The document discusses the significant challenge of diagnosing and treating communicable diseases in developing countries, highlighting the need for standard laboratory procedures and quality assurance in microbiology. It introduces the 2nd edition of a manual on basic laboratory procedures in clinical bacteriology, detailing updated content and the importance of quality control in laboratory investigations. The World Health Organization's role in providing guidance and promoting best practices in laboratory techniques is emphasized to enhance public health outcomes.


![WHO Library Cataloguing-in-Publication Data
Basic laboratory procedures in clinical bacteriology / J. Vandepitte . . . [et al.].—2nd ed.
1.Bacteriological techniques—standards 2.Laboratory techniques and procedures standards
3.Manuals I.Vandepitte, J.
ISBN 92 4 154545 3 (NLM classification: QY 100)
© World Health Organization 2003
All rights reserved. Publications of the World Health Organization can be obtained from Marketing
and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel:
+41 22 791 2476; fax: +41 22 791 4857; email: bookorders@who.int). Requests for permission to
reproduce or translate WHO publications–whether for sale or for noncommercial distribution–should
be addressed to Publications, at the above address (fax: +41 22 791 4806; email:
permissions@who.int).
The designations employed and the presentation of the material in this publication do not imply the
expression of any opinion whatsoever on the part of the World Health Organization concerning the
legal status of any country, territory, city or area or of its authorities, or concerning the delimitation
of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which
there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they
are endorsed or recommended by the World Health Organization in preference to others of a similar
nature that are not mentioned. Errors and omissions excepted, the names of proprietary products
are distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication
is complete and correct and shall not be liable for any damages incurred as a result of its use.
The named authors alone are responsible for the views expressed in this publication.
Typeset in Hong Kong
Printed in Singapore
2001/13712—SNPBest-set/SNPSprint—6000](https://image.slidesharecdn.com/basiclaboratoryproceduresinclinicalbacteriology-191205114409/85/Basic-laboratory-procedures-in-clinical-bacteriology-6-320.jpg)

























































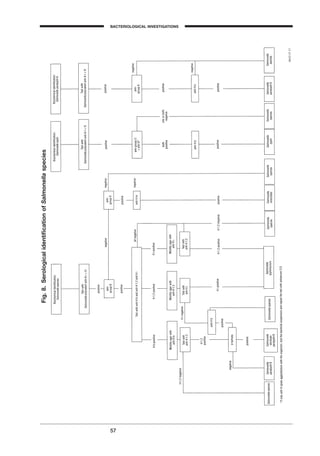
![1 corresponds to the typical salmonellae and includes among others: Salmo-
nella typhi, S. paratyphi A, S. enteritidis, S. typhimurium, S. choleraesuis. This sub-
group contains more than 2000 serotypes, which can be differentiated by their
antigenic formula (O, H and Vi antigens). Serotypes in subgroup 1 continue
to be named as if they were real species: Salmonella subgroup 1 serotype
typhimurium is simply called S. typhimurium. More than 99% of human sal-
monella isolates belong to subgroup 1.
The important antigens for serotyping Salmonella species are the somatic, or
O, antigens and the flagellar, or H, antigens. O antigens are present in both
motile and nonmotile organisms and are resistant to boiling; H antigens are
present only in motile organisms and are sensitive to boiling. The majority of
the Salmonella species are diphasic in the motile state and may exhibit two
antigenic forms referred to as phases 1 and 2. These phases share the same O
antigens but possess different H antigens. To identify the serotype it is neces-
sary to identify the specific H antigens in both phases. These may not always
be evident, and phase suppression may be necessary to confirm the latent
phase.
O antigens are designated by Arabic numerals. Phase 1 H antigens are desig-
nated by small Roman letters and phase 2 H antigens by Arabic numerals. For
example, the antigenic formula for S. typhimurium is 1,4,[5],12:i:1,2, where O
antigens are 1, 4, 5 and 12; phase 1 of the H antigen is “i” and phase 2 anti-
gens are 1 and 2. A bracket indicates that the antigen may be absent, and an
underlined antigen indicates that the antigen is associated with lysogenic con-
version by a bacteriophage. This change in antigenic structure is only present
when the bacteriophage is present and may be the only difference between
certain serotypes.
The Salmonella species have been placed in groups according to the presence
of certain O antigens. These groups are often referred to as the Kauff-
mann–White scheme. Capital Roman letters designate the O group. In the
original scheme the groups were A, B, C, D and E; these were subsequently
expanded to A–Z with 4 subgroups in C, 3 in D, 4 in E and 2 in G. The O
groups are defined by the presence of certain O antigens as follows:
55
BACTERIOLOGICAL INVESTIGATIONS
A
Table 18. Biochemical indentification of Campylobacter species found in stool
Growth at H2S/KIA Hippurate Nitrate Susceptible to
15∞C 25∞C 42∞C
hydrolysisa
reduction Nalidixic acidb
Cefalotinc
Campylobacter jejuni - - + - + + S R
subsp. jejuni
C. jejuni subsp. doylei - - - - d - S S
C. coli - - + + - + S R
C. lari - - + - - + R R
C. upsaliensis - - + - - + S S
C. fetus subsp. fetus - + - - - + R S
C. hyointestinalis - + v + - + R S
Arcobacter butzlerid
+ + - - - + v R
Abbreviations: +: >95% positive; d+: 75–95% positive; d: 26–74% positive; d-: 5–25% positive; -: <5% positive; v: variable result; S: susceptible; R:
resistant. H2S/KIA: Kligler’s iron agar.
a
Only deep purple colour is considered positive.
b
30 mg nalidixic acid disk.
c
30 mg cefalotin disk.
d
Catalase-negative or catalase weakly positive; Kligler’s iron agar.
BLM1 1/17/04 2:01 PM Page 55](https://image.slidesharecdn.com/basiclaboratoryproceduresinclinicalbacteriology-191205114409/85/Basic-laboratory-procedures-in-clinical-bacteriology-65-320.jpg)



























