Download to read offline



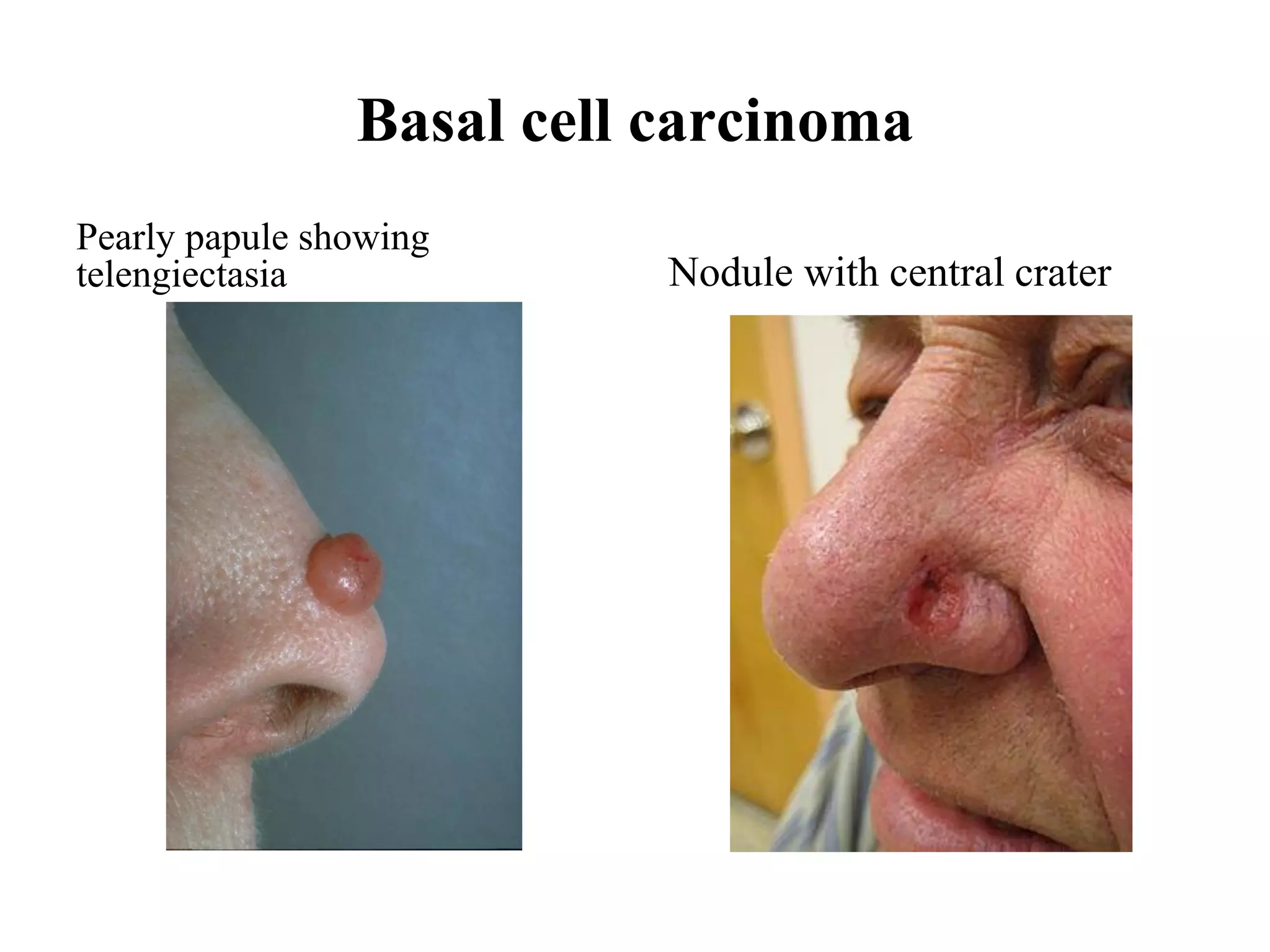

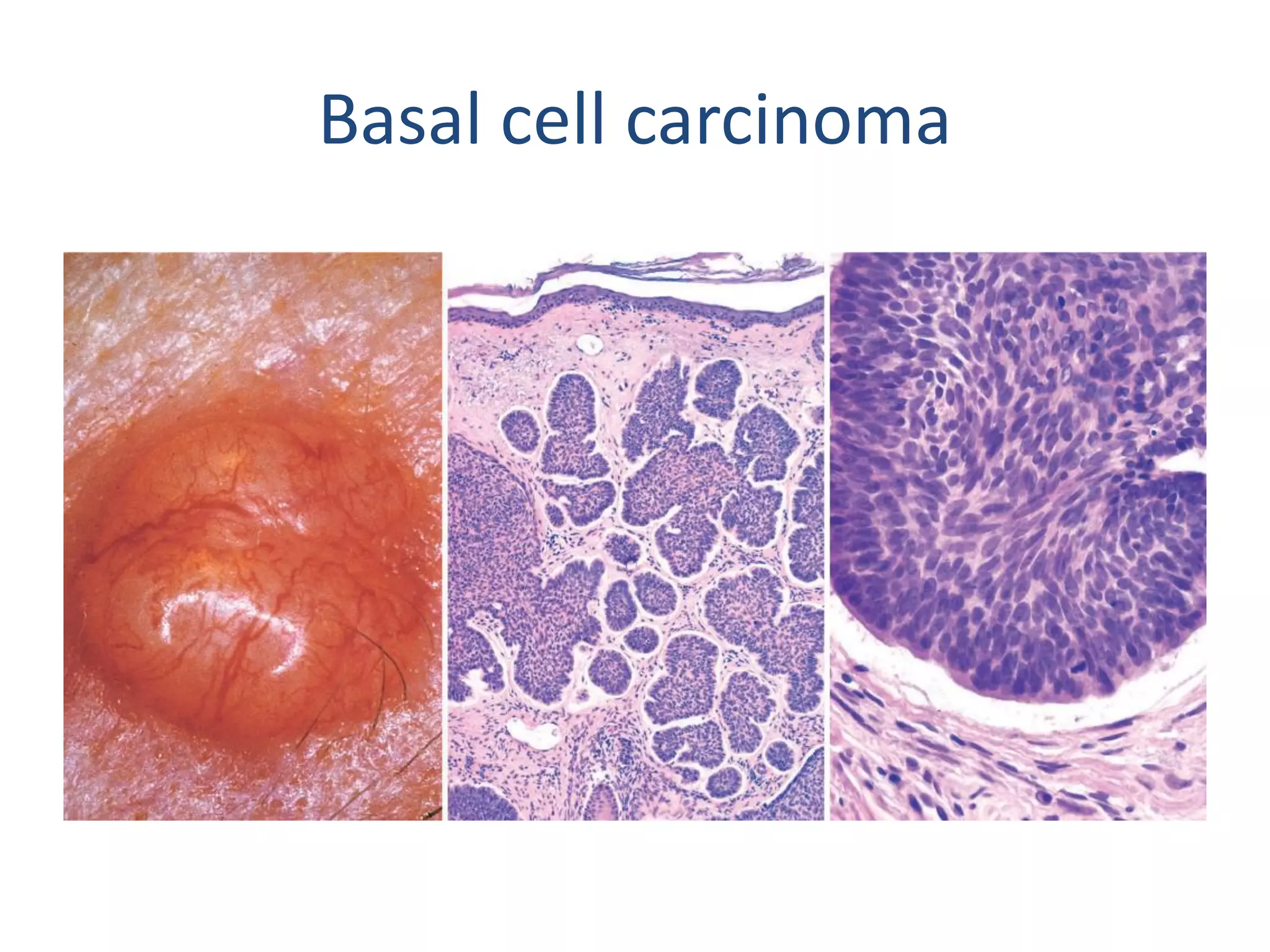


Basal cell carcinoma is a slow-growing type of skin cancer that rarely metastasizes but can be locally aggressive. It arises from the basal cell layer of the epidermis or hair follicles, resembling cells in the basal epidermal layer. Risk factors include chronic sun exposure, light pigmentation, genetic conditions like xeroderma pigmentosum, radiation exposure, and skin injuries. It is caused by mutations in the PTCH1 tumor suppressor gene, dysregulating the hedgehog signaling pathway. Basal cell carcinoma typically appears as pearly papules or nodules on sun-exposed skin, often with prominent blood vessels visible within the lesions.












































































