INTRODUCTION
BCC is slowprogressing NMSC that aises from basal cells ,most deeper layer of epidermis.
SYNONYMS- Rodent ulcer
Basiloma
non melanoma skin cancer (NMSC),
‐ to distinguish them from ‘melanomas’ which have a much higher
malignant potential.
BCC represent approximately 74% of NMSC whilst SCC are less common at 23%.
BCC is the most common skin cancer in immunocompetent individuals where as SCC is most common skin
cancer in immunosuppressed organ transplantation recipients.
3.
BASAL CELL CARCINOMA
EPIDEMIOLOGY
Increases as age advances-80% of cases occur in people aged 60yrs and over.
The life time risk of developing BCC is 28%-33%.
Male > female.
Risk is higher in individuals with markers of UV susceptibility.
Markers of chronic photodamage are positively associated with BCC.
ENVIRONMENTAL FACTORS
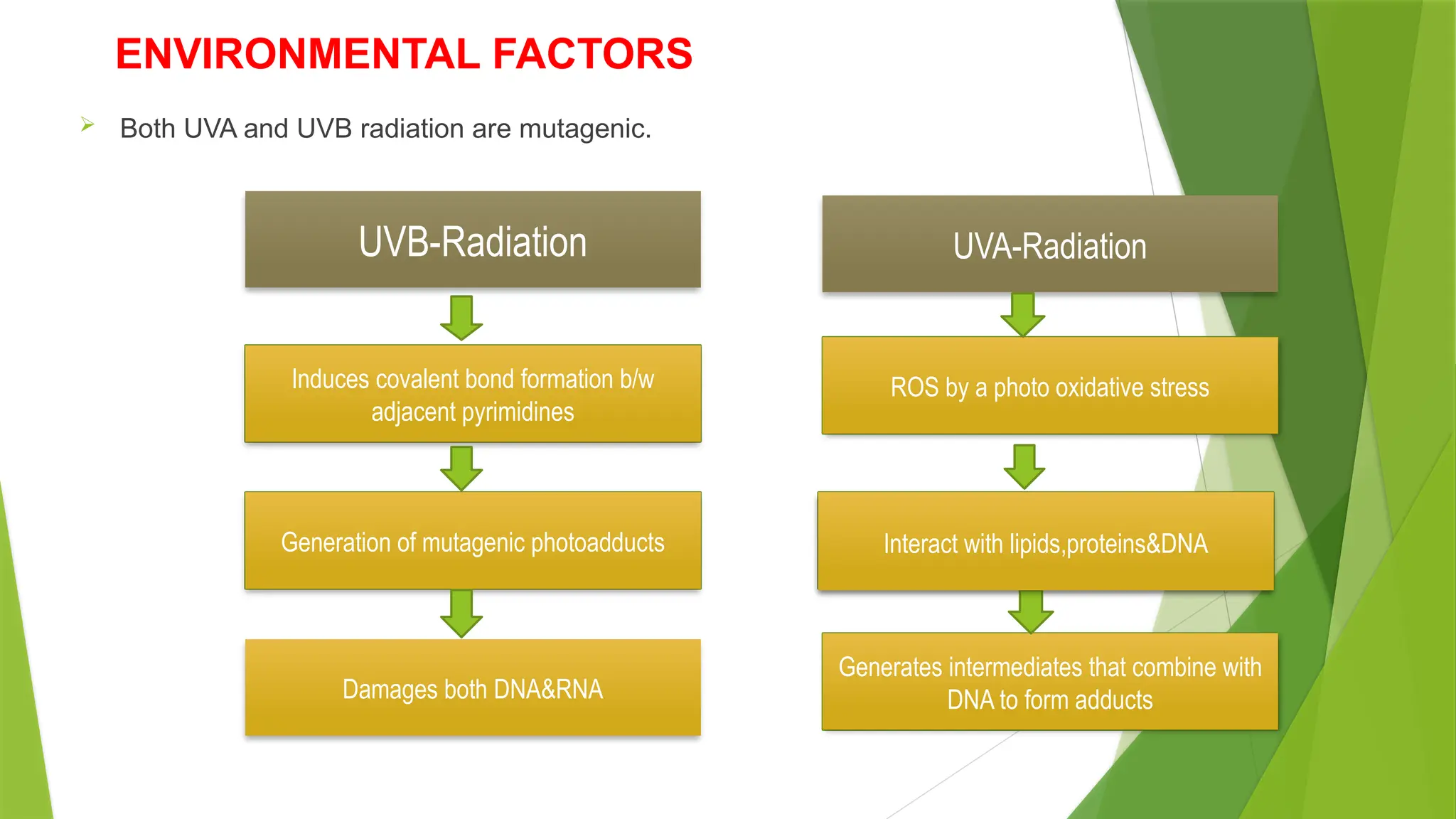
BothUVA and UVB radiation are mutagenic.
