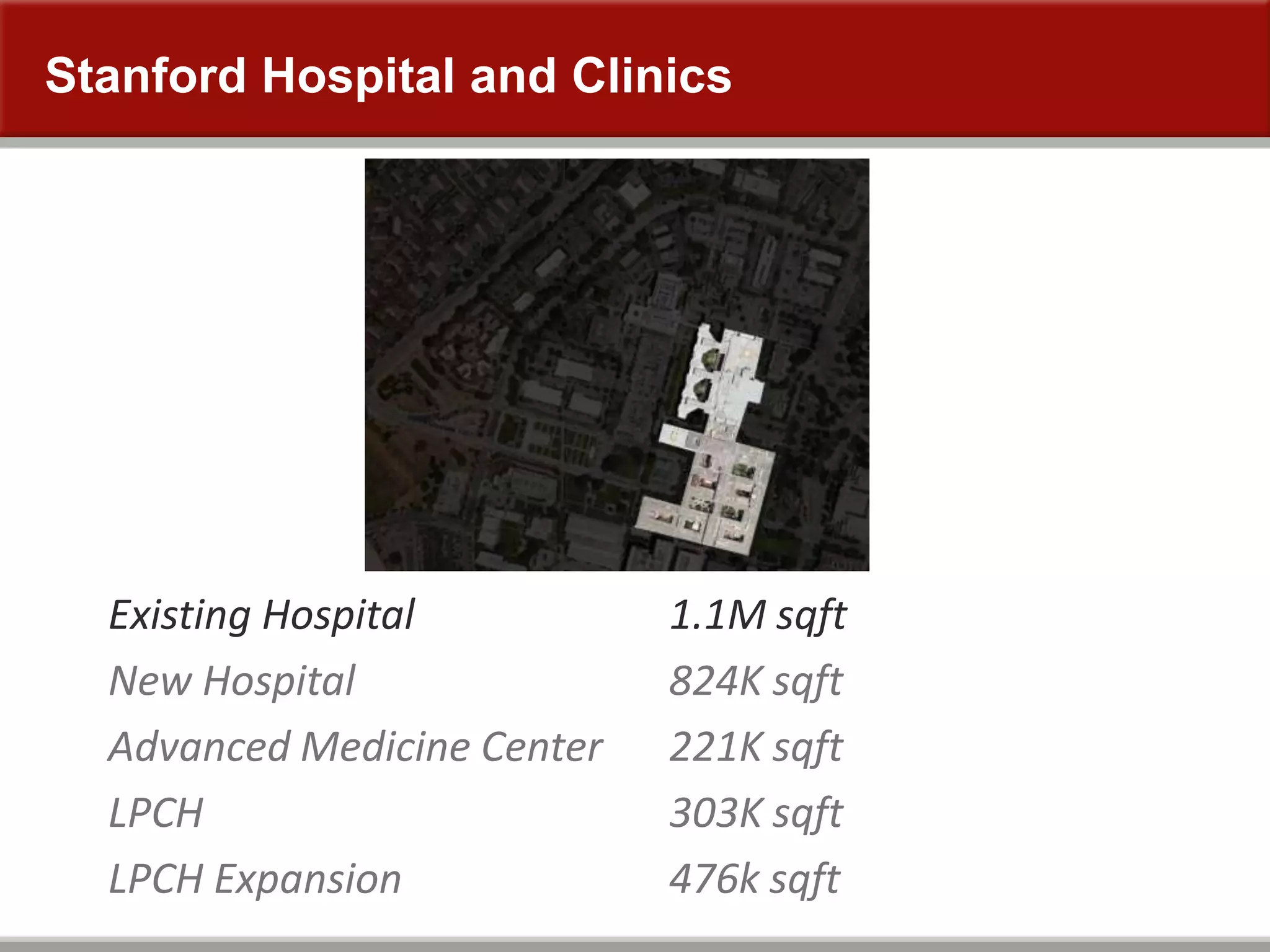
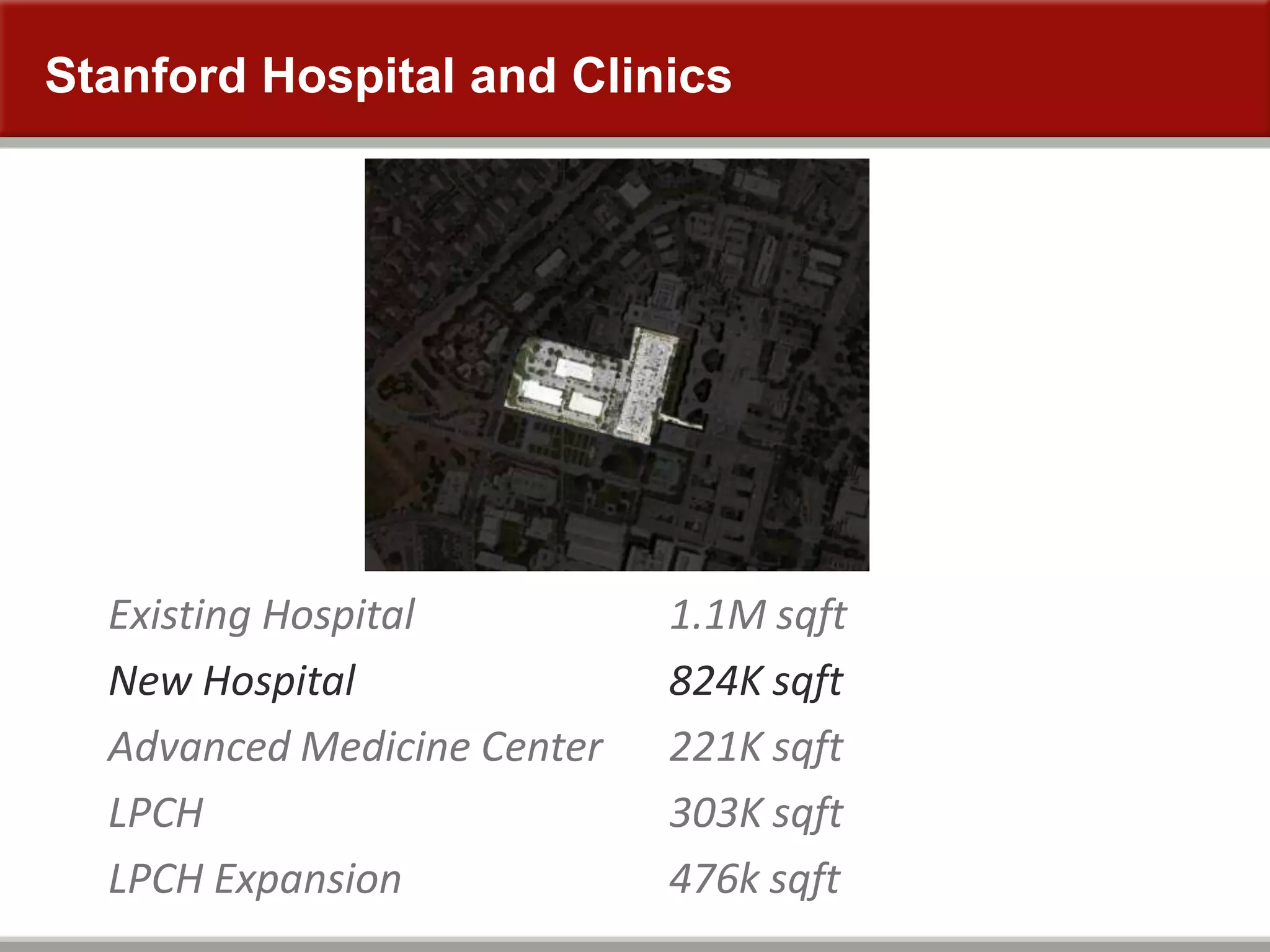
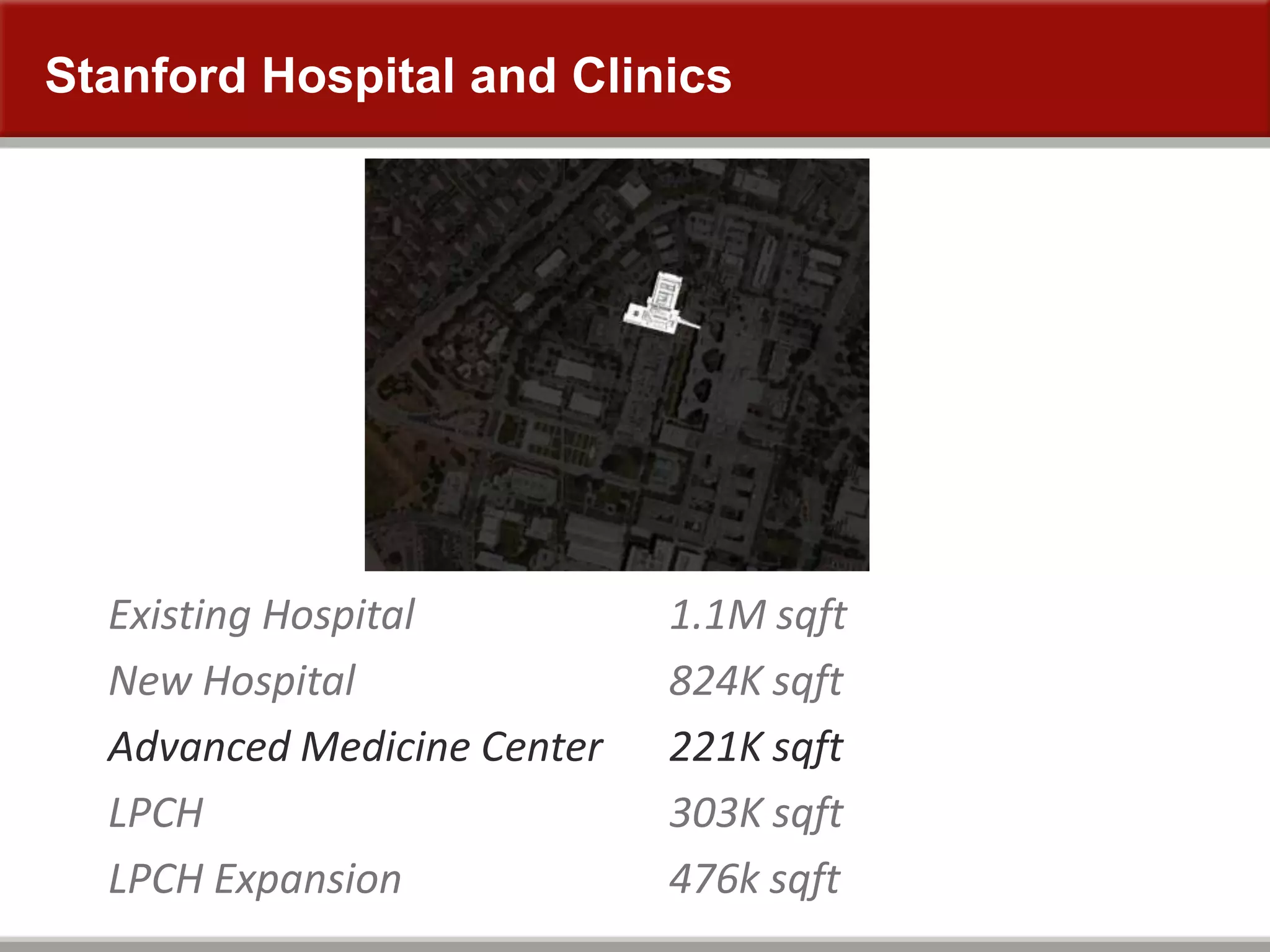
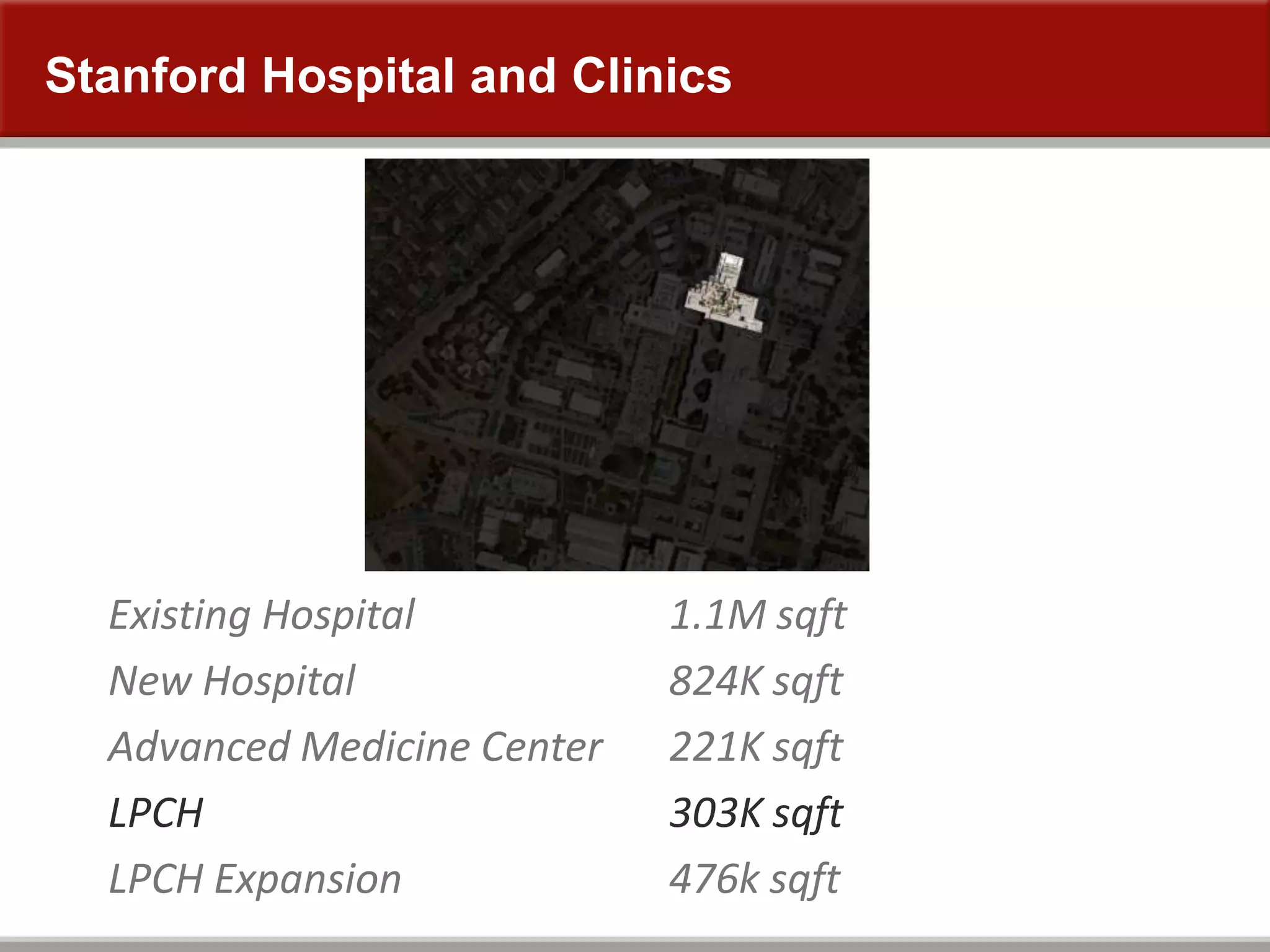
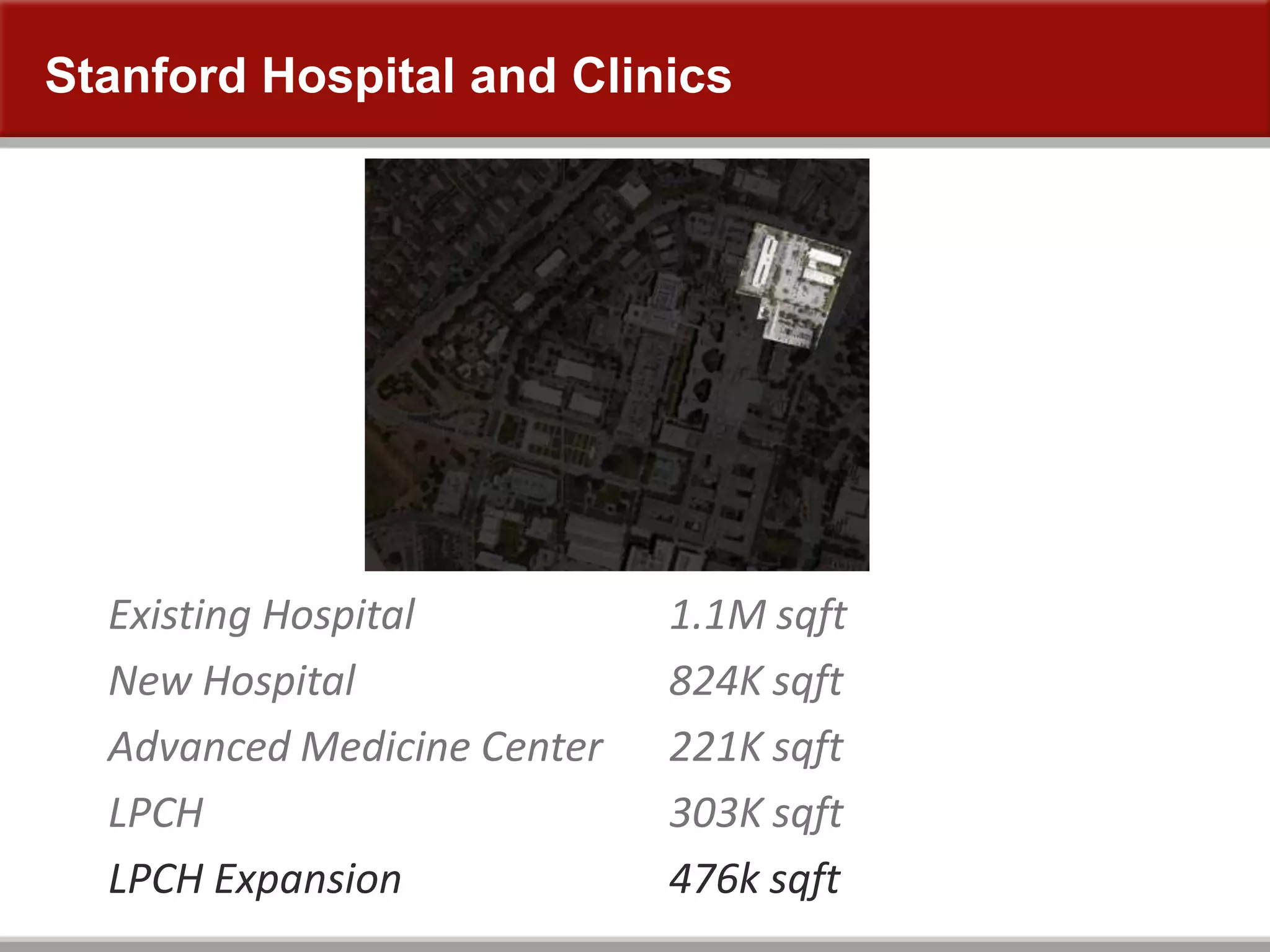
