and children below 3 years because of incomplete myelination of motor nerve fibers of the bladder.
2. When myelination is complete, voluntary control of micturition develops and bedwetting stops. (Ref. K Sembulingam)
11.
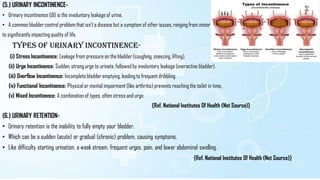
(5.) URINARY INCONTINENCE-
•Urinary incontinence (UI) is the involuntary leakage of urine.
• A common bladdercontrol problem that isn't a disease but a symptom of other issues, ranging from minor
to significantly impactingquality of life.
Types of Urinary Incontinence-
(i) Stress Incontinence: Leakage from pressure on the bladder(coughing, sneezing, lifting).
(ii) Urge Incontinence: Sudden, strong urge to urinate, followed by involuntary leakage (overactive bladder).
(iii) Overflow Incontinence: Incomplete bladder emptying, leading to frequent dribbling.
(iv) Functional Incontinence: Physical or mental impairment (like arthritis) prevents reachingthe toilet in time.
(v) Mixed Incontinence: A combination of types, often stress and urge.
{Ref. National Institutes Of Health (Net Source)}
(6.) URINARY RETENTION-
• Urinary retention is the inability to fully empty your bladder.
• Which can be a sudden (acute) or gradual (chronic) problem, causing symptoms.
• Like difficulty starting urination, a weak stream, frequent urges, pain, and lower abdominal swelling.
{Ref. National Institutes Of Health (Net Source)}
12.
REFERENCES
1. K SEMBULINGAM
2.GUYTON AND HALL
3. MEDICAL PHYSIOLOGY (DR. GYANENDRA KUMAR GUPTA)
4. NET SOURCE
5. ROSS AND WILSON ANATOMY AND PHYSIOLOGY