UVB-Radiation
Damages both DNA&RNA
UVA-Radiation
Generation of mutagenic photoadducts
Induces covalent bond formation b/w
adjacent pyrimidines
ROS by a photo oxidative stress
Interact with lipids,proteins&DNA
Generates intermediates that combine with
DNA to form adducts
Interact with lipids,proteins&DNA
6.
GENETICS
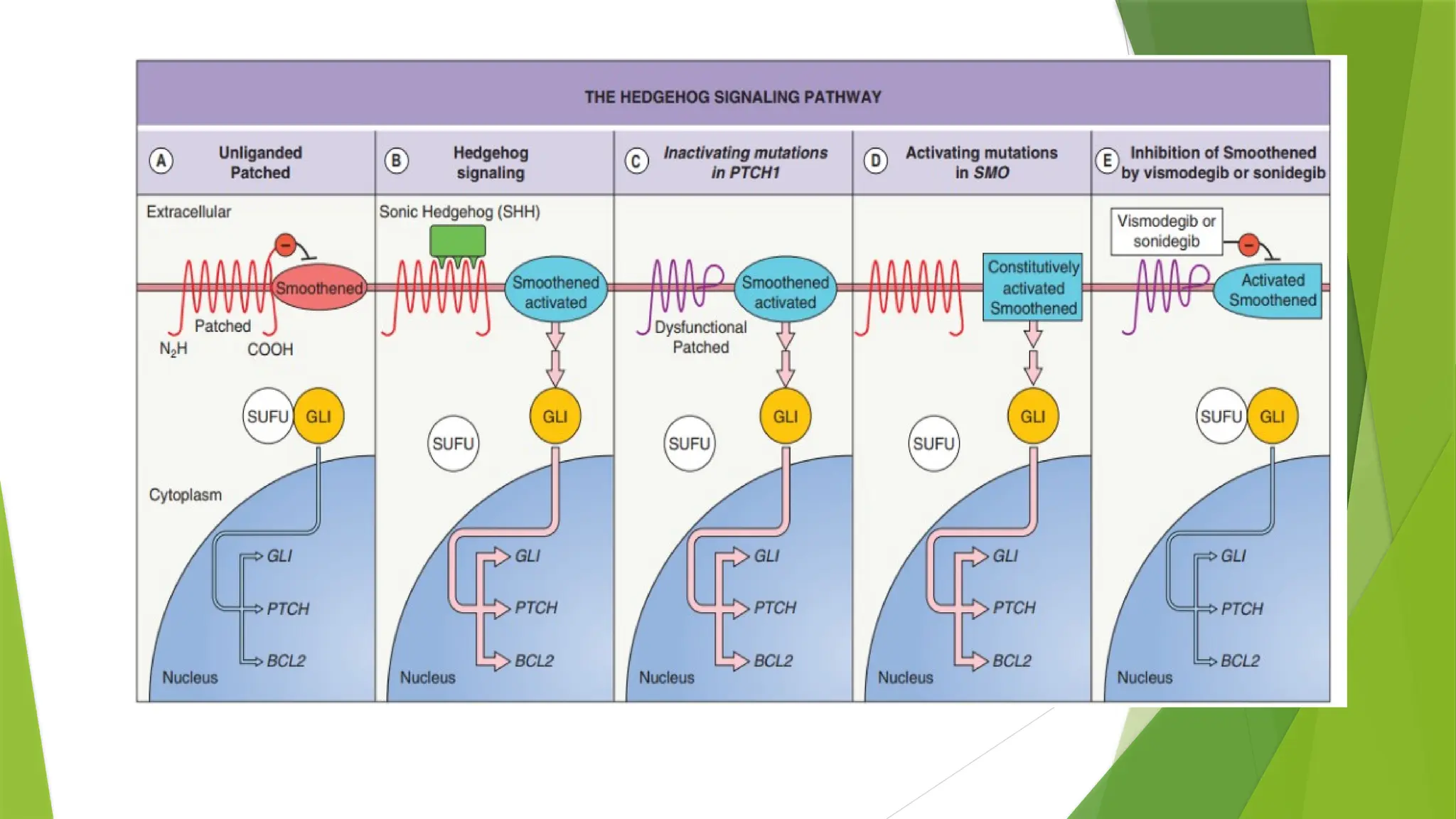
PTCH1 ,a segment polarity gene (9q22.3) with tumour suppressor functions encodes a
transmembrane protein, Patched 1 which acts like the receptor for SHH.
