Beth Israel newsletter on acid reflux surgery
•
1 like•390 views

Minimally invasive fundoplication surgery provides relief for many patients with persistent GERD. The standard laparoscopic fundoplication procedure performed at Beth Israel Medical Center since 1995 involves wrapping and stitching the stomach around the distal esophagus to recreate a functioning sphincter and alleviate heartburn in up to 90% of cases. While medications only reduce acid production and do not correct anatomical issues causing reflux, fundoplication surgery both relieves symptoms and repairs defects by tightening the lower esophageal sphincter. Transoral incisionless fundoplication is a newer minimally invasive approach being explored that deploys fasteners through the esophagus to create a valve without external inc

More Related Content
Similar to Beth Israel newsletter on acid reflux surgery
Similar to Beth Israel newsletter on acid reflux surgery (20)
More from Ben Gurion University of the Negev
More from Ben Gurion University of the Negev (20)
Recently uploaded
Recently uploaded (20)
Beth Israel newsletter on acid reflux surgery
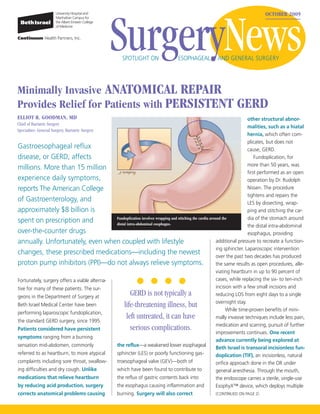
- 1. SurgeryNews OCTOBER 2009 SPOTLIGHT ON ESOPHAGEAL AND GENERAL SURGERY Minimally Invasive ANATOMICAL REPAIR Provides Relief for Patients with PERSISTENT GERD ELLIOT R. GOODMAN, MD other structural abnor- Chief of Bariatric Surgery malities, such as a hiatal Specialties: General Surgery, Bariatric Surgery hernia, which often com- plicates, but does not Gastroesophageal reflux cause, GERD. disease, or GERD, affects Fundoplication, for more than 50 years, was millions. More than 15 million first performed as an open experience daily symptoms, operation by Dr. Rudolph reports The American College Nissen. The procedure tightens and repairs the of Gastroenterology, and LES by dissecting, wrap- approximately $8 billion is ping and stitching the car- dia of the stomach around spent on prescription and Fundoplication involves wrapping and stitching the cardia around the distal intra-abdominal esophagus. the distal intra-abdominal over-the-counter drugs esophagus, providing annually. Unfortunately, even when coupled with lifestyle additional pressure to recreate a function- ing sphincter. Laparoscopic intervention changes, these prescribed medications—including the newest over the past two decades has produced proton pump inhibitors (PPI)—do not always relieve symptoms. the same results as open procedures, alle- viating heartburn in up to 90 percent of Fortunately, surgery offers a viable alterna- cases, while replacing the six- to ten-inch tive for many of these patients. The sur- incision with a few small incisions and geons in the Department of Surgery at GERD is not typically a reducing LOS from eight days to a single overnight stay. Beth Israel Medical Center have been life-threatening illness, but While time-proven benefits of mini- performing laparoscopic fundoplication, the standard GERD surgery, since 1995. left untreated, it can have mally invasive techniques include less pain, medication and scarring, pursuit of further Patients considered have persistent serious complications. improvements continues. One recent symptoms ranging from a burning advance currently being explored at sensation mid-abdomen, commonly the reflux—a weakened lower esophageal Beth Israel is transoral incisionless fun- referred to as heartburn, to more atypical sphincter (LES) or poorly functioning gas- doplication (TIF), an incisionless, natural complaints including sore throat, swallow- troesophageal valve (GEV)—both of orifice approach done in the OR under ing difficulties and dry cough. Unlike which have been found to contribute to general anesthesia. Through the mouth, medications that relieve heartburn the reflux of gastric contents back into the endoscope carries a sterile, single-use by reducing acid production, surgery the esophagus causing inflammation and EsophyX™ device, which deploys multiple corrects anatomical problems causing burning. Surgery will also correct (CONTINUED ON PAGE 2)