![Use the low-power objective (¥10) to bring the specimen into focus. Centre the
light in the field by adjusting the centring screws located on the condenser, and
focus the condenser by raising or lowering it until the smallest diameter of light
is obtained. Recentre the light if necessary. Then use the dry ¥40 objective to
bring the specimen into focus, and examine the slide carefully. The contrast will
be better when the microscopy is done in the dark. Avoid bright daylight.
T. pallidum appears white, illuminated on a dark background (Fig. 9). It is iden-
tified by its typical morphology, size, and movement. It is a thin (0.25–0.3mm)
organism, 6–16mm long, with 8–14 regular, tightly wound deep spirals. It
exhibits quick and rather abrupt movements. It rotates relatively slowly about
the longitudinal axis (like a corkscrew). This rotation is accompanied by
bending (twisting) in the middle and is executed rather stiffly. Lengthening
and shortening (like an elastic expander spiral) may be observed. Distortion
may occur in tortuous convolutions. When the organism is attached to, or
obstructed by, heavier objects, the resulting vigorous struggling distorts the
coils. Other non-syphilis spirochaetes may be loosely coiled, thick, and coarse;
the movements are different (not like a corkscrew), but take the form of a more
writhing motion, with marked flexion and frequent relaxation of the coils.
The demonstration of treponemes with morphology and motility characteris-
tic of T. pallidum constitutes a positive diagnosis for primary and secondary
syphilis. Patients with a primary chancre, which is dark-field positive, may
be serologically negative. They normally become serologically reactive within
a few weeks.
Failure to find the organism does not exclude a diagnosis of syphilis.
Negative results may mean that:
• An insufficient number of organisms was present (a single dark-field
examination has a sensitivity of no more than 50%).
• The patient had already taken antimicrobials.
84
Fig. 9. Appearance of T. pallidum under dark-field microscopy
[Negative]
SEXUALLY TRANSMITTED DISEASES
BLM1 1/17/04 2:02 PM Page 84](https://image.slidesharecdn.com/basiclaboratoryproceduresinclinicalbacteriology-191205114409/85/Basic-laboratory-procedures-in-clinical-bacteriology-94-320.jpg)























































































![WHO Library Cataloguing-in-Publication Data
Basic laboratory procedures in clinical bacteriology / J. Vandepitte . . . [et al.].—2nd ed.
1.Bacteriological techniques—standards 2.Laboratory techniques and procedures standards
3.Manuals I.Vandepitte, J.
ISBN 92 4 154545 3 (NLM classification: QY 100)
© World Health Organization 2003
All rights reserved. Publications of the World Health Organization can be obtained from Marketing
and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel:
+41 22 791 2476; fax: +41 22 791 4857; email: bookorders@who.int). Requests for permission to
reproduce or translate WHO publications–whether for sale or for noncommercial distribution–should
be addressed to Publications, at the above address (fax: +41 22 791 4806; email:
permissions@who.int).
The designations employed and the presentation of the material in this publication do not imply the
expression of any opinion whatsoever on the part of the World Health Organization concerning the
legal status of any country, territory, city or area or of its authorities, or concerning the delimitation
of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which
there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they
are endorsed or recommended by the World Health Organization in preference to others of a similar
nature that are not mentioned. Errors and omissions excepted, the names of proprietary products
are distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication
is complete and correct and shall not be liable for any damages incurred as a result of its use.
The named authors alone are responsible for the views expressed in this publication.
Typeset in Hong Kong
Printed in Singapore
2001/13712—SNPBest-set/SNPSprint—6000](https://image.slidesharecdn.com/basiclaboratoryproceduresinclinicalbacteriology-191205114409/85/Basic-laboratory-procedures-in-clinical-bacteriology-184-320.jpg)







































































