The document provides an extensive overview of behavioral sciences in healthcare, emphasizing the integration of psychology, sociology, and anthropology with traditional medical practices. It discusses various health care models, including the bio-psycho-social model and the integrated model, which highlight the importance of understanding the interactions between biological, psychological, and social factors in health and illness. Additionally, it addresses non-pharmacological interventions, medical ethics, and the psychosocial aspects of patient care, advocating for a holistic approach to medicine.














































![Eysenbach G, ]adadAR
Evidence-based Patient Choice
and Consumer heatth
informat/cs in the Internet age
] Med Internet Res 2001,3t2):e19
URL: http://wwwjmit
org/2001/2/e19
DOl: lo.2196/jmir.3.2.e19
PMID: 11720961
PMCID: PMC1761898
5. Doctor-Patient Relationship
Ifyou have come to hetp me
You are wasting your time
But ifyou hove come because
Your tiberation is bound up with mine
Then let us work together
- An Australian Aborigine’s statement to a Doctor
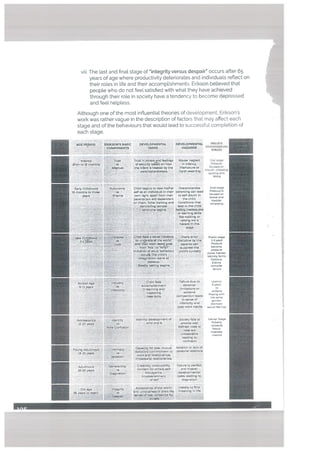
The basis of the unique relationship between doctor and patient is the
capacity of the doctor to appreciate the complexity of human behaviour. A
doctor must be sensitive to the effects of history, culture, and environment
on his patients. At the center of this therapeutic retationship is the trust that
a patient has in the doctor, This trust is built on the unconditionaL positive
regard that the doctor holds for the patient, irrespective of their gender,
social class, caste, colour or creed. The bond that forms in the relationship
can take three forms:
The vertical model, where the doctor completely takes over the
process of care with the patient having virtually no role e.g. when a
patient is unconscious, immobilised or in an altered state of con
scious, or is incapacitated.
The teacher-student model, where the doctor plays a roLe similar to
that of an authority figure (such as a teacher or a parent), who dom
inates, controls and guides the patient e.g. in the case of a patient -
recovering from a surgical intervention.
The mutual participation, horizontal modeL where the doctor and
the participation behave as partners in the process of healing and
care. Each augments and supports the other’s effort. The patient in
this is fully aware and informed and plays an active role in the treat
ment process e.g. a patient of diabetes metlitus who understands
the nature of his/her illness and undertakes lifestyle changes to
manage it with the doctor’s cooperation. is an active partner in the
management process.
C
‘4(1’-”
/
- j
F,b
/
ZL:Z
; 2
48](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-53-320.jpg)


















































![The orbitofrontal cortex (so called because it represents the area above
the orbits) plays an important role in emotional regulation, specifical
ly anger management. It functions to associate possible outcomes of a
certain behaviour by weighing pros and cons based on reward and pun
ishment and makes a decision. Iii In one study people with more outgoing
personalities were found to have higher volume orbitofrontal cortex, while
more introverted people were found to have a higher volume ventromediat
prefrontal cortex. [2]
A part of the cingulate cortex, the anterior cingulate cortex (ACC) is the area
where the integration of emotional input with attention occurs. It, therefore,
controls emotional arousal and emotional self-controL It is involved in gen
erating empathy and social awareness and becomes active when individu
als indulge in acts of bravery. [41
To summarise, the prefrontal cortex (the smart’ part of the brain), takes into
account the emotions elicited and decides the most logical and rational
action to take in a situation. 171
The limbic system, specifically the amygdala, works to integrate inputs
from the thalamus and frontal cortex with outputs involving the endocrine
and autonomic nervous systems. This results in the expression of emotion.
• The amygdala is the main mediator of the fight, flight or freeze response.
It is invo[ved in the mediation of aggression, fear, sexuaL orientation and
social interaction, including the number and kind of people one is friends
with and interacts with in a social context. It also regulates personal space,
in that it is stimulated when another human being gets “uncomfortably
close.” [81
The right lobe of the amygdala houses negative emotions such as fear and
anxiety. The left lobe, on the other hand, mediates and stores both positive
emotions such as pleasure and happiness and negative emotions such as
fear. In one study, poLitical conservatism was linked to increased volume of
the right amygdala. [9]
Distinct gender differences have been seen in the male and female amyg
data. The mate amygdata has a larger right lobe, while the female amygda
Ia has a larger left lobe. As the right lobe is associated with negative emo
tions and action, men are more likely to react physically in situations that
are emotionally stressful. The left lobe is important in the recall of emotion
ally charged memories and details, leading to more intense thought, which
may explain why women are more likely to not react in physical ways to
emotional stress.