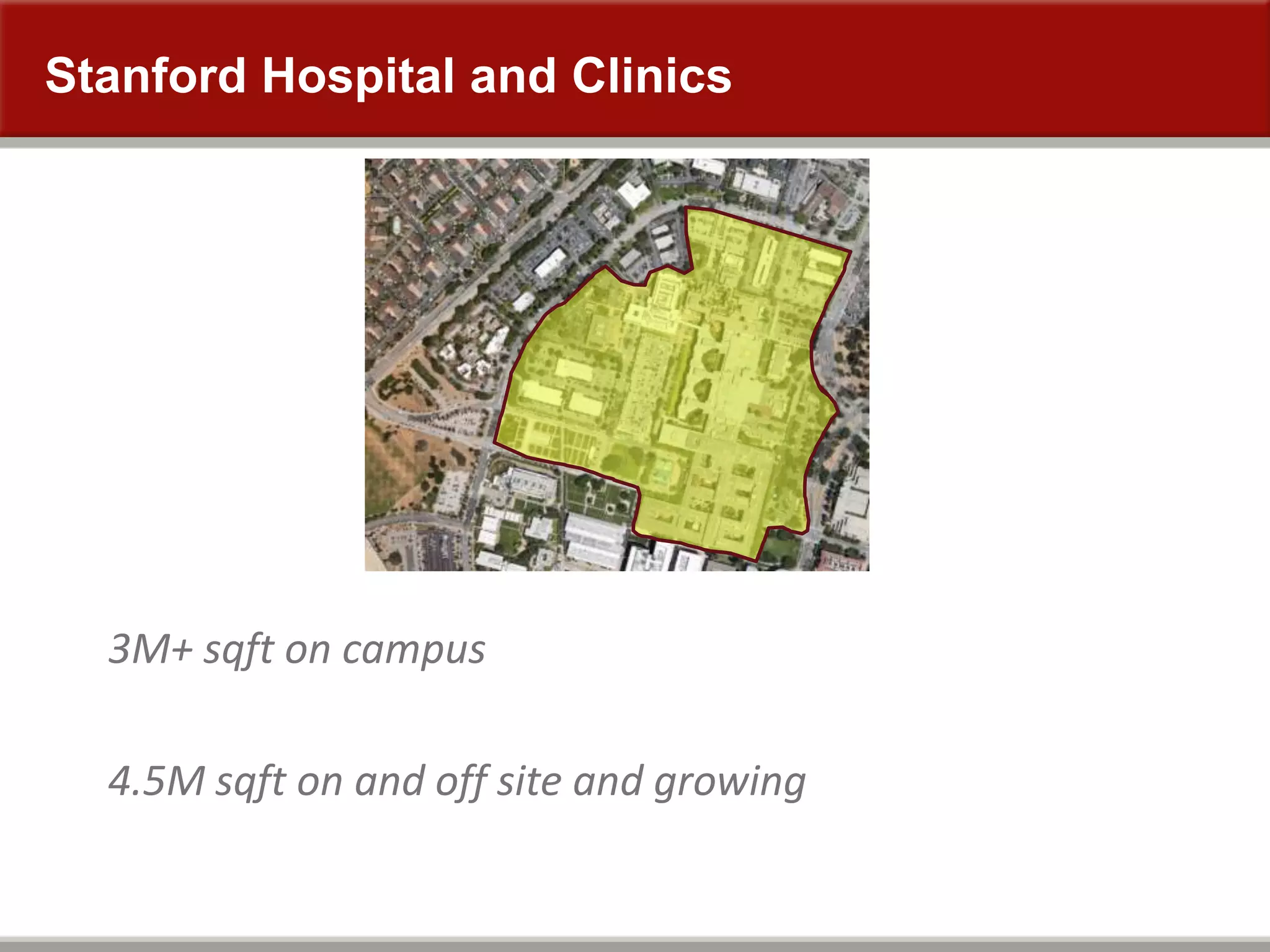
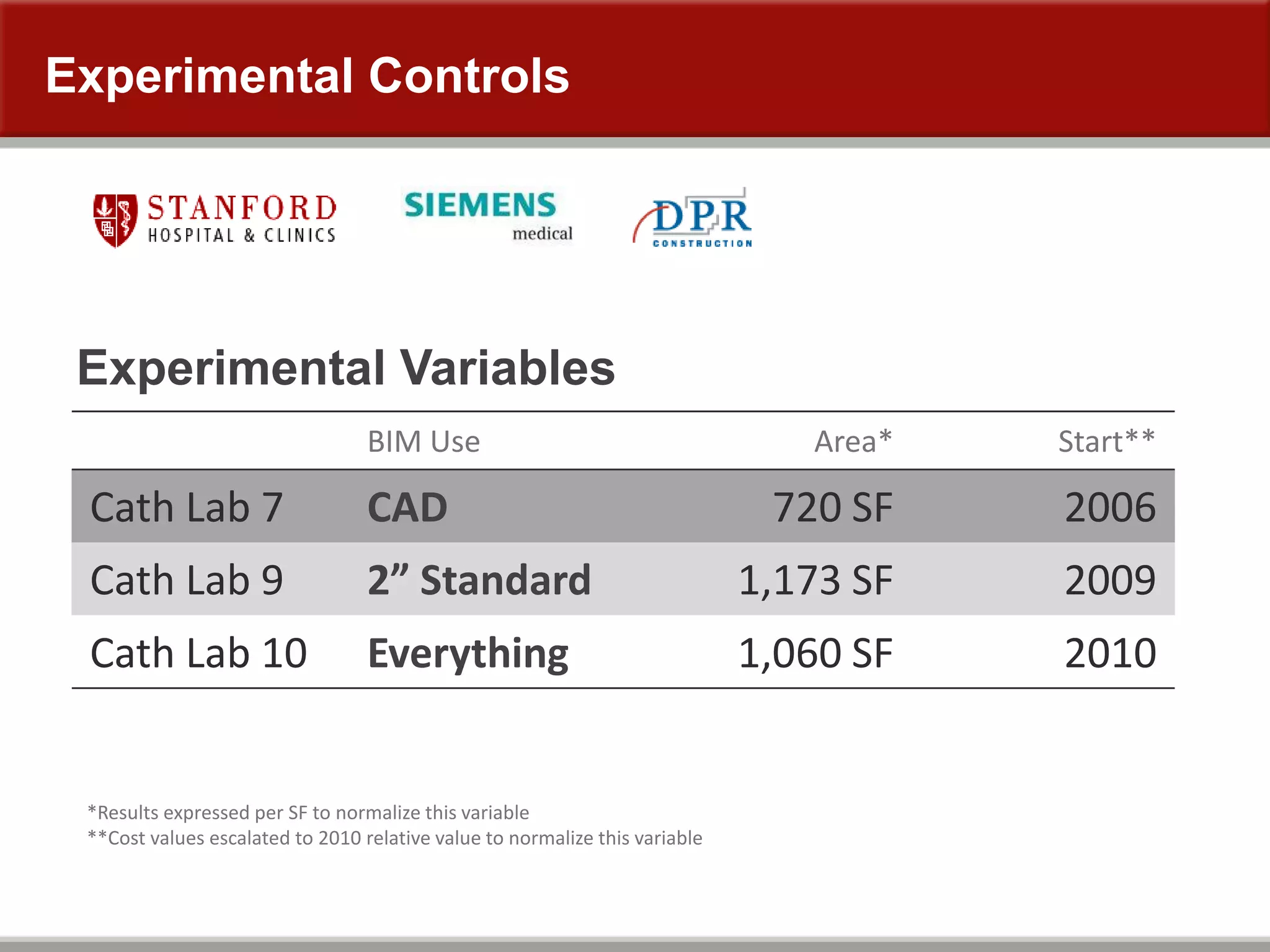
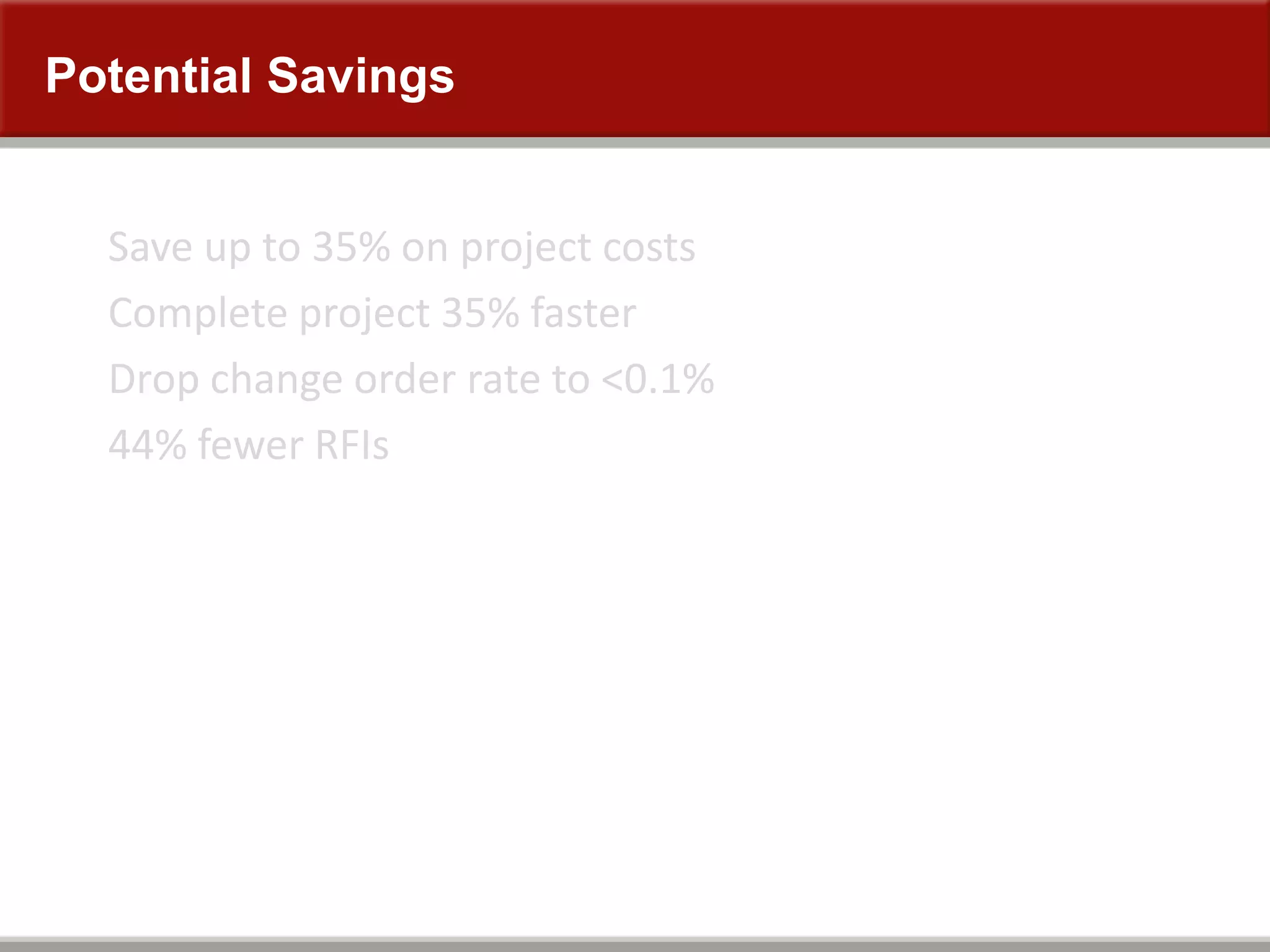
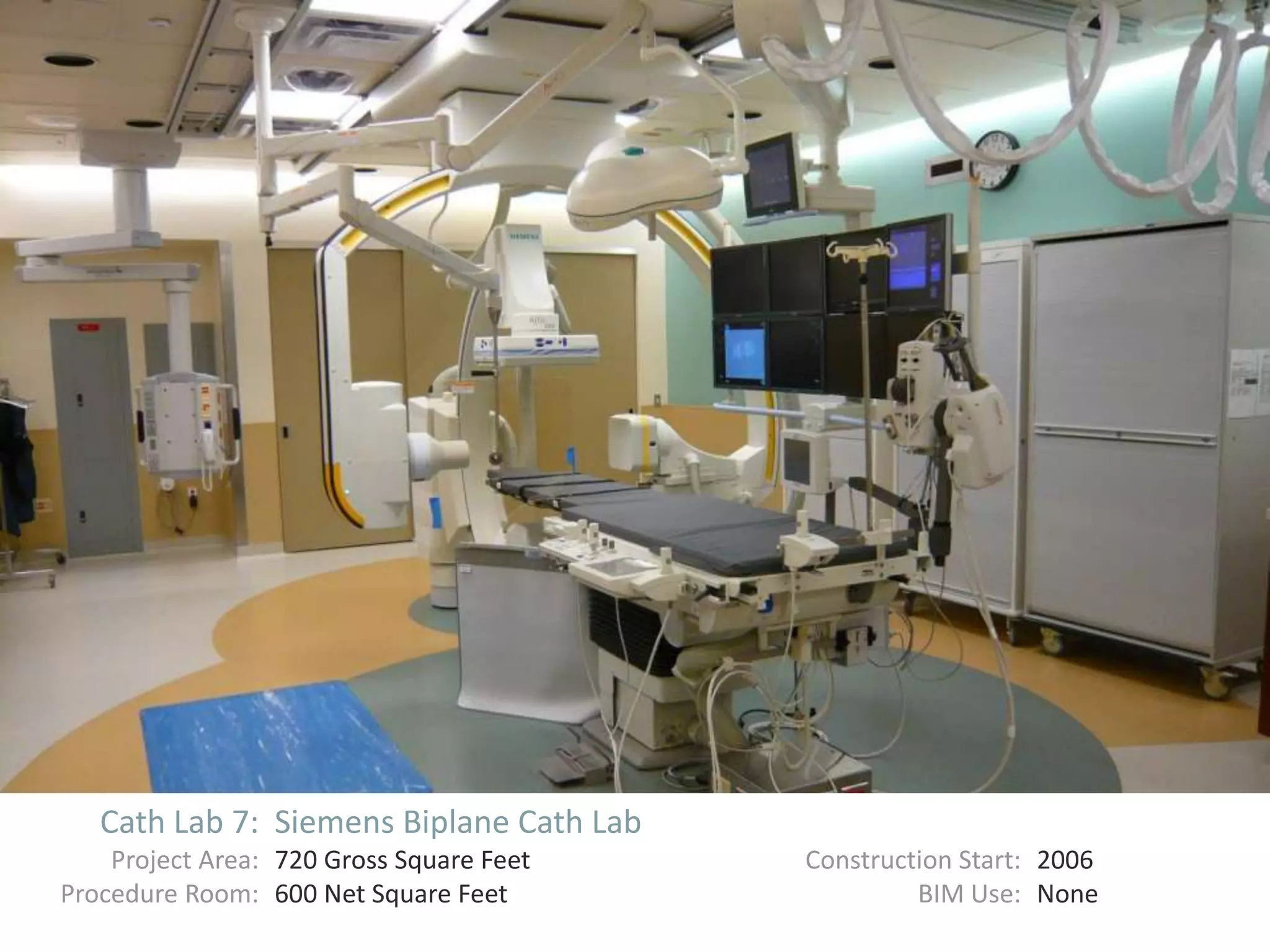
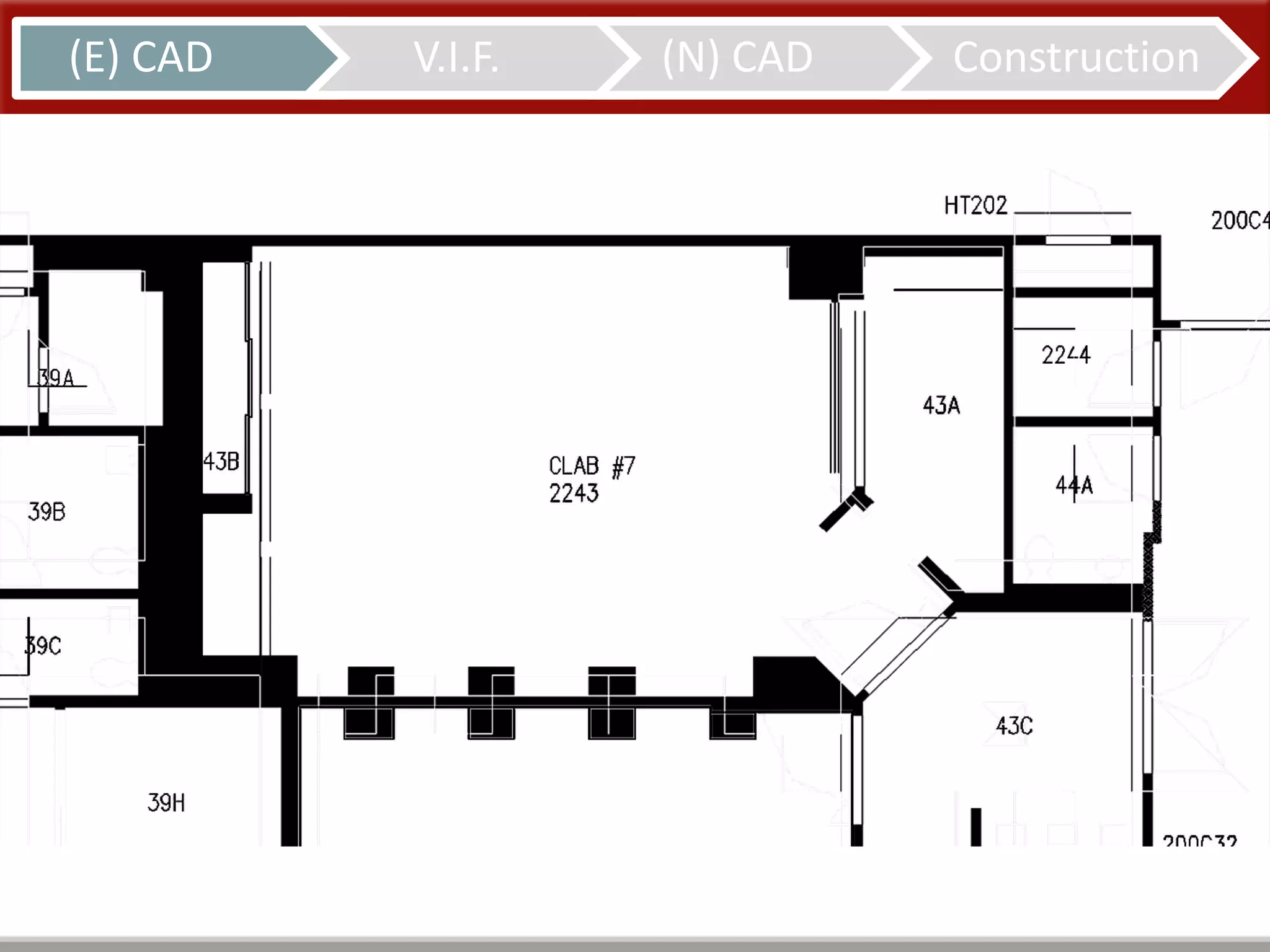
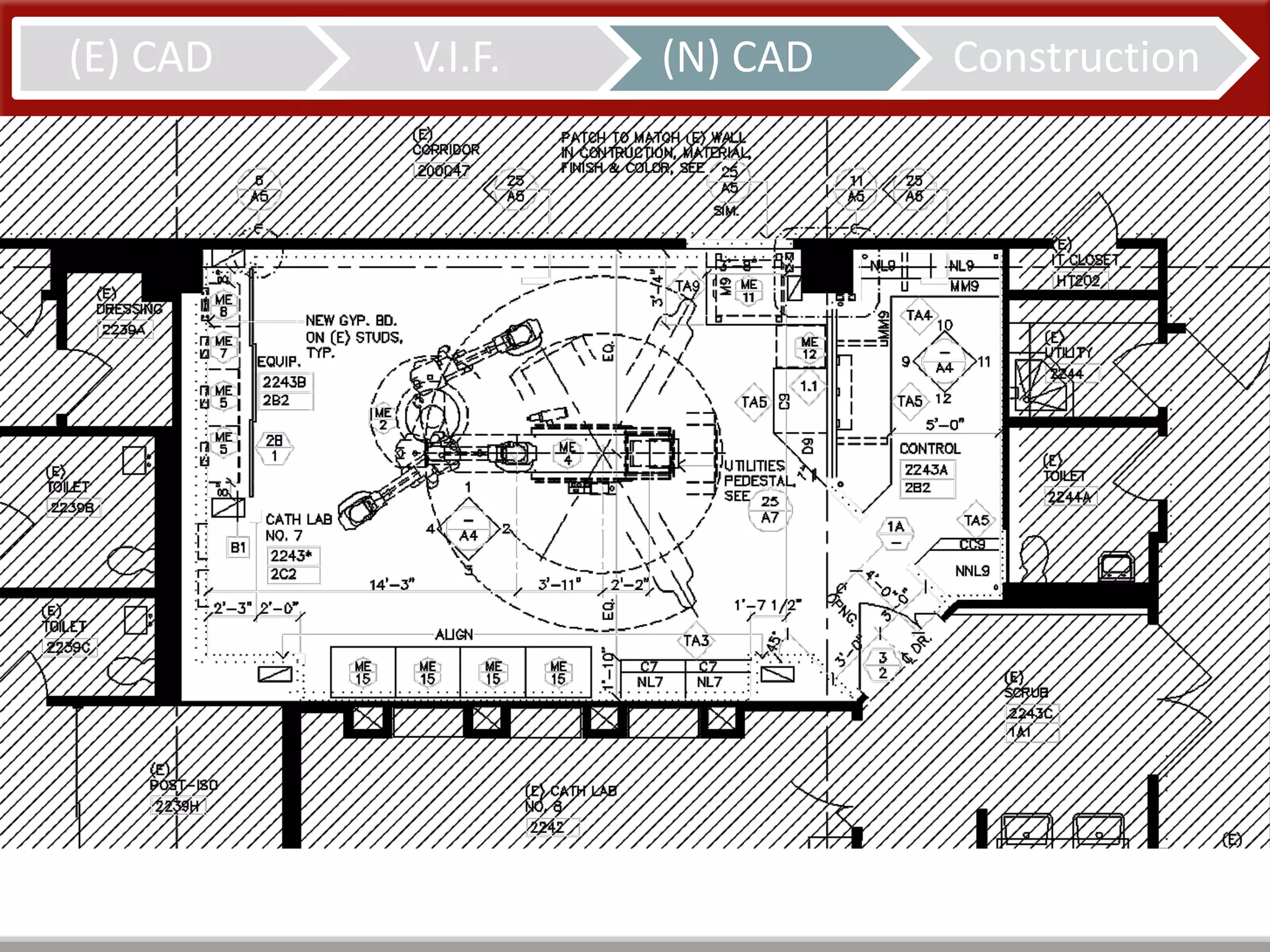