‐
Ptch 1 acts as a tumour suppressor, repressing the G protein coupled receptor smoothened (Smo).
‐ ‐
Loss of function mutations of PTCH1
‐ ‐
Reduced suppression of Smo
activation of the Gli family of transcription factors
resulting in sustained activation of target genes.
50% of BCCs – TP53 tumour suppressor gene mutations.
8.
SYNDROMES ASSOCIATED WITHBCC
A. XERODERMA PIGMENTOSA - Defect in DNA repair pathway,
Clinical Features- Photosensitivity, Freckles, Multiple skin cancer at
early age.
B. ALBINISM - AR disorder, defective melanogenesis, lightly or non
pigmented skin, silvery-white hair, reduced visual acuity, ocular
nystagmus predisposition to skin cancer.
. ROMBO SYNDROME: C/F- Atrophoderma Vermiculata, Milia,
Hypotrichosis, Trichoepithelioma,
BCC, And Peripheral Vasodilatation With Cyanosis.
9.
BASAL CELL NEVUSSYNDROME/ GORLIN SYNDROME
BCNS is an AD disorder due to an inactivating mutation in PTCH1 or rarely PTCH2.
Manifestations-
Multiple Or Early-onset Bccs
Odontogenic Keratocysts Of The Jaw
Palmoplantar Pits
Calcification Of The Falx Cerebri
Skeletal Anomalies .
Affected individuals may develop specific neoplasms such as medulloblastomas,
meningiomas , ovarian fibromas, and cardiac fibromas.
11.
BAZEX–DUPRÉ–CHRISTOL SYNDROME
Arare X linked dominant genodermatosis that predisposes affected individuals to multiple BCCs.
‐
Syndrome is characterized by hypotrichosis,
follicular atrophoderma of the cheeks,
milia cysts and
BCCs.
BCCs usually appear after the first decade of life.
Only females are affected.
12.
Occupational risk factors
Persons with outdoor occupations have a higher risk of developing skin cancer.
Agricultural workers, sailors, locomotive engineers, and textile workers.
Chemical exposures
Occupational chemical exposures which can lead to skin cancer most commonly involve
pesticides, coal tar, and polycyclic aromatic hydrocarbons.
BCC has been reported following extensive arsenic exposure. The typical latency period
from exposure to tumor development is 20–40 years.
13.
