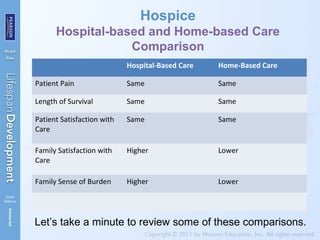
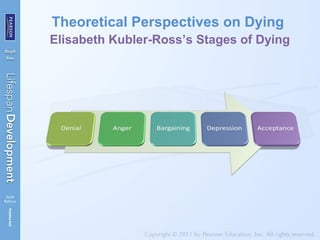
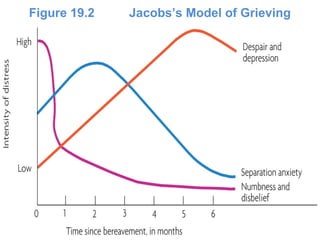
This chapter discusses death, dying, and bereavement. It covers where death typically occurs, an overview of hospice care philosophy and types, comparisons of hospital and home-based hospice care, developmental understanding of death, theoretical perspectives on dying and grieving, factors that influence the grieving process, and preventing long-term problems from grief. Key aspects of hospice care are that it views death as normal and involves families in patient care with the goal of palliative rather than curative medical care. Theoretical models of grieving suggest it occurs in stages or involves alternating between loss-oriented and restoration-oriented processes.