The amygdaLa also mediates the formation of memories that have an emo
tional content. When sensory input is received, it is relayed by the thalamus
to both the frontal cortex and the amygdata. The amygdala then checks
with the hippocampus to see if there is an emotional memory of a similar
experience. If one is found, we tend to react in a similar fashion, if not; the
prefrontal cortex kicks in to make something of the novel experience and
forms a new response. Activity of the amygdala has been linked to clinical
depression, anxiety disorders, and posttraumatic stress disorder. liD]
Despite the tact that the prefrontal cortex is the smart part of the brain, the
amygdala exerts far more control over it than the prefrontal cortex does
over the amygdata This can be understood it the amygdata is equated
with the moon which despite its size may eclipse the sun. This “limbic
eclipse” is th reason that “love is blind” “ghussa akal ko khaajaata hai”](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-115-320.jpg)


![References
i.Kringelbach, M. L. (2005) “The orbitofrontal cortex: Unking reward to he
donic experience. Nature Reviews Neuroscience 6: 691-702.
2. Schoenbaum G, Takahashi Y, Liu T, & McDannatd M (2011). “Does the orbi
tofrontat cortex signal vaLue?” Annals of the New York Academy ofSciences
1239: 87-99
3. Hu, C; Jiang, X (2014). “An emotion regulation role of ventromedial pre
frontal cortex in moratjudgment.” Front. Hum. Neurosci 8: 873. doi:10.3389/
fnhum.2o14.oo873.
4. Nicolle, A. & Goet, V. (2013). What is the role of ventromedial prefrontal
cortex in emotional influences on reason? In I. Btanchette (Ed.), Emotion
and Reasoning. Psychology Press.
5. Schwartz, Carl E., et aL “Structural differences in adult orbital and ventro
medial prefrontal cortex predicted by infant temperament at 4 months of
age.”Archives ofgeneral psychiatry 67.1 (2010): 78-84.
6. Carlson, N. (2012). Physiology of Behaviour filth Ed.). Hartow: Prentice
Hall.
.
Chan, R. C. K., Shum. D., Tou[opoutou, T. & Chen, E. Y. H., R: Shum, D: Tou
lopoulou, I; Chen, E (2008). “Assessment of executive functions: Review of
instruments and identification of critical issues.” Archives of Clinical Neuro
psychology. 2 23 (2): 201-216.
8. Kennedy, Daniel P., et al. “Personal space regulation by the human amyg
data.” Nature neuroscience 12.10 (2009): 1226-1227.
9. Kanai, Ryota, et at “Political orientations are correlated with brain struc
ture in young adults.” Current biology 21.8 (201;): 677-680.
10. Sheune, Yvette I., et at “Increased amygdata response to masked emo
tional faces in depressed subjects resolves with antidepressant treatment:
an fMRI study.” Biological psychiatry 50.9 (2001): 651-658,
ii. Peirson AR, Heuchert JW. Correlations for serotonin levels and measures
of mood in a nonctinica[ sample. Psychot Rep 2000:87:707-16,
12. Flory JD, Manuck SB, Matthews KA. et at. Serotonergic function in the
central nervous system is associated with daily ratings of positive mood.
Psychiatry Res 2004:129:11-9.
13. Muldoon MF, Mackey RH, Williams KV, et at. Low central nervous sys
tem serotonergic responsivity is associated with the metabolic syndrome
and physical inactivity. ] Clin Endocrinol Metab 2004: 89:266-71.
14. Schultz W (2007). “Multiple dopamine functions at different time cours
es.” Annual Review of Neuroscience 30: 259-88.
15. BjOrktund A, Dunnett SB (May 2007). “Dopamine neuron systems in the
brain: an update.” Trends in Neurosciences 30 (5): 194—202.
i6. Lee HJ, Macbeth AH, Pagani JH, Young WS (Jun 2009). “Oxytocin: the
great facilitator of tite.” Progress in Neurobiology 88 (2): 127-51.
17. 01ff, M.. FrUling. J. L., Kubzansky, L. D., Bradley, B., Ettenbogen. M. A., Car
doso, C & van Zuiden, M. (2013). The role of oxytocin in social bonding, stress
regulation and mental heatth: an update on the moderating effects of context and
interindividuat differences. Psychoneuroendocrinotogy, 38(9), 1883-1894.](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-118-320.jpg)
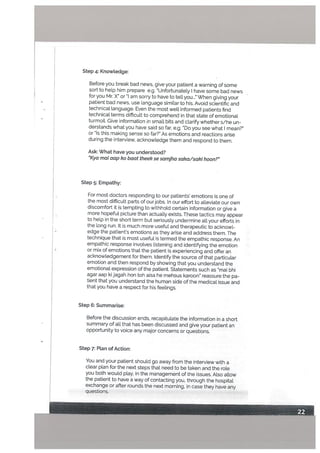
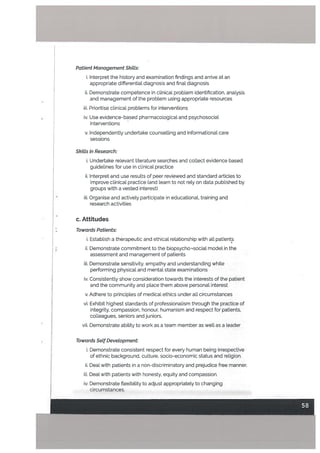
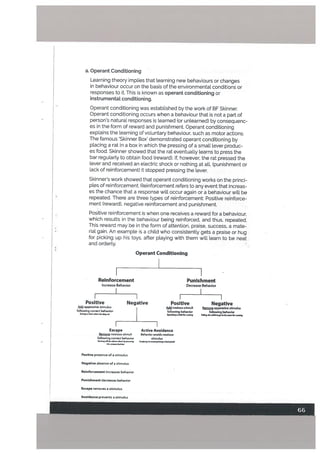
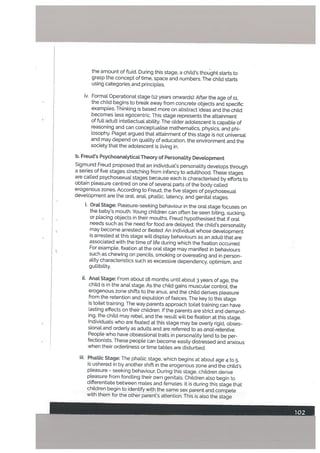
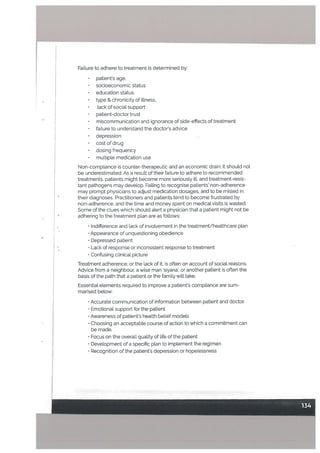
![Motor and Sensory Regions of the Cerebral Cortex
Language
Language forms a quintessential part of what it means to be human.