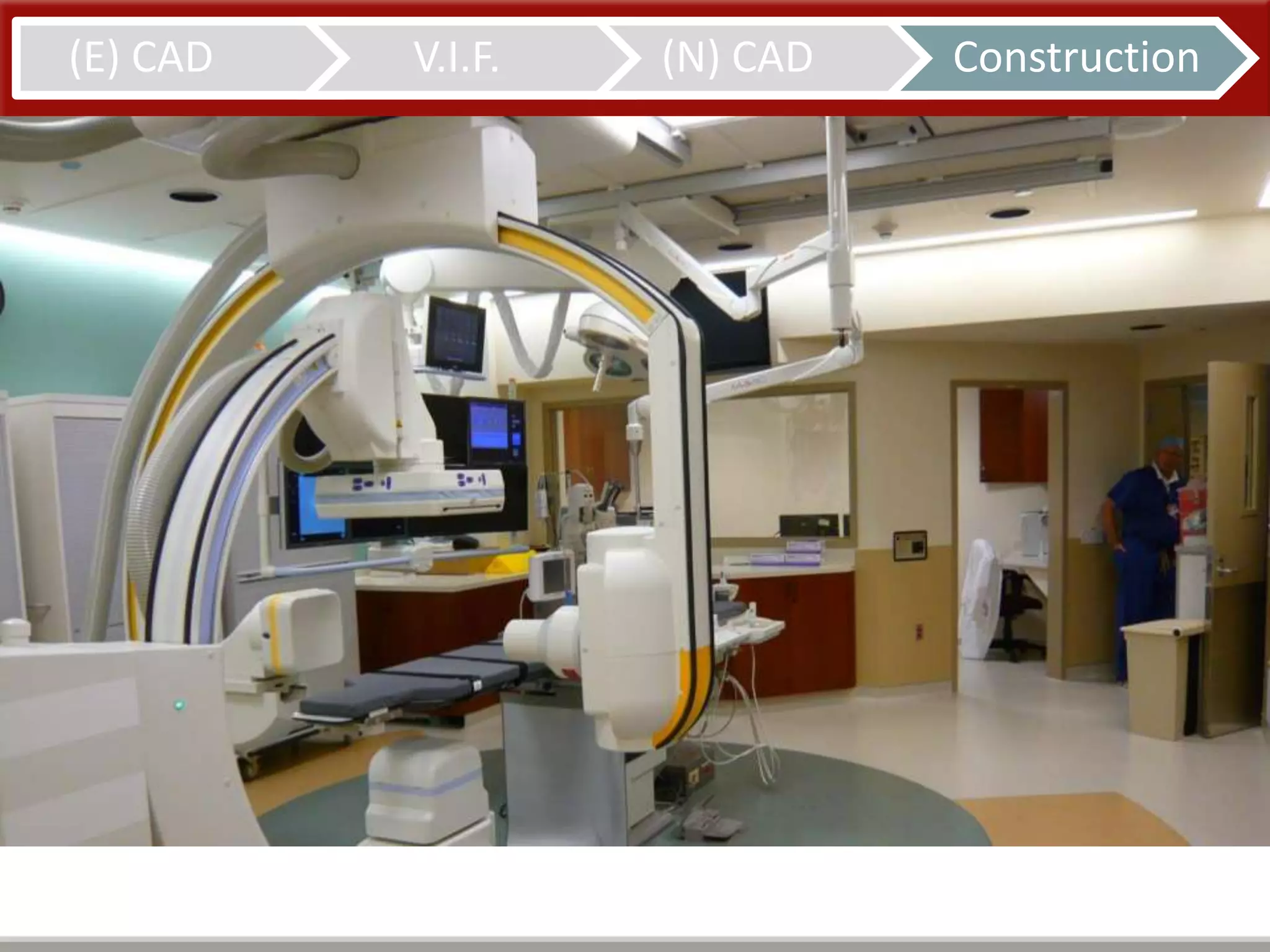
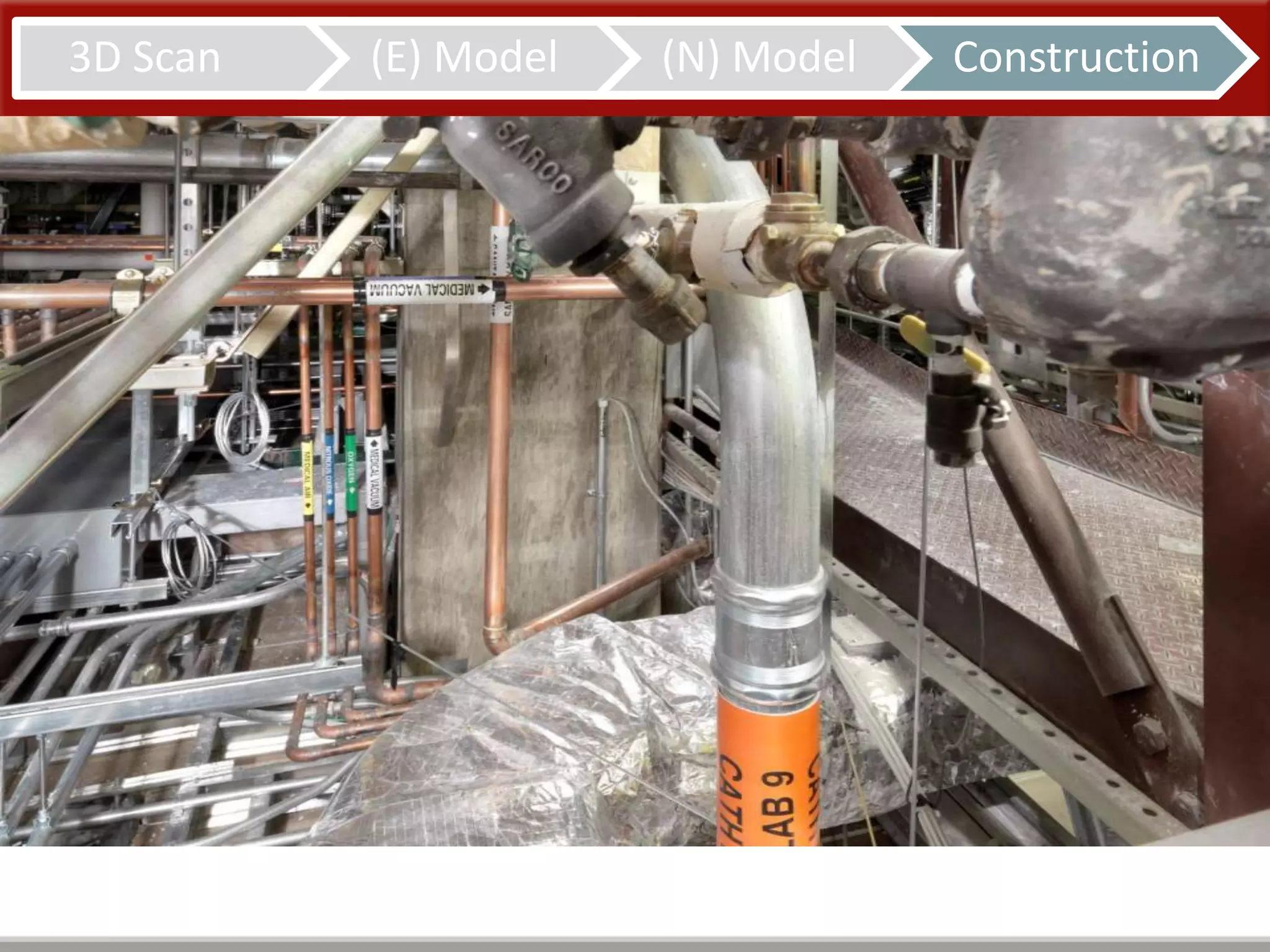
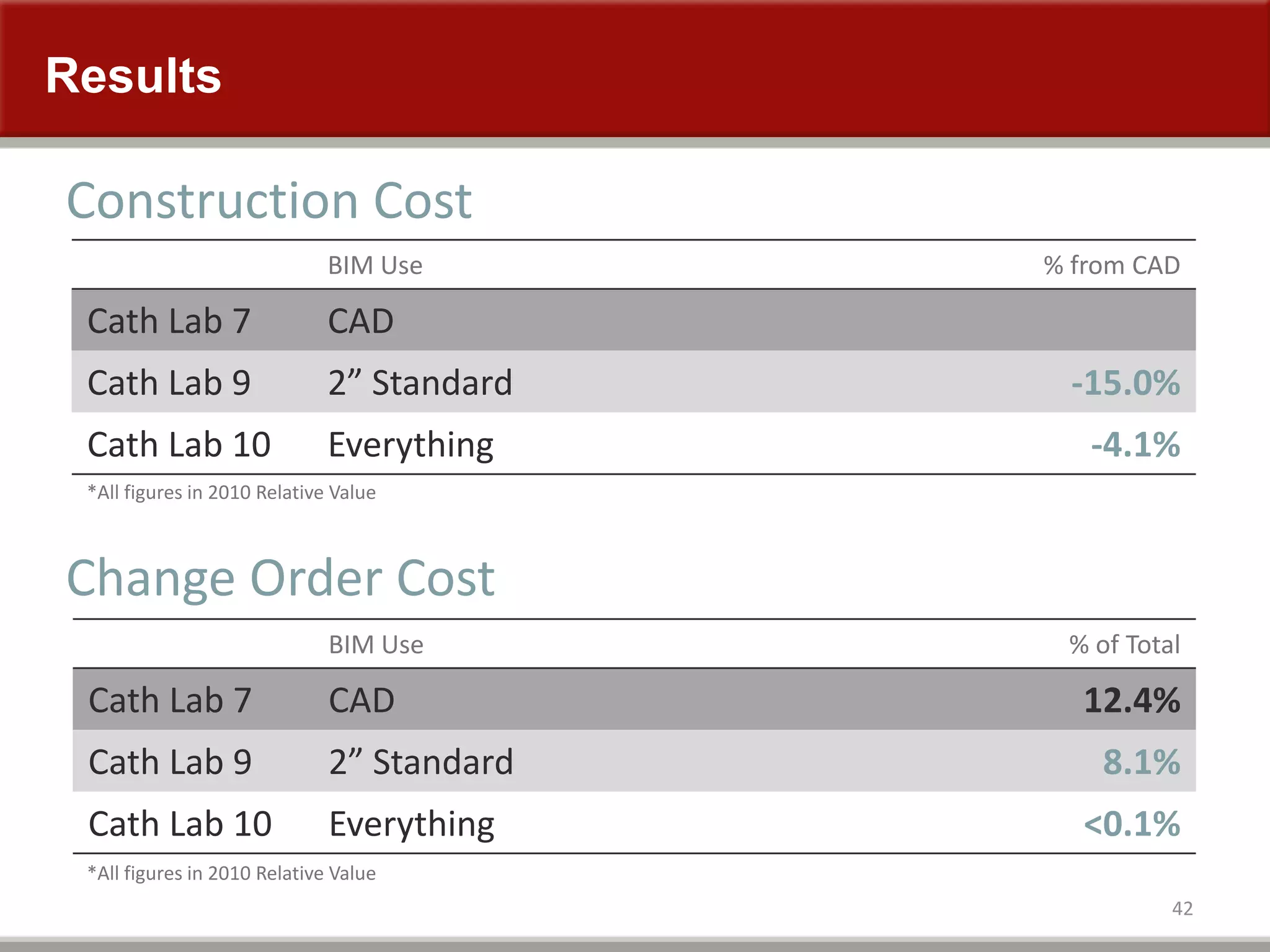
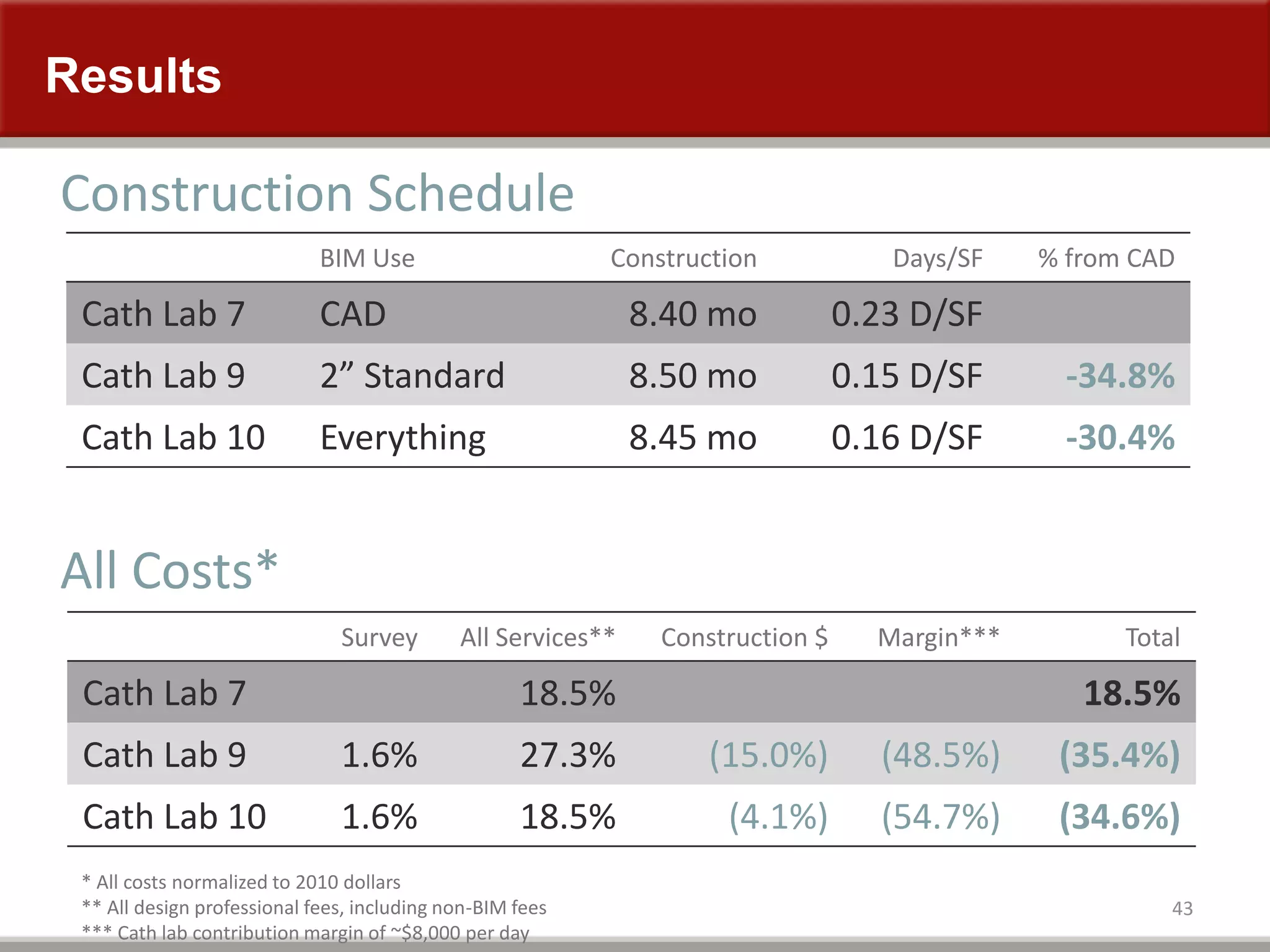
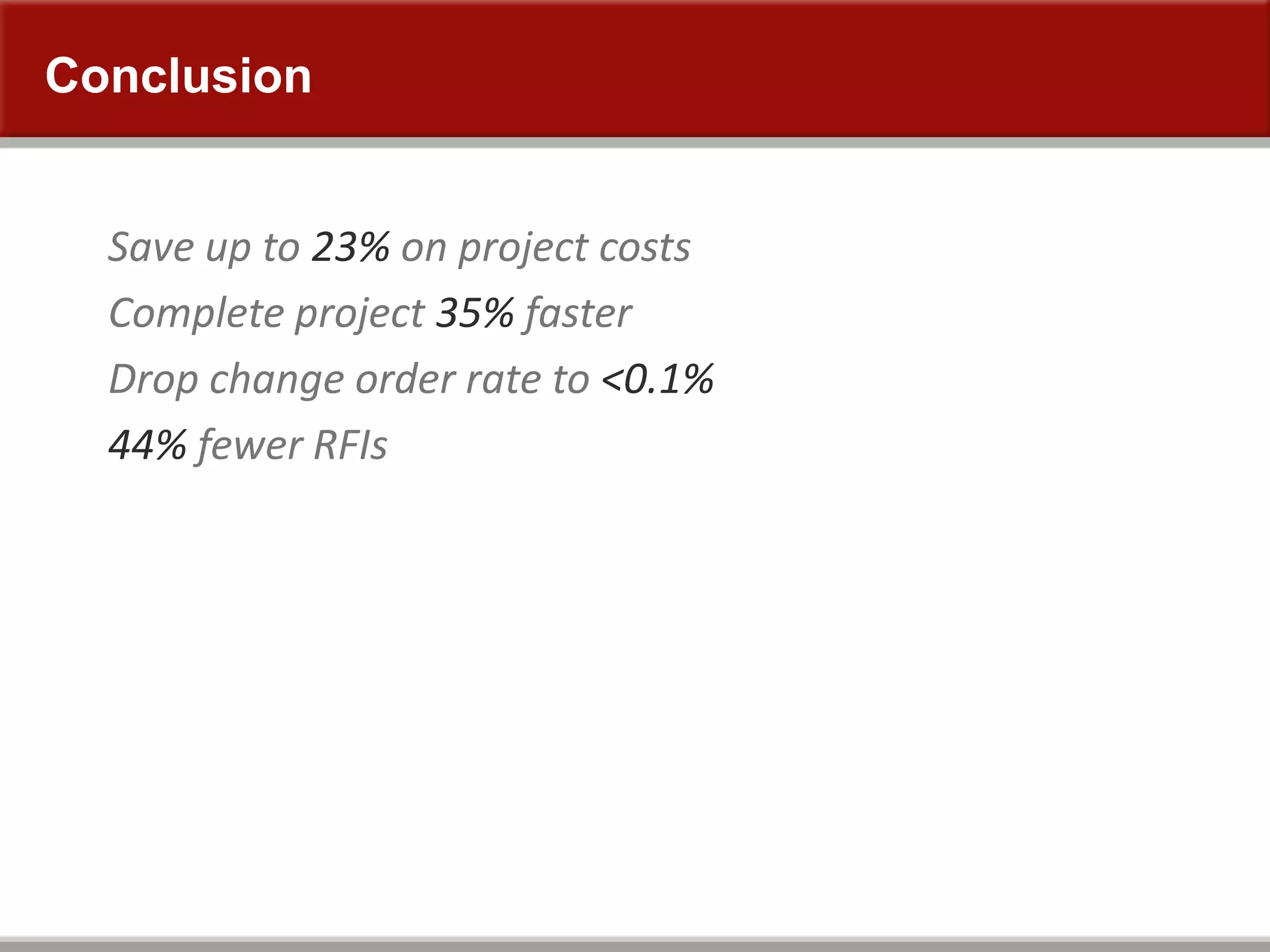