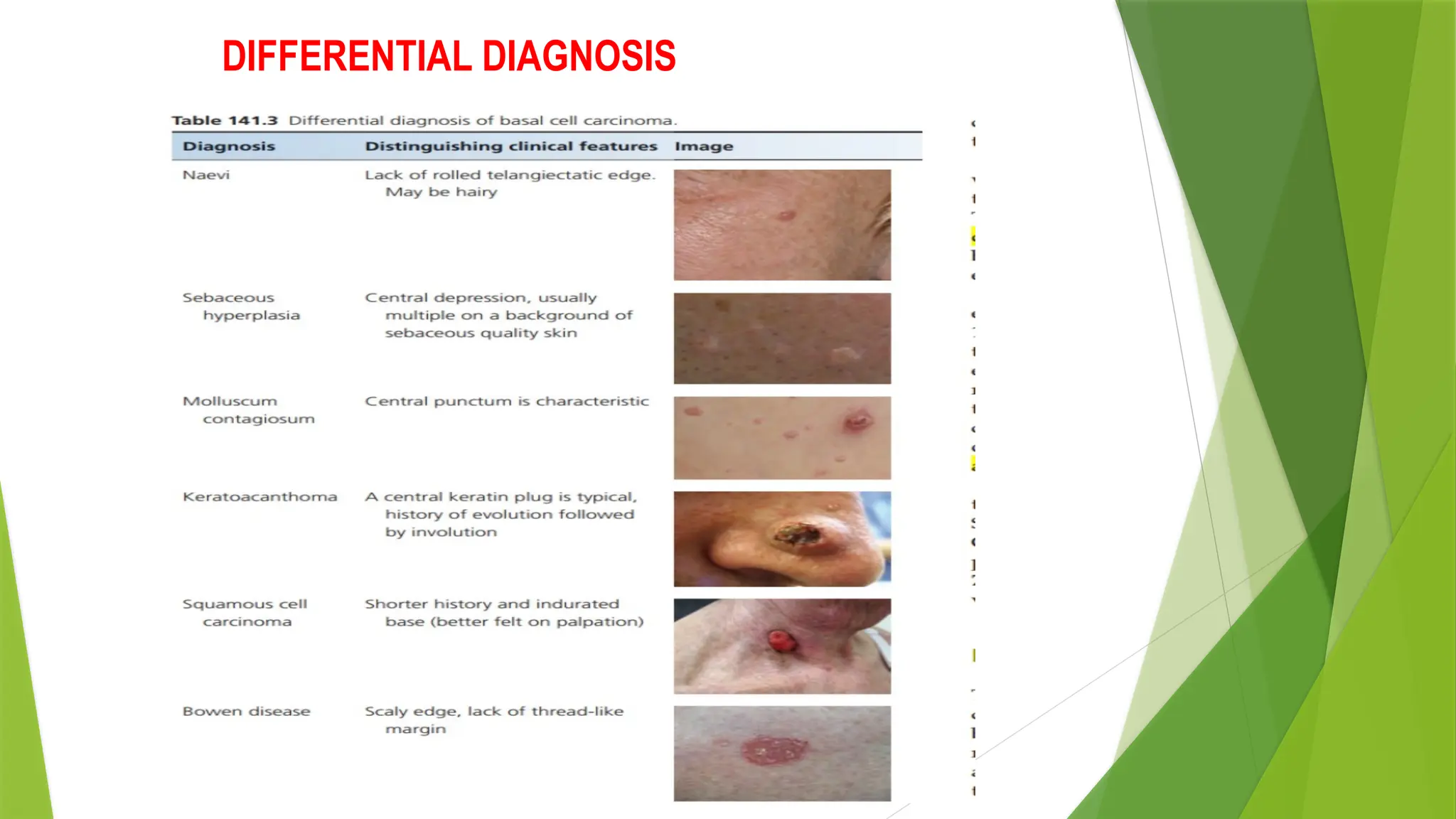
CLINICAL FEATURES
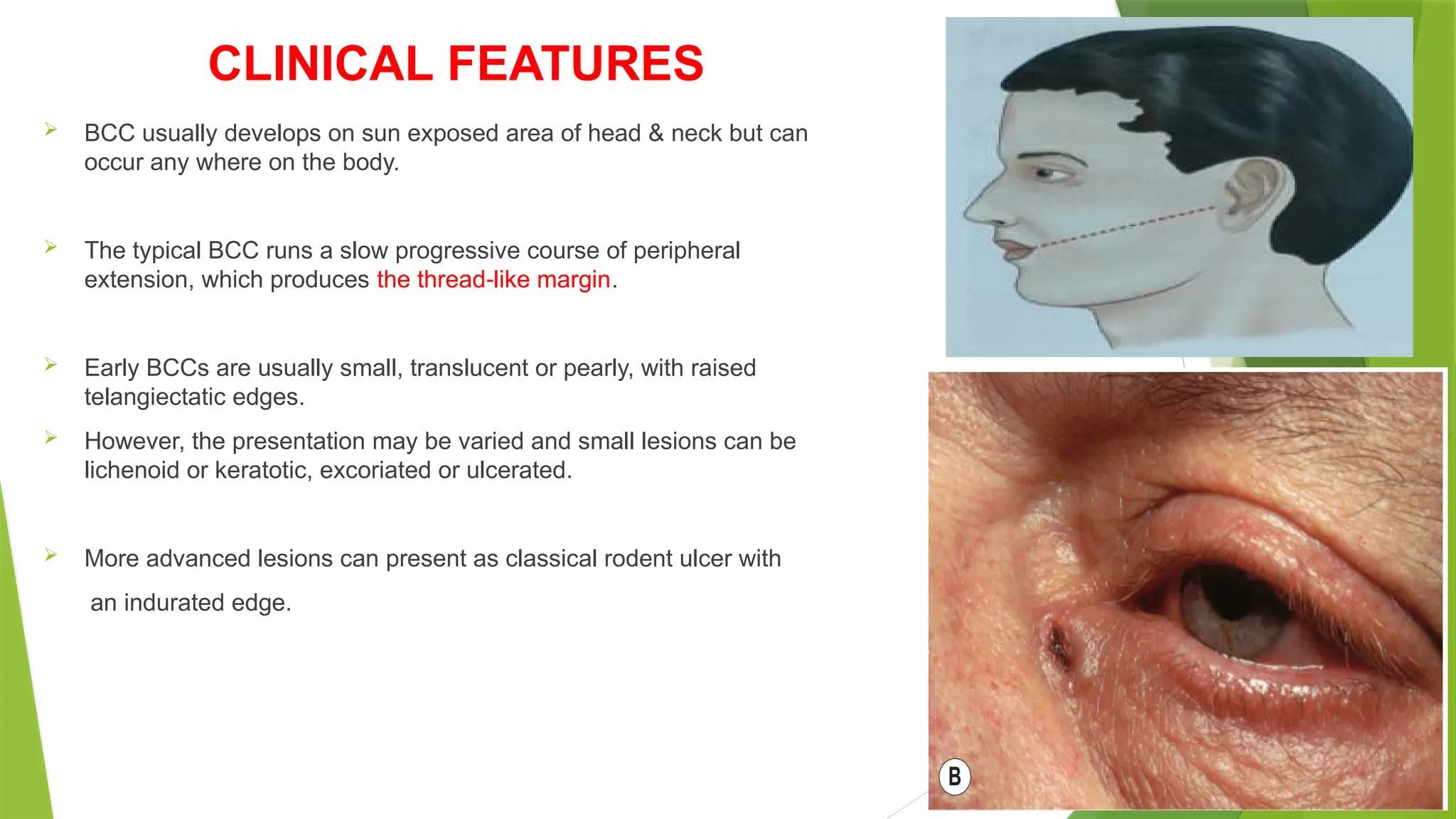
BCCusually develops on sun exposed area of head & neck but can
occur any where on the body.
The typical BCC runs a slow progressive course of peripheral
extension, which produces the thread like margin
‐ .
Early BCCs are usually small, translucent or pearly, with raised
telangiectatic edges.
However, the presentation may be varied and small lesions can be
lichenoid or keratotic, excoriated or ulcerated.
More advanced lesions can present as classical rodent ulcer with
an indurated edge.
