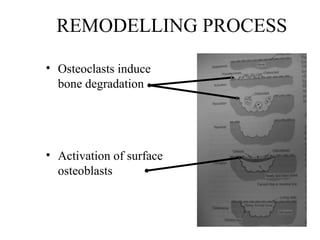
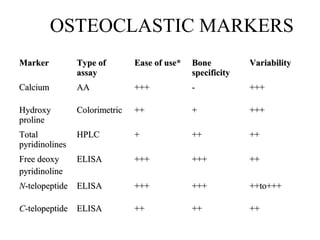
This document discusses biochemical markers that can be used to monitor bone formation and resorption. It notes that these markers may provide preferable alternatives to densitometry in some clinical settings. The document reviews the history of using biochemical markers in orthopedics and describes markers of bone formation mediated by osteoblasts and bone resorption mediated by osteoclasts. It also discusses factors like hormones, local stresses, and the environment that can impact bone turnover.