- 2. BI Surgeons TREAT GERD RARE ESOPHAGEAL DISORDER (CONTINUED FROM PAGE 1) polypropylene fasteners, transfixing and BURTON G. SURICK, MD Attending, Department of Surgery achieving serosa-to-serosa fusion, creating Specialties: General Surgery, Minimally Invasive Laparoscopic Surgery, Bariatric Surgery a functional gastroesophageal valve. Most patients who opt for GERD surgery are In direct contrast to GERD, achalasia is a rare esophageal disorder suitable candidates for traditional laparo- scopic fundoplication. The EsophyX™ resulting from an overly tight lower esophageal sphincter (LES), procedure is appropriate for those which keeps food from passing through. Only 2,000 people without large hiatal hernias (over 2 cm), esophageal strictures, or significant scar- develop this condition annually in the US, according to The ring from prior abdominal surgery. Society of Thoracic Surgeons, but untreated it has unpleasant All patients undergo careful consequences. Fortunately, surgeons like Beth Israel Medical evaluation and screening. Good motility in the esophagus, determined Center’s Burton Surick, MD, and Richard Friedman, MD, are by manometry testing, is required, as is performing a minimally invasive surgery with great success. eliminating a cardiac diagnosis, which can sometimes mimic GERD symptoms. Endoscopic evaluation and an upper GI series is standard to view the esophagus surface and check for abnormalities. Additional tests performed include 24-hour pH monitoring, done on an outpatient basis to record acid levels while a patient goes about normal activities. GERD is not typically a life-threatening illness but, left untreated, it can have A: Failure of the valve at the lower esophageal sphincter (LES) results in food entrapment and distension of the esophagus. B: Myotomy requires splitting the LES muscle to release the valve and allow food passage into the serious complications, including bleeding, stomach. C: A portion of the cardia is repositioned and reattached over the site of the incision. ulcers, strictures, and Barrett’s esophagus, a pre-cancerous condition that can even- tually lead to a fatal outcome. Palliative Called a myotomy, the procedure involves Symptoms of achalasia may include medical management does not correct splitting the LES to disrupt the muscle progressive difficulty in swallowing, eating the problem, and lifelong treatment and fibers, allowing food to pass more easily and drinking, the need to wash food monitoring is necessary to prevent deteri- into the stomach. As an open surgery, down with liquids, regurgitation of food, oration. Anatomical repair offers cure, myotomy has been performed for decades. heartburn, chronic cough, weight loss, and and incisionless advances reduce OR The laparoscopic approach, initially used in chest pain or pressure that may increase risks, potentially prompting physicians the 1990s, has proved highly successful— after eating, or radiate to the back, neck and their patients to opt for surgical inter- nearly 95 percent of patients experience and arms. Patients with these complaints, vention earlier. years of symptom relief afterwards. Other which can appear similar to GERD, under- treatments include application of an endo- go complete evaluations that include scopic balloon within the LES that expands esophageal endoscopy and manometry. For further information or to refer a and tears the valve muscles, and a Botox patient for surgical GERD intervention, injection administered under endoscopic please contact Elliot Goodman, MD, at guidance that paralyzes the valve. But For further information about achalasia neither provides relief for as long, or for as or to refer a patient to Burton Surick, MD, (212) 844-8838. many patients as does myotomy. Currently, or Richard Friedman, MD, please call no oral medications are available either. (212) 420-4520. 2