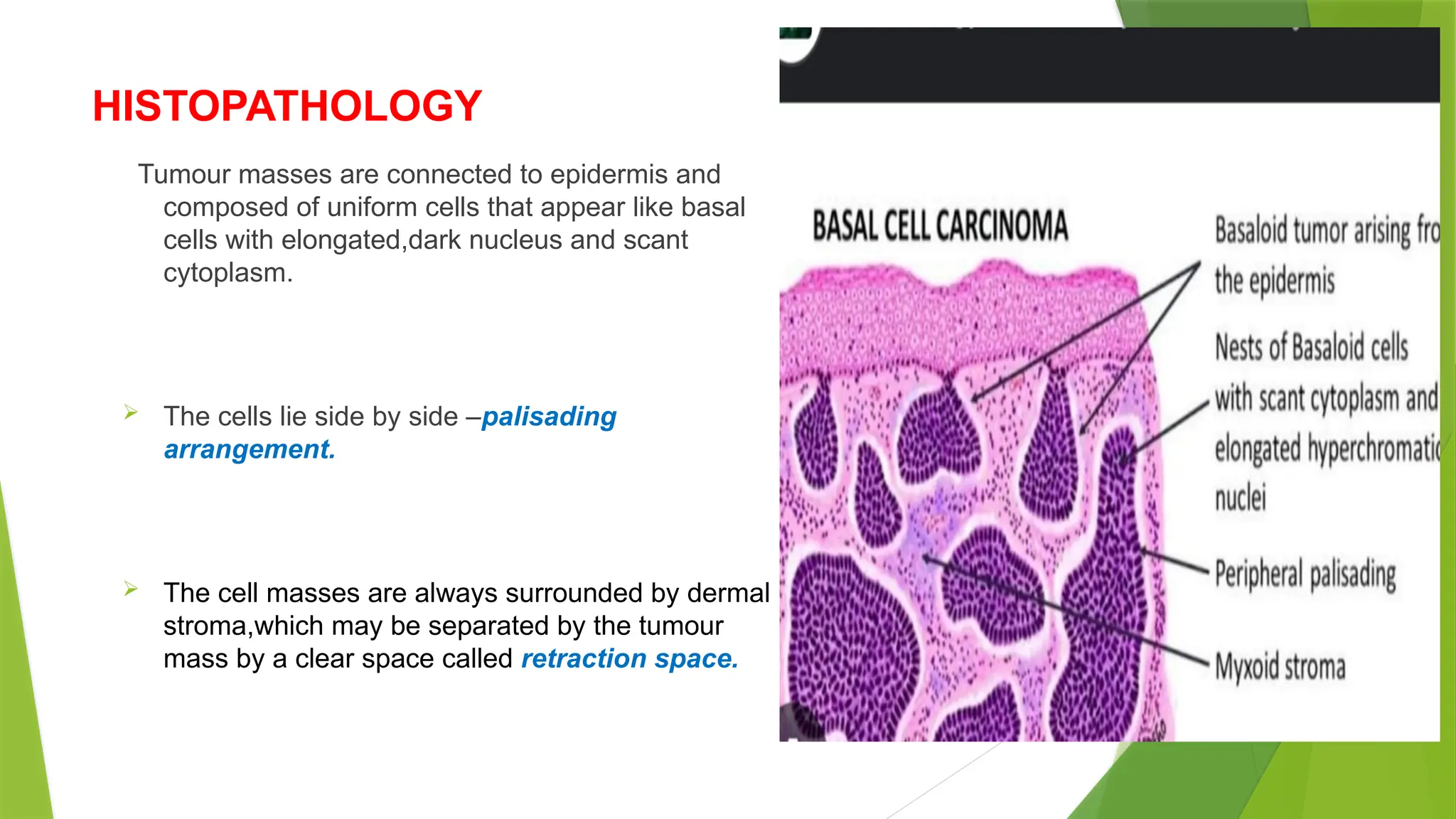
HISTOPATHOLOGY
Tumour masses areconnected to epidermis and
composed of uniform cells that appear like basal
cells with elongated,dark nucleus and scant
cytoplasm.
The cells lie side by side –palisading
arrangement.
The cell masses are always surrounded by dermal
stroma,which may be separated by the tumour
mass by a clear space called retraction space.