Human language is unique compared to the communication techniques
used by other animals. Other animats communicate using a finite num
ber of ideas that can be expressed. Human language. on the other hand,
is open-ended and productive meaning. Humans, can, thus produce an
infinite range of expressions from a finite set of elements to create new
words and sentences. [ii
Speaking is the default mode for language in all human cultures. Humans
produce language using control of the lips, tongue and the rest of the vo
cal apparatus. They are able to differentiate spoken sounds white attaching
contextual meaning to the sounds. In other words we can understand what
is being said, and what it means in a certain situation. These abilities are
[inked to a neurological apparatus to acquire and produce language. 12]
While, language is processed in various areas in the human brain, the two
areas that are mainly involved in language processing are Wernicke’s area,
located in the posterior section of the superior temporal gyrus, (temporal
lobe) and the Broca’s area, located in the posterior inferior frontal gyrus
(frontal lobe) of the dominant hemisphere. Wernicke’s area is used for lan
guage comprehension and Broca’s area is responsible for language artic
ulation. Language is the only human behavior that has two controlcentres.
thus the famous idiom pehte tolah phir boto’ (think before you speak).
Primary motor cortex
(precentr& gyms)
Somatic motor association area
(premotor cortex)
Prefrontal cortex
Sri
Broca’s area—
(production of speech)
Primary sensory cortex
(postcentml gyms)
/ Somatic sensory association area
Visual association
//_ area
Visual cortex
Auditory association area / -
--
I Wemicke’s area
Auditory cortex (understand speech)](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-119-320.jpg)

![Memory
Memory is defined as the mental capacity to encode, store, and retrieve
information. [ii
Clinically we are concerned with three, testable periods of memory which
have distinct anatomical correlates: Immediate memory functioning over
a period of seconds: recent memory applicable over a scale of minutes to
days: and remote memory ranging over time periods spanning months to
years.
Immediate memory can be understood as the ability to follow a train of
thought. It is divided into phonological and visuospatial components. The
phonological component is localised in the left hemishphere and the
visuospatial in the right.. Immediate memory is often related with recent
memory using the concept of working memory. Working memory is defined
as the ability to store information for several seconds while other cognitive
operations take place using this information. The dorsolateral prefrontal
cortex is required for working memory along with the certainty with which
the information is known. [2] Some researchers locaUse working memory
predominantly to the left frontal cortex.
Three brain structures are critical to the formation of memories: the medial
temporal lobe, certain diencephalic nuclei, and the basal forebrain.
The hippocompus is part of the medial temporat tobe. Adjacent to the ante
rior end of the hippocampus is the amygdata. The amygdala and the hip
pocampus work in tandem to store emotional experiences. The amygdala
rates the emotional importance of an experience and activates the level of
hippocampal activity. This phenomenon is called the memory enhance
ment effect and is the reason why emotionally intense experiences are
etched in memory. This is why most of us would find it hard to recall what
we had for lunch last Tuesday, but remember in great detail what the menu
for a close family wedding three years ago was or the exact sequence of
events when vie were in a car accident.
The amygdata also plays a role in the formation of long-term memory by
moduLating synaptic plasticity, which helps to retain a memory. It helps to
visuaLise memory as a grassy path, that when used repeatedly becomes a
place of common fare.
Long-term memory for learning events is not formed immediately. These
memories are slowly made over time, through a process called tong term
potentiation These are enhanced and made permanent when they are
potentiated by experiences. This is also why you don’t remember last
minute cramming after a few weeks. It is, therefore, imperative for a medi
cal student to ensure that all forms of knowledge are enriched by seeing a
patient or dealing with a relevant clinical experience in real Life settings of a
hospital. The lesser the gap between studying and clinical experience, the
higher the chance that the knowledge will remain in memory for the long
term.
The association areas are required for the formation of memory for motor
acts. The performance of a new action requires feedback from the sensory
cortex and association areas. Neuroimaging has shown activation of the
large parts of the cortex, during performance of unskilled acts. When per
forming repeated activities initially the medial temporal lobe is activated,
however with time the performance of the act results only in the activation
of the premotor and left parietal cortex. This phenomenon is known as the](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-121-320.jpg)

![There have been attempts to explain different temperaments in humans by
examining variations in a person’s brain stem, Umbic system, and thatamo
cortical arousal system using Electroencephalogram (EEG). [1] Limbic sys
tem activation has been [inked to neuroticism, with high activation showing
high neuroticism.[2] High cortical arousal has been shown to be associated
with introversion. People with high extraversion and low neuroticism have
been shown to have the towest overa[[ levels of internal arousat. Converse
ly people with high extraversion and high neuroticism have been shown to
have the lowest intrinsic thatamocortical excitation.