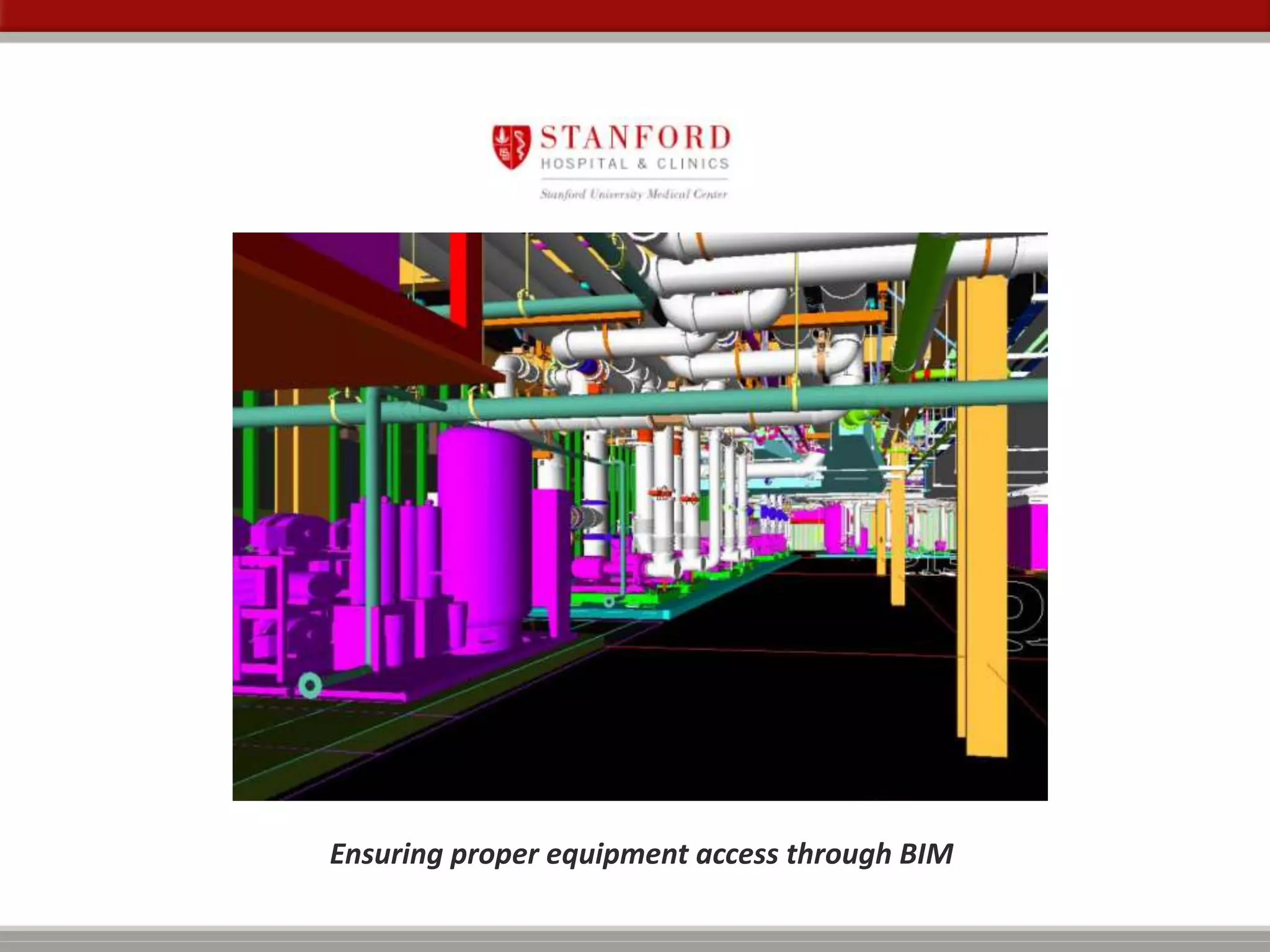
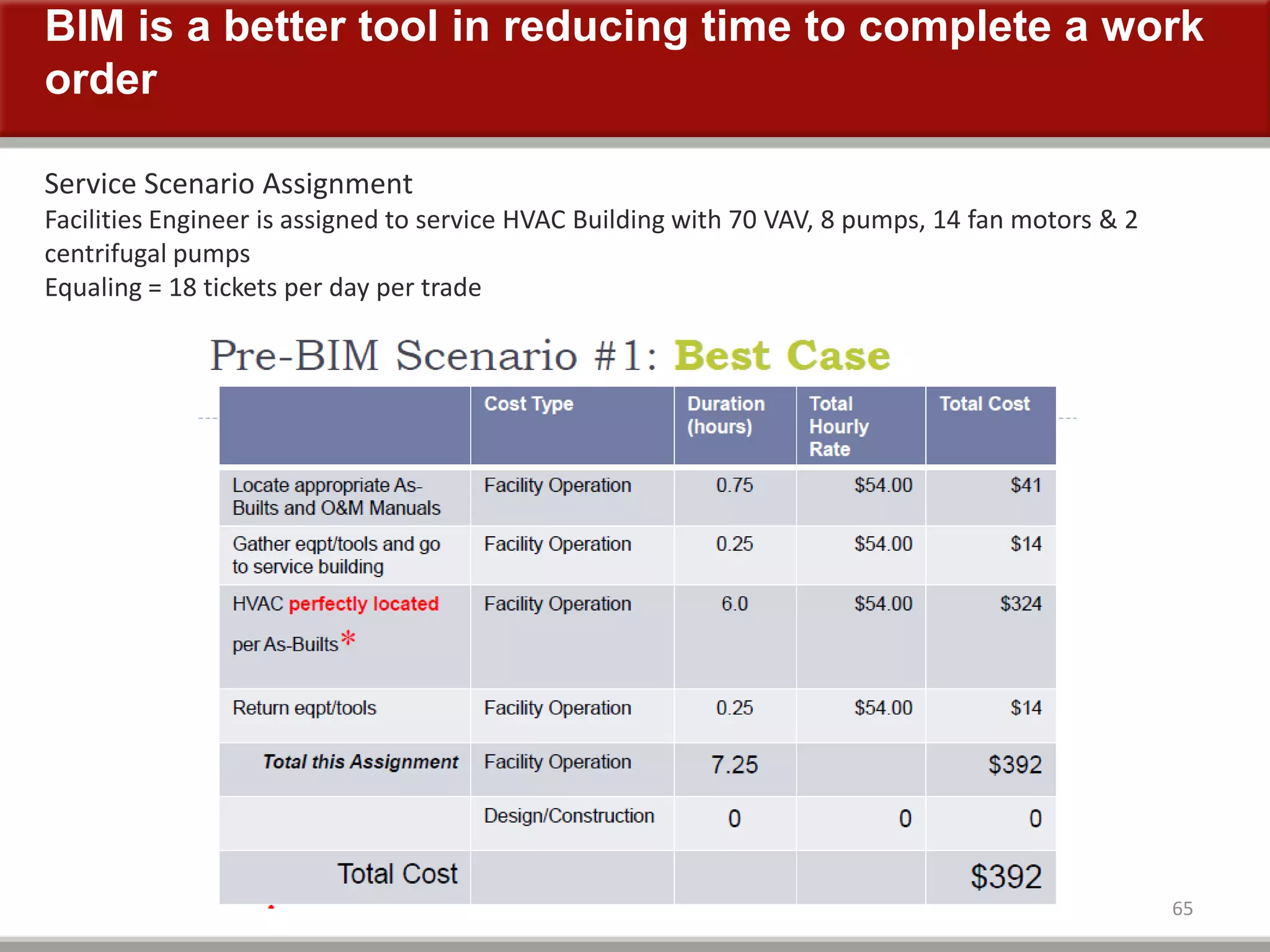
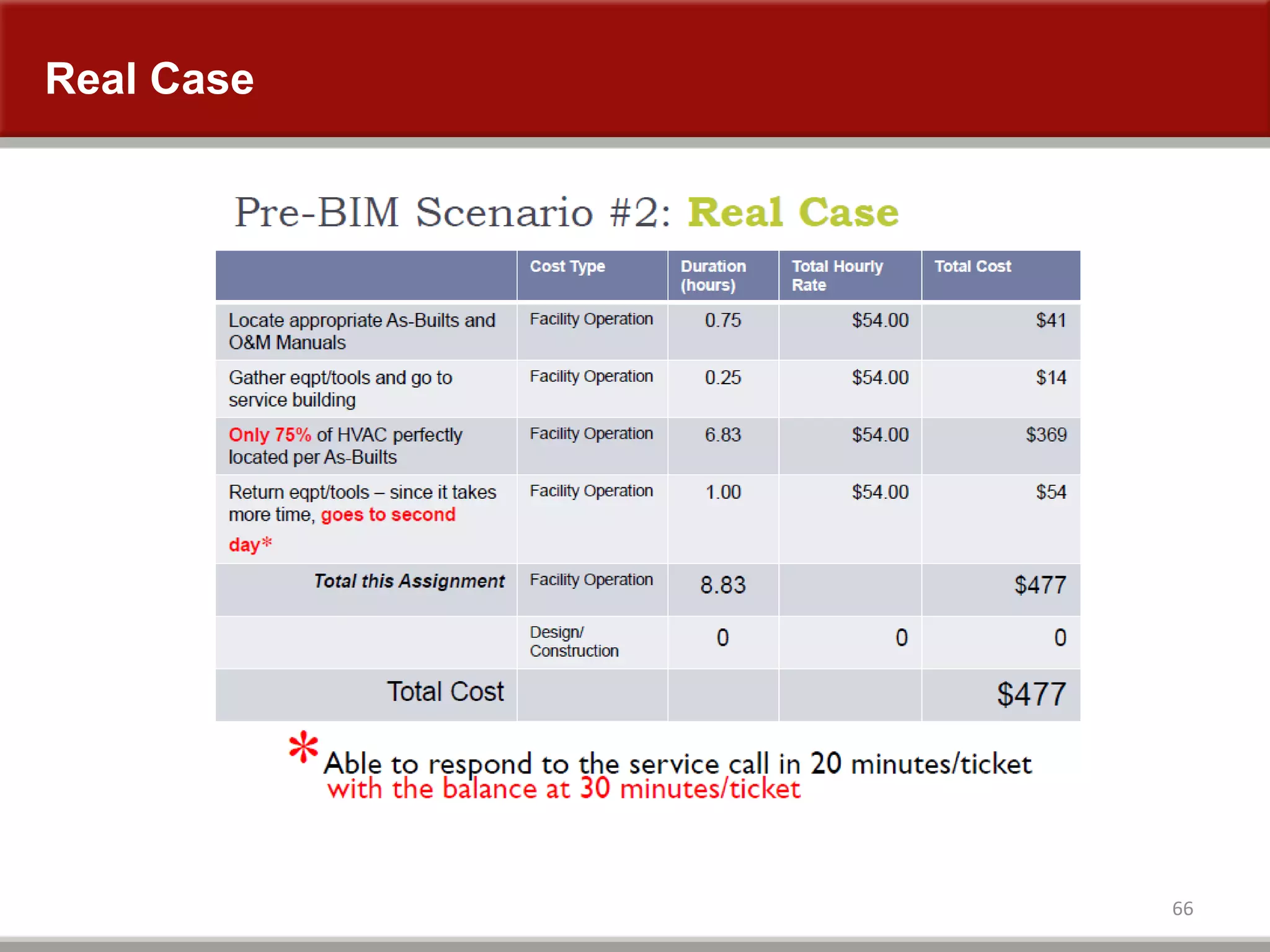
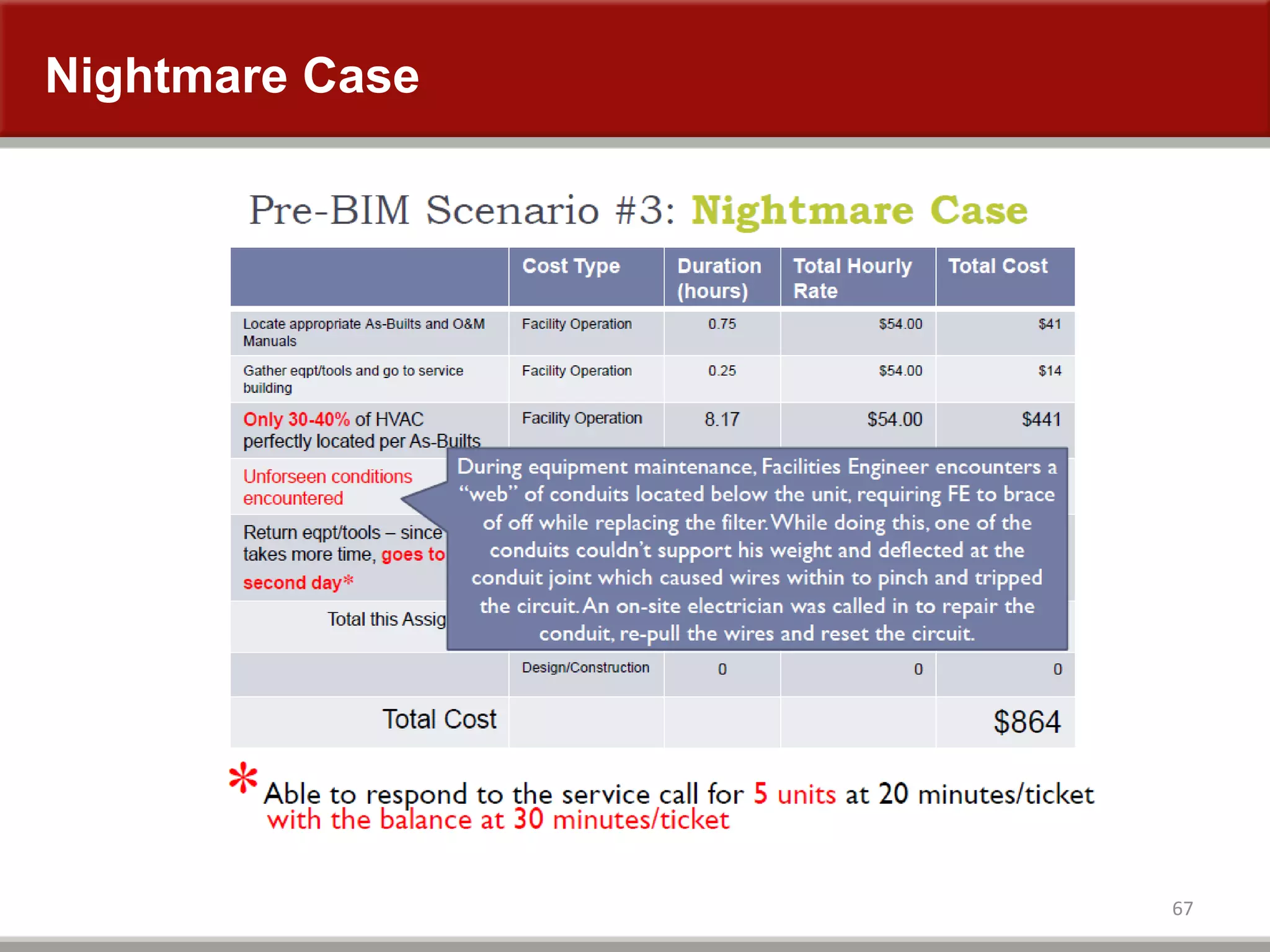
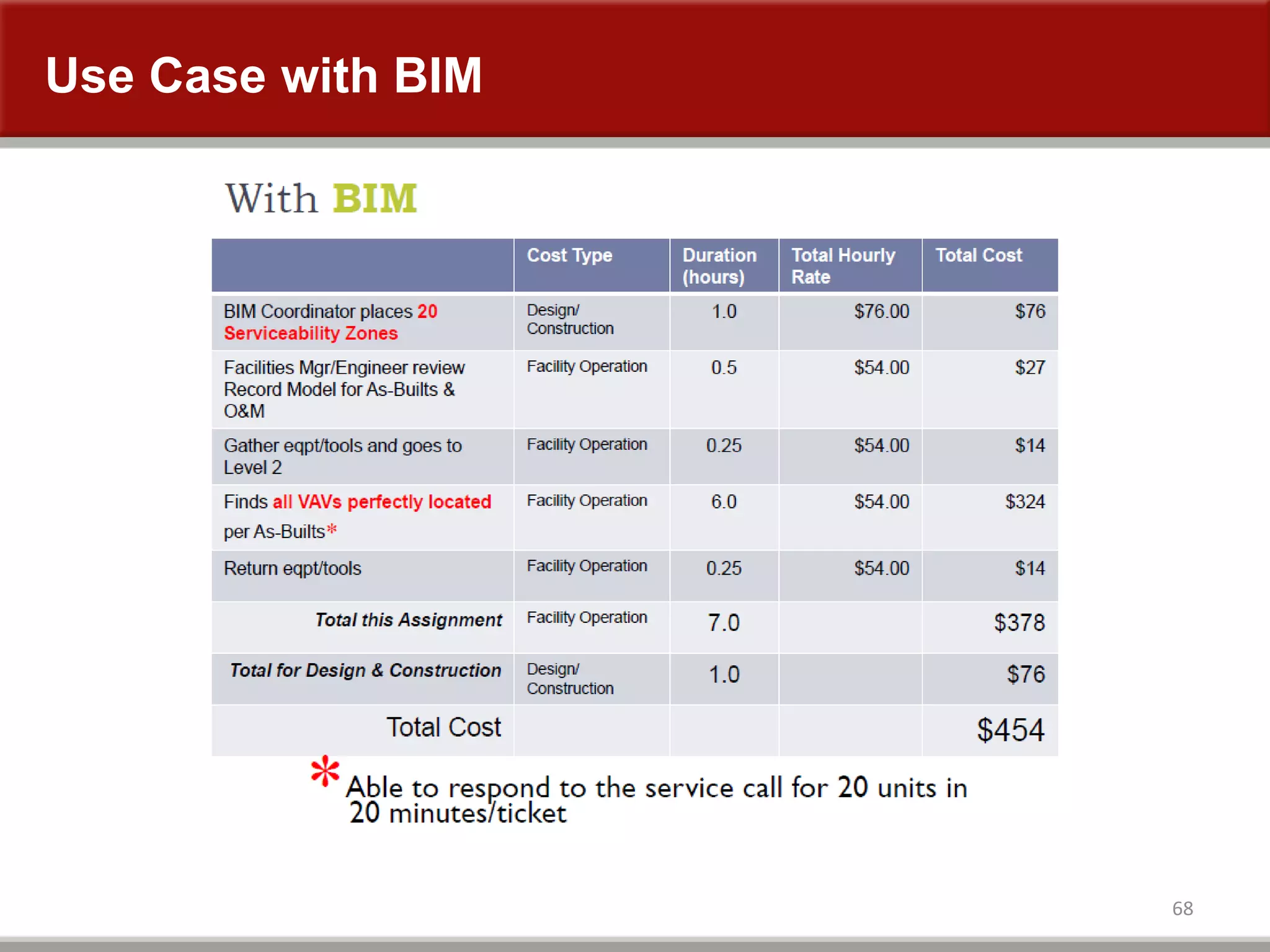
