INTRODUCTION
What is Autonomy?
The freedom and ability to act in a self-determined
manner
An integral part of patient autonomy is the ability
to make decisions over bodily integrity
Depends on the patient being given the
information in a manner that they understand
3.
AUTONOMY
Informed consent
Effective medicaltreatment - a mutual (bilateral)
communication between a doctor and a patient
Increases patient's legal and health awareness
Represents a patient's consent to a medical
treatment on the basis of previous instruction
Required in addition for the health care to be
provided
4.
AUTONOMY
Elements and requirementsof the Informed
Consent
A valid consent is composed out of 3 segments,
that need to be present all at a time
Given by a competent person
A person has to be overly informed about the
whole procedure or process to which he is giving
his consent
Needs to be given voluntarily, not under any kind
of pressure
5.
AUTONOMY
EXCEPTIONS CONCERNING INFORMED
CONSENT
Incase of their appearance in a particular
situation override the right to self-determination,
and a doctor's act is allowed even without
obtaining consent to a treatment
1) Emergency Exception
2) Incompetence
3) A Right to Not Know and Therapeutic Privilege of
Doctor
4) Compulsory Treatment
6.
AUTONOMY
The Convention onHuman Rights and
Biomedicine
“An intervention in the health field may only be
carried out after the person concerned has given
free and informed consent to it. This person shall
beforehand be given appropriate information as
to the purpose and nature of the intervention as
well as on its consequences and risks. The person
concerned may freely withdraw consent at any
time." (Article 5)
7.
THE PRINCIPLE OFAUTONOMY
One of the basic principles accepted worldwide
Contains :
1. a protection of autonomous decisions
2. a protection of bodily integrity
Consists of more partial rights:
1. the right of patient to know all the information
about a treatment
2. the right to make decisions about treatment
8.
THE PRINCIPLE OFAUTONOMY
The right to not be treated without one's consent
to it
The right to either consent or refuse the proposed
treatment
If a consent to a treatment is given, a particular
treatment (intervention) can be done. However,
there is a possibility to withdraw such consent at
any time
9.
THE PRINCIPLE OFAUTONOMY
The treating Physician must do everything
possible to ensure that patients (or their
representatives in case of incompetence)
understand all issues related to their clinical
status
Inform them of the possible courses of
therapeutic action available to them and make
sure that they are acting of their own volition and
not under any external duress
If so, patients are considered to be autonomous,
and by extension competent to make decisions
related to their bodies or health, and it is the
practitioners’ duty to accept and respect their
10.
THE FIVE DIMENSIONSOF
PATIENT AUTONOMY
Decisional Autonomy
Functional Autonomy
Executive Autonomy
Narrative Autonomy
Informative Autonomy
11.
THE FIVE DIMENSIONSOF
PATIENT AUTONOMY
Decisional Autonomy
Refers to patients’ freedom of choice, in other
words, their capacity to deliberate and decide on a
course of action from among a suitable range of
useful options
Exercised between the medical practitioner and
the patient
12.
THE FIVE DIMENSIONSOF
PATIENT AUTONOMY
Functional Autonomy
Patients’ capacity to perform the basic activities
of daily living and to individually undertake tasks
that a statistical majority of people normally
perform (such as eating, seeing, walking,
understanding complex situations, etc.)
Depends upon the Mental, Physical and Sensory
functions
13.
THE FIVE DIMENSIONSOF
PATIENT AUTONOMY
Functional Autonomy
Contributed by the disabilities people have and
also from disabling environments
Relates to the material possibility of performing a
task (e.g., getting dressed without help)
14.
THE FIVE DIMENSIONSOF
PATIENT AUTONOMY
Executive Autonomy
May be defined as the capacity to implement the
decision made and maintain it over time, in other
words, to execute it
Involves the patient’s capacity to plan, sequence,
and perform tasks related to the management of
their chronic disease, especially those related to
the planning and execution of treatment
15.
THE FIVE DIMENSIONSOF
PATIENT AUTONOMY
Executive Autonomy
The patient’s executive autonomy is essential for
effective supervising and executing the treatment
plan
The essential aspect is the ability to keep to the
course of action decided upon (e.g., quitting
smoking)
Non-adherence, ignoring or underrating the
importance of executive autonomy leads to
“poorer health outcomes for patients, repeated
hospitalizations, and frustrated clinicians”
16.
THE FIVE DIMENSIONSOF
PATIENT AUTONOMY
Narrative Autonomy
The capacity that patients have to retain,
understand, and communicate for others, related
to circumstances of their illness, management
and treatment they received
Being capable of participating in certain types of
communicative interactions with others
Is the most basic features of the reality shared by
patient and audience
17.