References
1. Robinson, David (6 November 2000). UH0w brain arousal systems de
termine different temperament types and the major dimensions of per
sonality.” Elsevier. Personality and Individual Differences i: 1233—1259.doi:
10.1016/s0191-8869(oo)0o2;1-7.
2. Robinson, David; Gabriet, Katchan (22 February 1993). Personality and
Second Language Learning(PDF). Personality Individual Differences i6 (1):
143—157.dOi:10,1016/0191-8869(94)90118-x. Retrievedl2 November 2012.
Steep
Steep is a recurring state of altered consciousness, imperative to nor
mal brain and body function. Approximately one third of our lives is spent
asleep. Steep is characterised by decreased awareness and interaction
with surroundings, lowered sensory activity and inhibition of voluntary
muscles.
The awake state is characterised by beta and alpha waves on the electro
encephalogram. Beta waves are commonly seen during active mental con-
centration whereas alpha waves are seen when a person c[oses their eyes
and relaxes.
Each stage of the sleep cycle is characterised by a specific wave form on
EEG. Mapping the transition of sleep from one stage to another is known as
sleep architecture and this changes with age.
The normat sleep cycle is divided into rapid eye movement (REM) steep
and non-rapid eye movement (NREM steep). REM sleep is a period of high
levels of activity in the brain and a level of physiological activity similar to
when the person is awake. During NREM sleep, physiological activity is less
than when an individual is awake. NREM has four stages (1-4).](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-123-320.jpg)

















![In our culture, most psychiatric disorders, epilepsy, fits and related chang
es in consciousness, and headache are attributed to supernatural causes
or ‘evil eye’. Heart conditions, diabetes, and hypertension are attributed
to stress, poor dietary habits, and unhealthy lifestyles. Liver and kidney
disease are attributed to eating the ‘wrong food’ ( “garam taseer”). Sexual
diseases are considered a curse of nature, caused by moral depravity.
Cultural views on treatments and interventions are largely diverse and vary
with social class, educational background. urban and rural setting and in-
fluence of prevailing subcultures. Altopathic medication are Largely viewed
as ‘goram’ and dangerous. and essentially lesser of the two evils when
confronted with disease. Pharmacological preparations are called ‘ongrezi
dawayi’ (a reference to the days of the British Pa]). This is to distinguish
it from ‘des! dawa’ (local or medicine of our own heritage). ‘Des! dawn’ is
considered ‘thand/’ and thus, more appropriate in a predominantly hot and
humid temperate setting. Local translations of the words ‘tablet’, ‘injection’
have dangerous connotations e.g. ‘tablet’ is translated as ‘got/which is the
same as ‘bullet’, injections are often just referred to as “su/”fneedle).
The most preferred and the first line of treatment in our culture are house
hold remedies and herbs based on past experience and conventional
wisdom. These are supplemented by prayers to The Almighty by the
individuaL his family, and sometimes the pit, the local faith healer, or the
prayer leader at the local mosque. Alms, sadqo, taweez, and holy water are
also used. It is only after the failure of these convenient, easily accessible,
inexpensive and trustworthy interventions that professional treatments and
interventions are considered an option. Alternative medicine, folk medicine,
healing through spiritualists, omits, sorcerers, shamans, and faith healers
are often reserved for patients with psychiatric disorders and epilepsy.
Often inhumane methods of ‘treatment’ are used by these agents in the
presence of and in connivance with the referring members of the family.
Cuftura[ty Sensitive Clinical Assessment
A culturally sensitive assessment may not he required in all patients and
not always at the start of a treatment plan. It would, however, be urgently
required when a patient is obviously from a different ethnic background
e.g. a patient from rural Sindh, central-Punjab, Balochistan or Northern
Areas being nursed in Lahore, Karachi or Islamabad. It is also important to
consider the concept of heritage consistency. This refers to how closely
an individual is influenced by or practices his/her particular ethnic back
ground. The lifestyle, health belief model, or practices of an individual may
not always be the same as their cultural heritage, In case a patient has a
high heritage consistency, the next step is to note how much of his/her
beliefs are influenced by the cultural background.
The following questions can be asked in a clinicat setting to ensure a
deeper cultural understanding of the patient’s explanatory model of illness
• What do you call your problem? What name does it have?
• What do you think has caused your problem?
• How do you think it started and what course do you think it will take?
A recommended approach for culturally sensitive health professional was
suggested by Fowkes and Berlin in lg8os. This approach can yield not only
invaluable information about the patient and family’s cultural understand
ing of the disease (their health belief model HBM) but also improves](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-143-320.jpg)
































![Chapter 5
Psychosocial Aspects of Alternative Medicine
The term alternative medicine refers to atl medicine that has not been
tested using the scientific method, and has no evidence to prove its efficacy.
This includes homeopathy, acupuncture. hikmat and other forms of herb
al medicine. In our culture, alternative medicine is usually the first line of
treatment that a patient adopts when s/he first becomes ilL It is practiced
by anyone and everyone who has ever experienced illness, and alternative
medical advice can be sought from anyone, whether it is a fruit vendor, a
neighbour or your grandmother. The reasons for this are that traditionalLy
a[Lopathic medicine was considered a western invention, harsh’ on the
body and unsuitable for the subcontinentat climate. It was only to be turned
to if and when all else had failed, and the healing properUes of household
remedies had failed. A return to the use of alternative medicine is seen in
patients in situations where allopathic medicine suggests a painful cure, or
does not have one.