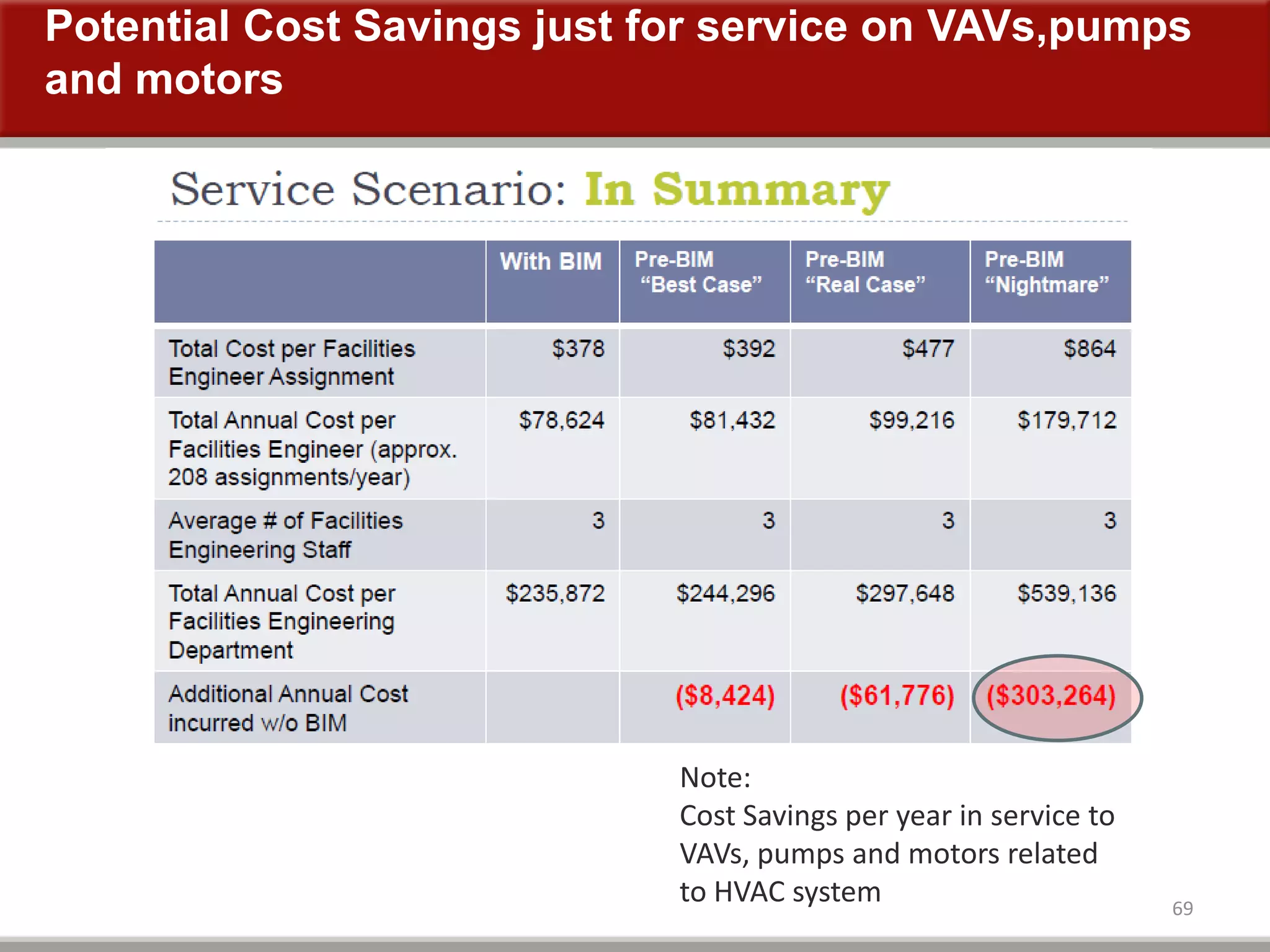
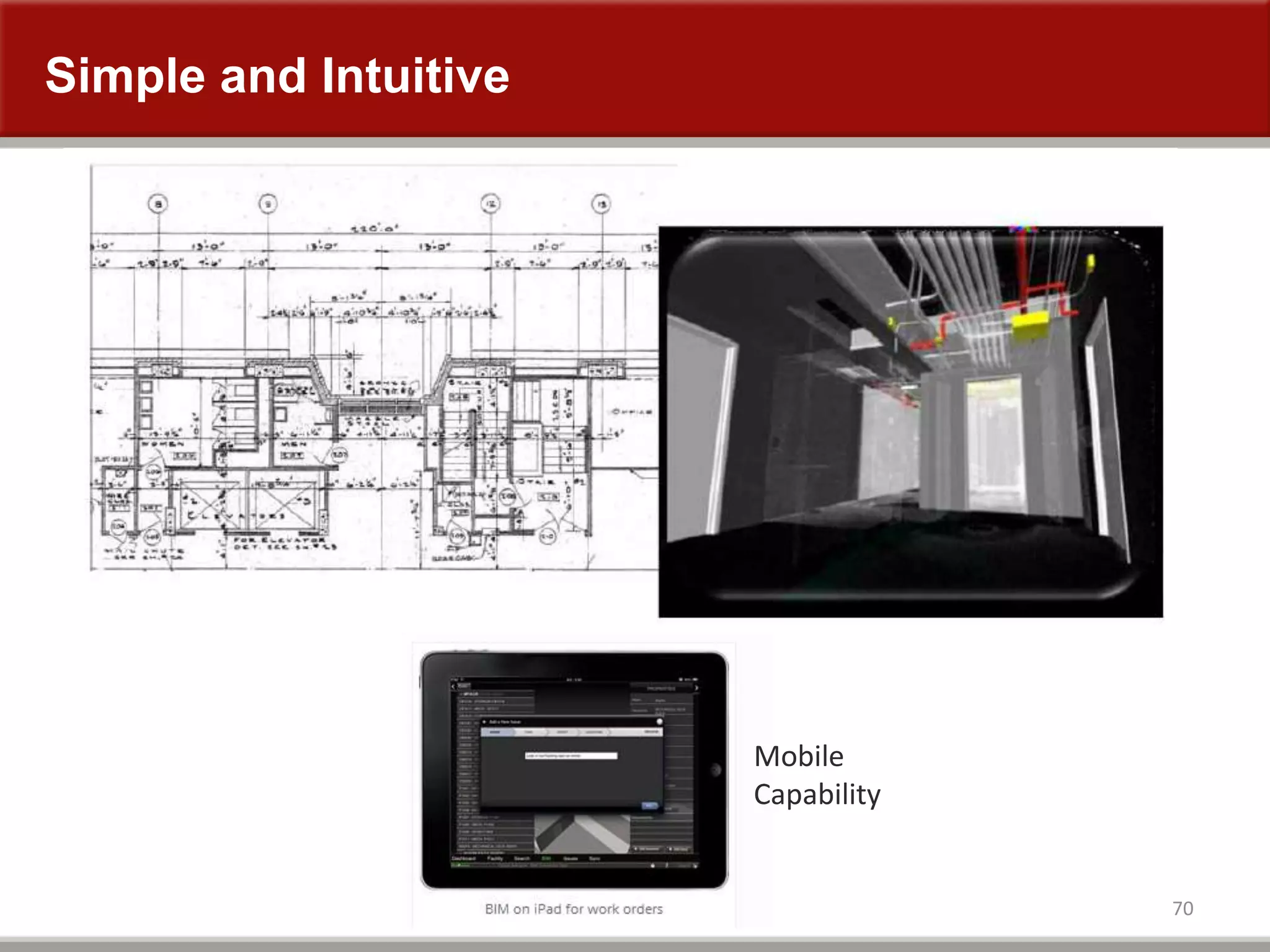
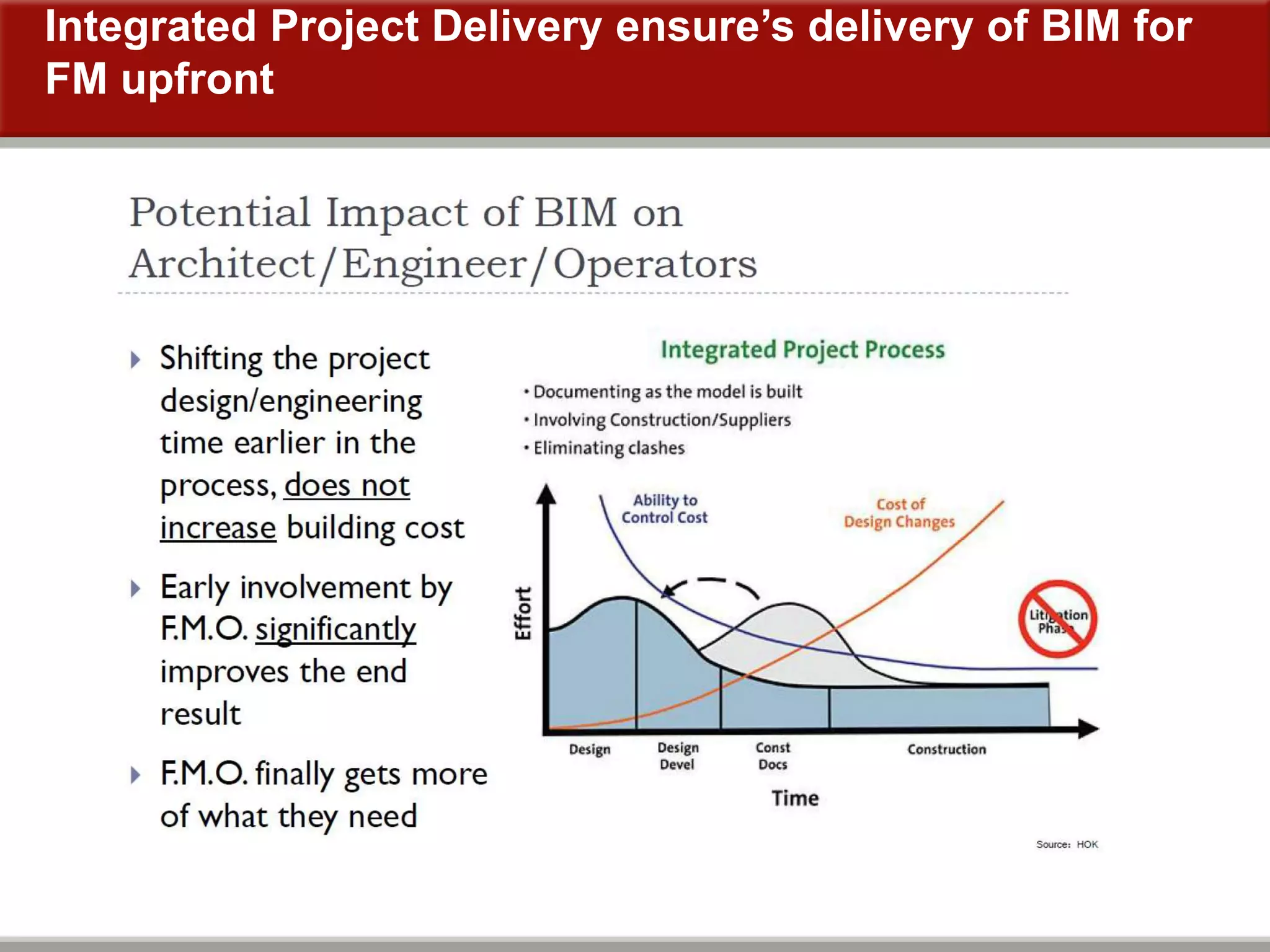
The document discusses BIM implementation at Stanford Hospital and Clinics. It provides information on various construction projects including an existing hospital, new hospital, advanced medicine center, and LPCH expansions. It details the square footage of each project and presents data comparing the use of CAD versus BIM on three catheterization lab projects, finding that BIM led to lower costs, faster completion times, and fewer changes and requests for information. The document advocates establishing BIM procedures and guidelines to ensure proper access to mechanical, electrical, and plumbing equipment. It also discusses using BIM to support facilities management by integrating it with work order and asset management systems.