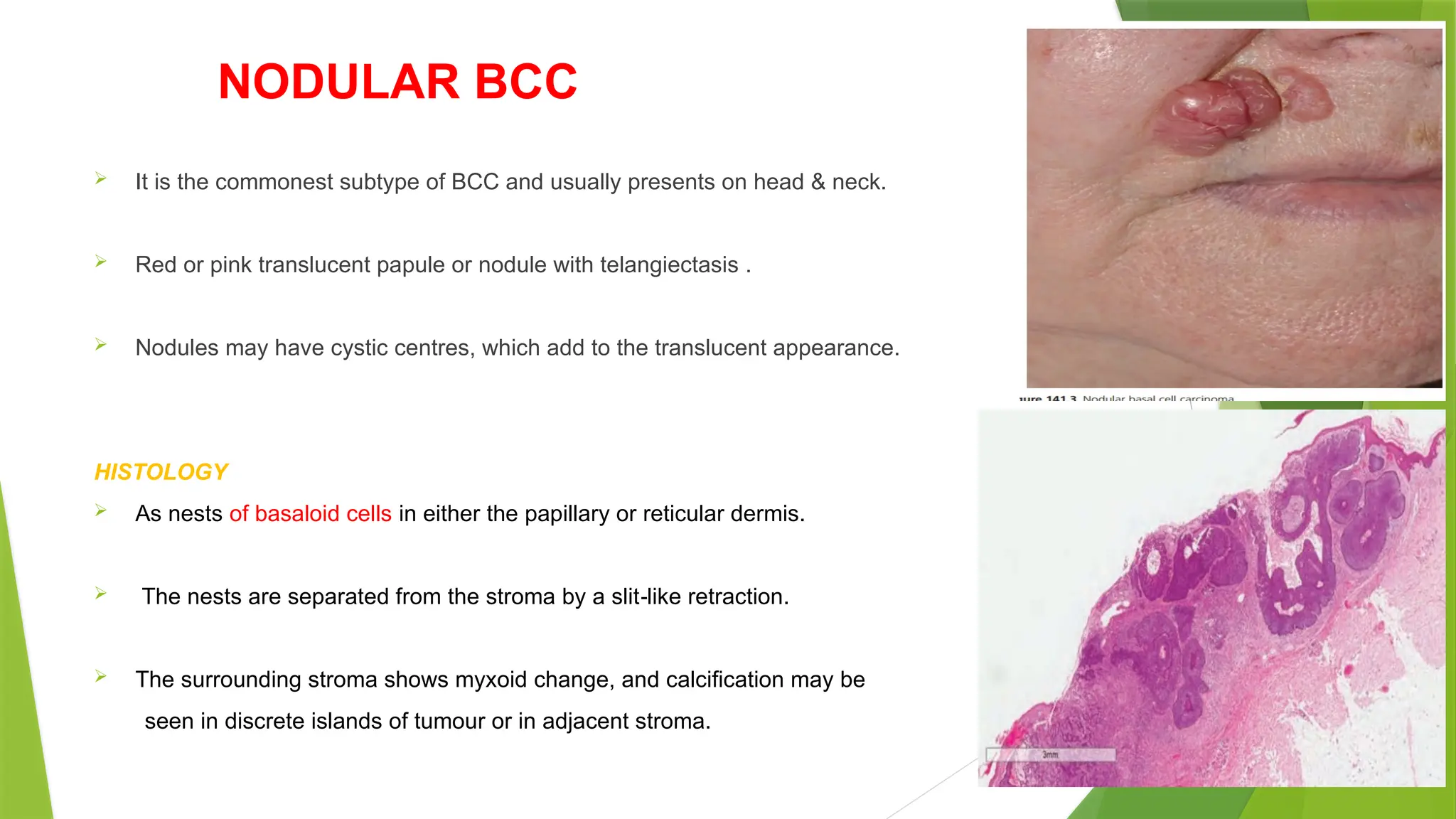
NODULAR BCC
Itis the commonest subtype of BCC and usually presents on head & neck.
Red or pink translucent papule or nodule with telangiectasis .
Nodules may have cystic centres, which add to the translucent appearance.