White anecdotal evidence states that these alternative methods are ef
fective there is no scientific evidence to back this claim. Homeopathy, in
particutar, according to the NHS UK has been cited as ‘performing no better
than placebos.” The National Institute of Health and Care Excellence (NICE)
guidelines do not recommend the use of homeopathy for the treatment of
any ailment. In a 2013 large scale study conducted by the Nationat Health
and Medical Research Council of Australia, 57 systematic reviews containing
176 individual studies, published between 1997 and 2013 were evaluated by
an independent contractor overseen by a body of homeopaths. The study
found that there is no evidence that homeopathy caused greater health im
provements than placebo. or caused health improvements equal to those
of another treatment. This finding has been repeatedly confirmed by find
ings in various peer reviewed journals. tl][21[3][41
As health professionals it is therefore, unethical to recommend homeo
pathic treatment to any of our patients, even if we have personally feel that
they are effective. Any patients who report that they are using homeopathic
medication must be informed that there is no evidence to support their effi
cacy. They must also be instructed to continue the use of altopathic medi
cine if they insist on using homeopathic or other remedies.
References
1. Fisher, P., & Ernst, E. (2015). Should doctors recommend homeopathy?.
www.bmj.com
2. Australian National Health and Medicat Research CounciL Statement on
homeopathy. 2015.
www.nhmrc.gov.au/_ffles_nhmrc/pubtications/attachments/camo2_nhm-
rc_statement_homeopathy.pdf.
3. Ernst E. A systematic review of systematic reviews of homeopathy. British
journal of clinical
pharmacology. 2002 Dec 1;54(6):577-82.
4. Campbell A. Homeopathy in perspective. Lulu, 2008.
5. Cucherat M, Haugh MC, Gooch M, BoisselJP. Evidence of clinical effica
cy of homeopathy. European Journal of Clinical Pharmacology. 2000 Apr
1:56t1):27-33.
6. Smith K. Against homeopathy—a utilitarian perspective. Bioethics. 2012
Oct 1;26(8):398-409.](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-179-320.jpg)
![Chapter 6
Common Psychiatric Disorders in General
Health Settings
The workings of the human mind have remained mysterious since the
beginning of time. Psychiatry. the medical specialty devoted to the study.
diagnosis, treatment, and prevention of mental illness, is just as Little
understood, despite being the oldest profession known to man. In prehis
toric times, people haunted by ‘evil spirits” were taken to medicine men
to have holes drilled into their skutts to let the spirits escape. The need to
understand the way our minds work coupled with lack of scientific prowess
to investigate the mechanics of the brain led to the perpetuation of these
myths. The first psychiatric facilities were set up in the 8th century in the
Islamic world but methods more humane than exorcisms did not come into
use until the seventeenth and eighteenth centuries. Psychiatry has come
a long way since then but sadly the perceptions surrounding it are very
much prehistoric, especially in our part of the world.
The myths and misconceptions surrounding mental illness, treatments and
mental health professionals themselves are many and manifest. The war
against the stigma of mental illness is one that we alt fight. whether we are
protesting against being called “crazy” or fighting for a loved one to get
help. According to the WHO Mental Health Action Plan 2013-2020 Re
port, “mental, neurological and substance use disorders exact a high toll,
accounting for 13% of the total global burden of disease in the year 2004,
Depression atone accounts for 4.3% of the global burden of disease and is
among the largest single causes of disability worldwide Eli % of all years
lived with disabitity globally], particularty for women. The economic conse
quences of these health losses are equally large: a recent study estimated
that the cumutative global impact of mental disorders in terms of lost eco
nomic output will amount to US$ 16.3 million between 2011 and 2030.”
Some of the most common myths and misconceptions surrounding mentaL
health issues, their treatments and mentat health professionals are being
dealt with here hi:
Myth: Psychiatric Illnesses do not exist or are caused by magic and evit
spirits
Reatity: Psychiatric illnesses are caused by structural and chemical chang
es in various structures of the body, especially the brain, and are just as
much a “curse” as any other illness or adverse life event. The reasons for
this are genetic, biochemical, behavioural and environmentaL According
to a WHO Report, one in every four people in the world wilt be affected by
mental or neurological disorders at some point in their lives. Psychiatric
Illnesses constitute 15% of all diseases incurred in people throughout the
world. 33% of all hospital attendances are for psychiatric diseases.
Myth: Psychological factors do not cause any other diseases
Reality: Psychological factors are acause of the disease for at least 60% of
alt patients with any disease. In fact, mental illnesses such as depression
may predispose one to developing infections, heart disease, diabetes and
even cancer.