- 3. Beth Israel’s GENERAL SURGERY SPECIALISTS Provide ADVANCED CARE FROM A TO Z MICHAEL LEITMAN, MD Chief of General Surgery Specialties: Oncologic Surgery, Bariatric Surgery General surgery specialists at Beth Israel Medical Center treat thousands of patients each year. Providing interventions for a wide range of conditions from appendicitis to obesity, these physicians treat diseases affecting the abdomen and its organs. Individualized treatment plans, increasingly with minimally invasive surgery (MIS), a multidisciplinary team approach, and collaboration with referring physicians, are all hallmarks of the division. What is general surgery? Recent laparoscopic advances Key Administration In spite of its name, general surgery is a Further refinements to MIS include single surgical specialty that focuses on the incision laparoscopic surgery (SILS), diagnosis and treatment of diseases and MARTIN KARPEH, MD involving the application of a special disorders affecting the abdomen, digestive Chairman, Department of Surgery device at the navel that accommodates (212) 420-4041 tract and endocrine system. The most the three necessary instruments for chole- common conditions treated by Beth Israel MERYL GOLD cystectomy, a technique in use at Beth surgeons include gallstones and other Administrator, Department of Surgery Israel for the past six months. Another gall bladder disease, a variety of hernias (212) 420-4457 advance, natural orifice endoscopic (inguinal, recurrent, bilateral, ventral, surgery, performed with an endoscope KATHERINE ZAYAS and incisional), obesity, pancreatitis, Administrator, Ambulatory Surgery through one of the body’s natural orifices, appendicitis, bowel obstructions, colon (212) 844-8203 includes the EsophyX™ and StomaphX™ inflammation and cancer, and trauma. procedures, which treat gastroesophageal The broad perspective of these spe- reflux and revise gastric bypasses, respec- cialists enhances comprehensive and A Vast Array of Treatments tively. Over the past year, Beth Israel has thorough diagnosis, and allows for the established itself as a leader in the metro- most skillful surgical solutions possible. The General Surgery Division provides politan area, performing more than 70 laparoscopic as well as open treatments for StomaphX™ procedures with good results. patients with: Minimally invasive • Hernia In addition to improving care through treatment is preferred • Gallbladder disease and gallstones technical advances, the collegial environ- Over the last 15 years, these solutions • Gastro-esophageal reflux disorder (GERD) ment of Beth Israel Medical Center, and • Pancreatitis the Division of General Surgery in particu- have increasingly involved minimally • Appendicitis invasive surgery (MIS). Well-established lar, provides superior patient care via • Diverticulitis disease benefits for both physician and patient • Inflammatory bowel disease collaboration between different specialties. hone in on one central principle— • Biliary (liver) diseases Treating obesity, for example, necessitates • Trauma partnerships among endocrinologists, reducing surgical risk. Smaller incisions and reduced trauma translate to fewer behavioral specialists and general surgeons. Additionally, within the Division of wound complications, less post-op pain, General Surgery, is the following specialized less pain medication, shorter LOS, faster program: • Bariatric Surgery Program recovery and fewer scars. MIS techniques For further information on general are now standard care for many proce- surgery services or to schedule a consulta- dures including cholecystectomy, Nissen www.BISurgery.org tion with a general surgeon, please call fundoplication and hernia repair. (212) 844-8203. 3
- 4. NONPROFIT ORGANIZATION US POSTAGE PAID PERMIT NO. 8048 NEW YORK, NY Beth Israel Medical Center First Avenue at 16th Street New York, NY 10003 In this issue... Laparoscopic Treatments for GERD; Treating the Rare Disorder of Achalasia; Advanced General Surgery Care from A to Z SurgeryNews OCTOBER 2009 SPOTLIGHT ON ESOPHAGEAL AND GENERAL SURGERY Is a DIGITAL Copy of Surgery News in your Future? The Department of Surgery is planning to go digital with future issues of Surgery News. If you would like to receive future copies electronically, please drop us an e-mail with “Electronic SN” in the subject line. Simply provide your full name, address, medical specialty and e-mail address to: paphilippe@chpnet.org. Beth Israel surgeons provide first-rate, state-of-the-art quality care to all patients and collaborate with referring physicians to create an individualized treatment plan. For more information about surgical services at Beth Israel Medical Center, call (212) 420 - 4044 or visit our Website at www.BISurgery.org. 4