THE FIVE DIMENSIONSOF
PATIENT AUTONOMY
Informative Autonomy
Involves patients’ ability to access and control
their personal, intimate, private, and public
information
Informative autonomy covers, the personal
management of clinical information, the right to
communicate or protect such information, the
doctor’s duty of confidentiality, and the skills
required to communicate with others about the
condition
18.
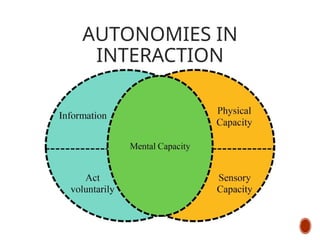
AUTONOMIES IN
INTERACTION
In thesetheories, the central aspect is individuals’
mental state, their transitory or permanent
capacity to take responsibility for their actions.
Some patients enjoy only limited functional
autonomy yet are decisional, executively, or
narratively autonomous
In other cases, poor executive autonomy may be
found with no other significant autonomous
deficit
THE CASES APPROACH
Developedby the National Centre for Ethics in
Health Care
Clarify the facts & requirements
Assemble the relevant information
Synthesize the information
Explain the synthesis
Support the ethical decision making process
21.
THE CASES APPROACH
Clarifythe facts & requirements
Characterize the type of problem
Obtain information about the case
Establish the goal from the ethical analysis
(consultation process)
Formulate the ethics question
22.
THE CASES APPROACH
Assemblethe relevant information
Consider the appropriate sources of information
Gather information systematically from each source
Summarise the information and the ethics question
23.
THE CASES APPROACH
Synthesizethe information
Determine weather a formal meeting is needed
Engage in ethical analysis
Identify the ethically appropriate decision maker
Facilitate moral deliberation about ethically
justifiable options
24.
THE CASES APPROACH
Explainthe synthesis
Communicate the synthesis to key participant
Provide additional resources
Document the consultation in the health record
Document the consultation in service records
25.
THE CASES APPROACH
Supportthe ethical decision making process
Follow up with the decision taken
Evaluate the outcome of the decision
Adjust the consultation process
Identify underlying systems issues
26.
THE FOUR BOXESMODEL
MEDICAL
INDICATION
S
PATIENT
PREFERENCE
S
QUALITY OF
LIFE
CONTEXTUA
L FEATURES
27.
THE FOUR BOXESMODEL
Medical Indications
Facts that indicate which form of diagnostic,
therapeutic or educational interventions are
appropriate
Is the problem Acute, chronic, critical, reversible
terminal ?
What are the goals of treatment ?
28.
THE FOUR BOXESMODEL
Medical Indications
In what circumstances are the medical treatment
not indicated ?
What are the probabilities of success of various
treatment options ?
How can the patient be benefited by medical care ?
How can any form of harm be avoided ?
29.
THE FOUR BOXESMODEL
Preferences of the patient
The choices that the patients make when they face
with the decisions about their health and medical
treatment
Consultant should include Ethical issues like :
Informed consent Refusal of treatment
Autonomy of the patient Advance directives
Alternative medicines Challenging patients
Cultural and religious beliefs
30.
THE FOUR BOXESMODEL
Quality of life
Refers to that degree of satisfaction that people
experience and value about their lives as a whole
and in its particular aspects, such as physical health
The main ethical principles involved are :
Beneficence and Autonomy
31.
THE FOUR BOXESMODEL
Quality of life
Relevant ethical questions :
What are the prospects with or without treatment
for return to normal life
What ethical issues may arise concerning
improving patients quality of life
32.
THE FOUR BOXESMODEL
Contextual features
It addresses the ways in which professional,
familial, religious, financial, legal and institutional
factors that may influence clinical decisions
Involved ethical principles includes - respect for
patient autonomy and justice
Justice refers to those moral and social theories that
attempt to distribute the benefits and burdens of a
social system in a fair and equitable way among all
participants in the system
33.
CONCLUSION
Autonomy entails considerablymore than just
decision-making by the patient and respecting that
autonomy involves much more than simply
presenting an informed consent form for signing
An important deficit in a person’s mental capacity
will result in a diminishment of both their
decisional and functional autonomy
People’s mental capacity is the link between
decisional and functional autonomy
In cases of serious mental damage, no other
dimension of autonomy is possible
34.
CONCLUSION
Patients with verysevere mental impairments are
not capable of :
Making decisions (decisional autonomy)
Performing for themselves many tasks that majority
of people can perform (functional autonomy)
Keeping to a given treatment over time (executive
autonomy)
Manifesting their communicative intentions in such
a way as to mold the response of their audience
(narrative autonomy)
Accessing and controlling their personal, intimate,
private, and public information







































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