•xed!n
istHyaKhan](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-180-320.jpg)












![f Suicide and Detiberate Self harm (DSH)
All patients of depression must be screened for suicide risk as go% of those
committing suicide or deliberate self harm are suffering from a psychiatric
illness. It is one of the top 10 causes of death in all age groups and one of
the top 3 causes in young adults and teenagers. Certain risk factors are
particutarty associated with completed suicide including:
• Gender (elderly white males being at highest risk),
• Psychosis,
• Alcoholism,
• Chronic physical illness, lack of social support and use of generally
lethal methods in the past (e.g. Gun rather than overdose of
medication). (For more, see box)
Medical students and young doctors may be reluctant to explore suicid
al ideation in the mistaken belief that asking about suicide may actually
increase a patient’s risk or give them ideas of suicide.” In fact, the opposite
may be true. Assessment of suicidal tendencies usually reassures patients,
reduces anxiety for both patient and doctor and facilitates partnership
in suicide prevention. The assessment should begin gradually by asking
questions such as Sometimes when people who are going through the
circumstances that you are, they may start to feel like life is not worth tiv
ingr and then asking more specifically about a history of suicidal attempts.
any specific current plans, hopelessness and any specific current inten
tions.
Deliberate self-harm is a term used to describe an act in which an individ
ual deliberately causes injury or harm to themselves, without the intent to
commit suicide. This may be in the form of cutting, or ingesting substances
in non-lethal doses.
Where doctors globally have a lower mortality rate from cancer and heart
disease relative to the general population, they sadly have a significantly
higher risk of dying from suicide [3]. In fact, according to a survey in 2015,
doctors are the most professionals to commit suicide, followed closely by
dentists. The leading cause of this is the prevalence of depression in med
ical students and postgraduate trainees. Completed suicide is also more
prevalent amongst medical professionals partialLy because of availability
and access to lethal means. Medical students and trainees are at particular
risk because they are unlikely to report a history of depression. Sadly. even
when it is reported, it may be neglected. This is due to myth that people
who ctaim to be having suicidal ideas are not likely to commit suicide. The
truth is 67% of individuals who committed suicide had confessed to some
one that they wanted to kill themselves. The famous Urdu saying o garajte
ham wo baraste nahi’ is untrue when it comes to a risk assessment of sui
cide. Any suicidal ideation being reported should, therefore, immediately
be considered as serious and requiring intervention. A detailed suicide risk
assessment must be carried out in all such cases. ‘The biggest risk of sui
cide is a direct statement of intent” [41 . These statements should never be
ignored, or responded to with statements of how the person is just looking
for attention” or ‘doesn’t reatly mean it.”](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-193-320.jpg)
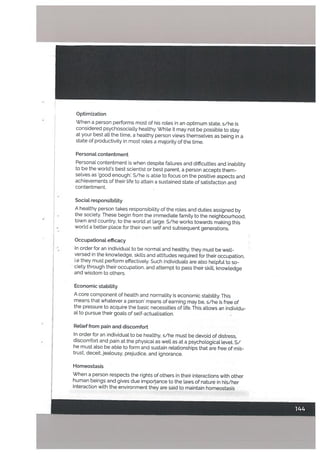
![Protective factors of suicide
Sane. ofconnectadneas
Having Chfl*.n
Good health
flestrictad Access to means
• U&. gender
• Early adufrage
• Psychological/emotional
problems
• P,dcal health problems
•Stranful I wants
• Major Depression
•4polerAfbctlveDbuitler
• Subetanc.abus. plenrd.r
• Antioclal Personality
Dlsord.r
• HLstoryofpsychlattlccare
• Previous 5ulcldai
b.hauiow
•Slngh
• Separated
• Family conflicts
• History oFchUdhood abuse
•Family history ofsuicide .
r
g. DeLirium
Delirium, also referred to as acute confusional state, refers to an acute de
dine in consciousness, cognition and attention. There is an incidence of up
to 55% in medicat and surgical inpatients 12].
Presenting Complaints
Families rather than the patient may request help because the patient is
often in a state of confusion or agitation. Delirium may commonly occur in
patients who are hospitalised for medical conditions, particularly in inten
sive care units and acute surgical units.
Diagnostic Features
Delirium is characterised by its sudden onset of hours or days. Confusion
is often present and patient struggles to understand surroundings. The
following neuropsychiatric symptoms are common:
Individualised Family Related Social Environmental
Risk Factors Risk Factors Risk Factors Risk Factors
• Socioeconomic .. Easy access to methods
disadvantage • cuturaisuppcttersuicisie
• Migrant population M.dio
UflernpbYrneflt Suicide among peers
•Soc
• Clouding of consciousness
• Poor memory,
• Agitation,
• Changi ng/ftuctuating emotions,
• Loss of orientation,](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-194-320.jpg)



![Masturbation
No other form ofsexual activity has been more frequently discussed, more
roundly condemned, and more universally practiced than masturbation.
- Kaplan and Saddock, Synopsis of Psychiatry
Masturbation refers to the physical stimulation of genitalia by oneself for
sexuat pteasure. This is a normal part of psychosexual devetopment. It is
an activity shrouded in shame and mystery despite the fact that nearly
all post-pubescent males and up to three fourths of females indutge in it
(Kinsey).
Children become aware of their genitaliajust as they become aware of
their other body parts. Upon reaching puberty. however, due to the in
crease in sex hormones and development of secondary sexual characteris
tics, masturbation may become a regular activity.
Myths and misconceptions such as “masturbation may result in loss of
sexual prowess and potency” and “masturbation can cause mental illness”
or “masturbation may result in a loss of manhood and mate virility” abound,
especially in our culture. There is no scientific evidence to support these
claims. Masturbation is a symptom of an emotional disturbance (not a
sexual one) only if it results in the individual losing control and
compulsively indulging in it ho].
