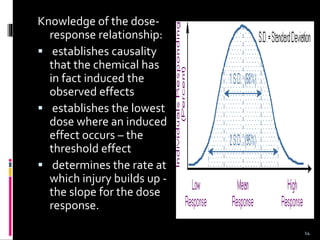
This document discusses basic concepts in toxicology. It defines toxicology as the study of adverse effects of chemicals on living organisms. Toxic effects can occur through various routes of exposure and be seen immediately or long after exposure. The dose and duration of exposure determine the severity of response. Target organs are also discussed, where specific tissues are affected rather than the whole body. Factors like intrinsic toxicity, dose, exposure conditions, and individual susceptibility influence the adverse health effects of toxins.






























![Biomagnification[1]](https://cdn.slidesharecdn.com/ss_thumbnails/biomagnification1-170608045729-thumbnail.jpg?width=640&height=640&fit=bounds)







