SexuaL orientation
According to the American Psychological Association, sexual orientation
refers to the sex of those to whom one is sexuatly and romanticatl.y attract-
ed. For the majority of the population (according to census data worldwide)
sexuat orientation is heterosexual i.e. individuals are attracted to the oppo
site sex. Statistics suggest that about 1-5% of the population of the world
has different sexual orientations. This number may be understated, how
ever, given government and religious taws banning homosexuality in most
parts of the world. This may be homosexual, i.e attraction to the same sex,
bisexual, i.e attraction to both genders and asexual, i.e no sexual attrac
tion. Another subset of individuals exists, who feel that sexuality cannot
be labelled. These individuals refer to themselves as “queer” or pansexual
or polysexual. Some research indicates that for some individuals, sexual
orientation may be fluid. This may be especiatly true for women (e.g.. Dia
mond, 2007; Golden, 1987; Peptau & Garnets, 2000),
As of July 2015, 72 countries and five sub-nationaljurisdictions have laws
criminaUzing homosexuality. A majority of these countries, inctuding Paki
stan are in Asia and Africa.
According to Darwin, natural selection dictates that any variations that
occur have to be ‘useful to man’ i.e. they must aid in an organism’s struggle
for survival and procreation. Homosexuality defies laws of natural selection
by preventing procreation due to same-sex sexual behaviour. Despite this,
it remains a stable population level trait in humans and animals, resulting in
a so-catted Darwinian “paradox.” Evolutionary models propose that genes
influencing homosexuality have a reproductive benefit on heterosexual
carriers of the gene 121. This may be the reason that homosexuality
continues to persist.](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-200-320.jpg)
![In 2006, a study found that human sexual preference has a significant ge
netic component. [41. It was also seen that biological and congenital factors
regulate human sexuatity 13]. These findings were corroborated in a study
2015, in which a Large scate genome-wide scan resulted in findings that
support the existence of genes on chromosome 8 and Xq28 influencing the
development of mate sexual orientation. ti] . Another study found linkage
between male sexual orientation and markers on the X chromosome of the
mother in some famities. The study found that the X chromosome played
a role in regutating sexuat orientation in a subgroup of homosexual males
[41. Some studies indicate females with hyperadrenocorticalism are more
likely to be homosexual as welt as bisexual than the general population.
Research in this field has been, for the most part, inconclusive. This may he
due to the tack of definitive samples, the abstract concept of attraction or
the taboo associated with nonheterosexuality. Continued research efforts
are required to enhance understanding of the genetics factors affecting
human sexuality.
Psychiatric morbidity
Research shows that non-heterosexual individuals are more likely to suffer
from poor general health [71. They are also twice as Likely to suffer from
depression, panic disorder, generatised anxiety disorder and have a higher
risk of suicide [51181. This is especially true for younger adults [6]. They also
have significantly higher rates of alcohol dependency and drug abuse Ig].
One factor in this is of course, the societal pressures and religious taboo
associated with non-heterosexuality. Due to this taboo, such individuals
may often present to a health professional with medically unexplained
symptoms, and/or severe depression and anxiety.
Sexuat Disorders
According to the International Classification of Disease, Tenth Edition, sex
ual disorders encompass three categories: sexual dysfunction (not caused
by organic disorders), disorders of sexual preference (paraphilias) and
gender identity disorders (gender dysphoria).
These are of importance due to the higher number of psychiatric morbid
ities associated with them. These individuals are more likely to suffer from
anxiety, depression and somatoform disorders. They also have higher risks
of suicide and deliberate self-harm. Often the clinical presentation may he
that of persistent headache, backache, abdominal discomfort. and gener
alised aches and pains. Low mood and other depressive features,
especially guilt and severe anxiety may he present.
SexuaL Dysfunction
Sexual dysfunction occurs when there is inability, difficulty or pain involving
sexual intercourse. This includes disorders such as those described in the
table above, The presence of any sexual dysfunction is a difficult situation for
not just the individual but also the sexual partner. In cases where the dys
function is severe enough to not allow for consummation of the marriage or
lead to reproductive problems. the entire family may become involved. This
can be a source for great discomfort for the individual. This is especially true
for males as they are expected to be ‘more informed’ in the sexual act and
all its nuances), even if they have no prior experience. Also in males, sexual
prowess or lack thereof, is closely connected to their self-esteem.](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-201-320.jpg)


![References
1. Sanders AR, Martin ER, Beecham GW, Guo 5, Dawood K, Rieger G, Bad
nerJA, Gershon ES, Krishnappa RS, Kolundza AS, Duan]. Genome-wide
scan demonstrates significant linkage for male sexual orientation.
Psychotogicat medicine. 2015 May 1:45(07):1379-88.
2. Burn A, SpectorT, Rahman Q. Common genetic factors among sexual
orientation, gender nonconformity, and number of sex partners in female
twins: ImpLications for the evolution of homosexuality. The journal of sexual
medicine. 2015 Apr 1;12(4):1004-11.
3. Jannini EA, Burn A, Jern P. and Nove[ti G. Genetics of human sexual be
havior: Where we are, where we are going. Sex Med Rev 2015;3:65-77.
4, Bocktandt S, Horvath 5, Vilain E, Hamer DH. Extreme skewing of X chro
mosome inactivation in mothers of homosexual men. Human Genetics.
2006 Feb 1:118(6):691-4.
5. Prajapati AC, Parikh S, Bala DV. A study of mental heatth status of men
who have sex with men in Ahmedabad city. Indian journal of psychiatry.
2014 Apr:56(2161.
6. Bränström R, Pachankis JE. Hatzenbuehler ML. Sexual orientation differ-
ences in mentaL health morbidity: A population-based longitudinal study.
The European Journal of Public Health. 2015 Oct 1:25(suppl 3):ckVl74-062,
7. Fredriksen-Gotdsen KI, Emlet CA, Kim HJ, Muraco A, Erosheva EA, Gold-
sen J, Hoy-Ellis CP. The physical and mental health of lesbian, gay male,
and bisexuat (LGB) o[der adults: The rote of key health indicators and risk
and protective factors. The Gerontologist. 2013 Aug 1:53(4):664-75.
8. Cochran SD, Sullivan JG, Mays VM. Prevalence of mental disorders,
psychological distress, and mental health services use among lesbian, gay,
and bisexual adults in the United States. Journal of consulting and clinical
psychology. 2003 Feb;71t1):53.
9. Cochran SD, Mays VM. Relation between psychiatric syndromes and
behavioraLly defined sexual orientation in a sample of the US, population.
American Journat of Epidemiology. 2000b;151:516-523. [PMC tree artictel
tPubMedl
io. Kaplan and Saddock Synopsis of Psychiatry, Eleventh Edition, page 570.
V](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-205-320.jpg)










![trauma “esults from anything that disrupts a chitds sense of safety and
security. This can include an unsafe environment, separation from a parent
or a sei Quo iLlness. Developmental trauma is most severe when it involves
betraya or harm at the hands of a cai’egiver. This trauma has a negative
impact on a childs physical, emotional and social development. Children
who have been traumatised see the world as a dangerous and frightening
place. When childhood trauma is i ot resolved, this sense of fear and help
tessness can carry over into adulthood, setting the stage for further trauma.
Normal responses to traumatic events
It is important to distinguish between normal reactions to traumatic events
and symptoms of a more serious and persistent problem Following a
traumatic event, most people experience a variety of emotions, including
shock, fear, anger and reLief to be alive. Often they think or talk of nothing
else except what they went through. Many others feei]umpy, detached or
depressed. Such reactions are neither a sign of weakness nor a positive
indicator of lasting trouble. They represent a normal response to an
abnormal event.
These feelings and symptoms typically last from a few days to a few
months gradually fading as one processes the trauma. Recovering from
trauma takes time and everyone heats at his or her own pace. However if
despite passage of months, the symptoms show no sign of letting up, a
person may be experiencing emotional or psychological trauma.
Professionat help is required if a person has:
Problems at home or work
• Living with persistent fear and anxiety
• Haunted by overwhelming memories or emotions
• Avoiding more and more things that reminds one of trauma
Posttraumatic Stress Disorder
Posttraumatic Stress Disorder tPTSD) is a condition that results from the
most severe kind of trauma. It is characterised by intrusive memories.
flashbacks or nightmares, avoiding things that remind one of the traumatic
event and living in a constant state of red alert, also known as
hyperarousal.
Common reactions to trauma
Guilt and wff-blarne
Mood swings nd lrtftablIftr
Dlstr.sslng memories
Social withdrawal
Feeling sad](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-217-320.jpg)







![Chapter]3
Stress and its Management
Definition
Hans Setye introduced the concept of stress into physiology from phys
ics, where it generally refers to a force acting against some resistance.
He defined stress as “the rate of wear and tear in the body” and “the state
manifested by a specific syndrome which consists of all the non-specifical
ly induced changes within a biological system.” In this General adaptation
syndrome (GAS), glucocotticoids are secreted by the adrenal cortex in re
sponse to adaptation demands placed on the organism by such disparate
stressors as heat, cold, starvation, and other environmental insult. Any such
stimulus to the body results in certain physiological changes in the body
which are cumulatively termed as stress (Lazarus; 1984). Stressors are the
environmental sources of threat to an organism, while stress is what occurs
as a result of this. Richard Lazarus emphasised the potential threat of life
events in causing stress.
Individuals have a personal view of their stress, based on their perception
of the event, past experiences, strengths. biographical assets and social
support. Other factors which influence the outcome of stress upon an
individual include race, gender. age, marital status, socioeconomic sta
tus and early developmental experiences. For example, black people are
more prone to develop hypertension than Caucasians. Females tend to
live tonger and recover quicker from illness than males. They also show
less physiological reactivity to stress as compared to males. The elderly
are more vulnerable to all kinds of stressors. The general observation that
work capacity decreases by 1% every year after 21 years of age, provides
evidence that people.who continue to work with same routines beyond 50
years tend to have higher incidence of coronary heart disease. Marriage
is considered a protective factor against stress and most illnesses in both
genders. Educational and economic attainments provide more resilience
against stress. Early parental loss, quality of love and care received in early
life years and children’s early exposure to socializations shape the re
sponse of people to different types of stress.
Stress is conventionally divided into two types based on the causative
factors:
Physiological stress caused by temperature. noise, hunger, disease, smok
ing, drinking and similar habits are considered generalised life stressors
affecting most people.
Psychosocial stress caused by psychological factors such as low self-es
teem, social factors such as life events (see table), job stability, career satis
faction, economic viability. marriage, children, relationships etc.
Stressors bring about a physiological change in the body of a person.
Some stressors produce impacts in a short span of time; such as loss of
parents orjob. Others, such as distressed relationships or care of a
disabled person in the house, inftuence the person gradually over a period
of time. Individual and situational variables mediate the relationship
between life change and illness.](https://image.slidesharecdn.com/behavioral-sciences-dr-mowadatrana1-240518055311-07f33cb4/85/Behavioral-sciences-dr-mowadat-rana-1-pdf-225-320.jpg)