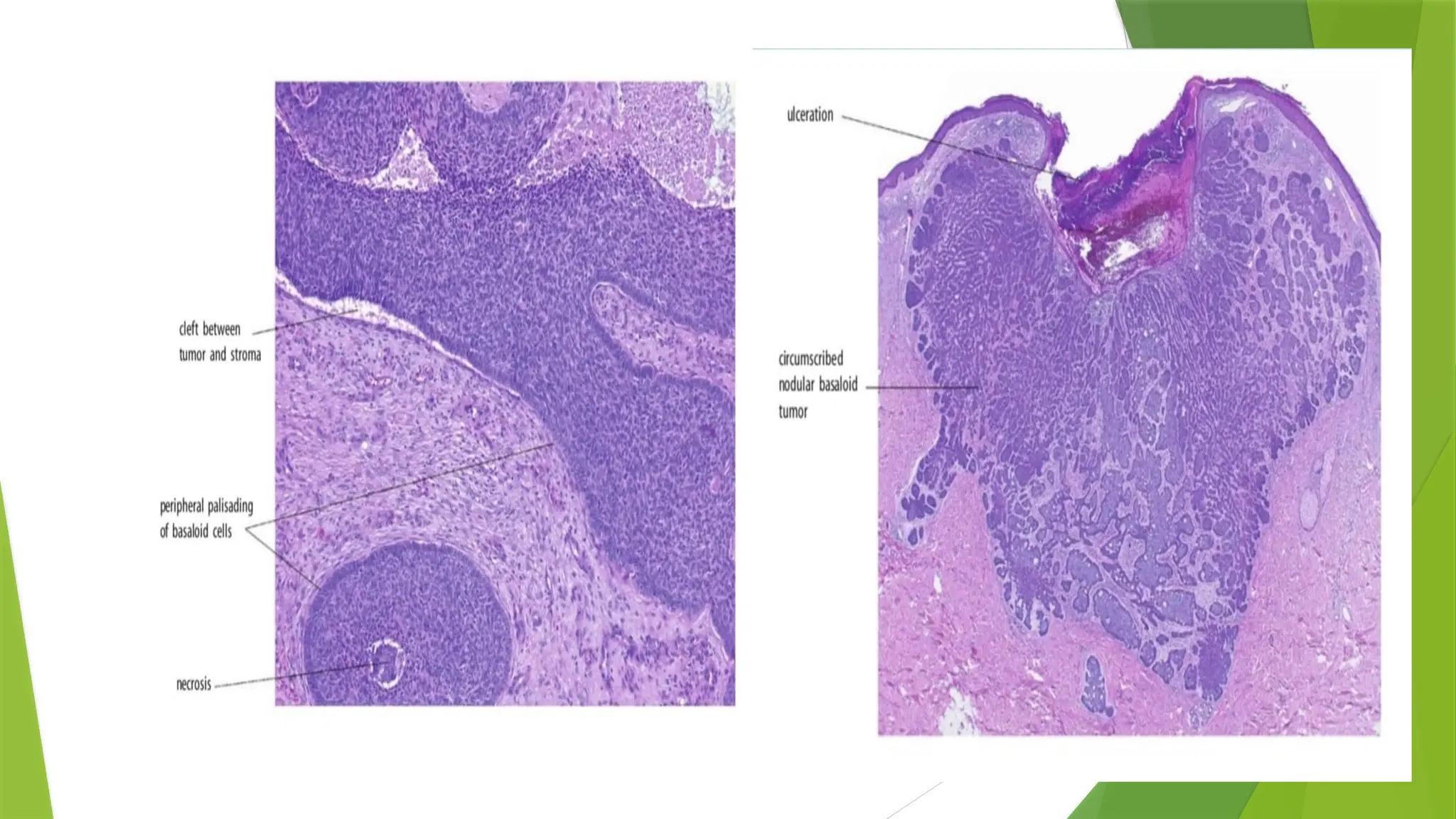
HISTOLOGY
As nests of basaloid cells in either the papillary or reticular dermis.
The nests are separated from the stroma by a slit like retraction.
‐
The surrounding stroma shows myxoid change, and calcification may be
seen in discrete islands of tumour or in adjacent stroma.
19.
SUPERFICIAL BCC
Lesscommon and predominantly present on the trunk.
These are bounded by a slightly raised thread like margin or a ‘whipcord’ edge which is
‐
irregular in outline.
The epidermis covering the central zone is usually atrophic and may be scaly.
HISTOLOGY
Proliferating atypical basaloid cells usually confined to papillary dermis.
A band like lymphoid infiltrate may be present .
‐
20.
PIGMENTED BCC
Sub typeof nodular bcc that exhibits increased melanization.
It appears as translucent , hyperpigmented papule.
Clinically mistaken for nodular melanoma.
HISTOLOGY
Large solid islands of basaloid cells with central pigmentation.
Peripheral palisade is a prominent feature.
Melanocytes are interspersd in b/w tumour cells and contain
numerous melanin granules.
21.
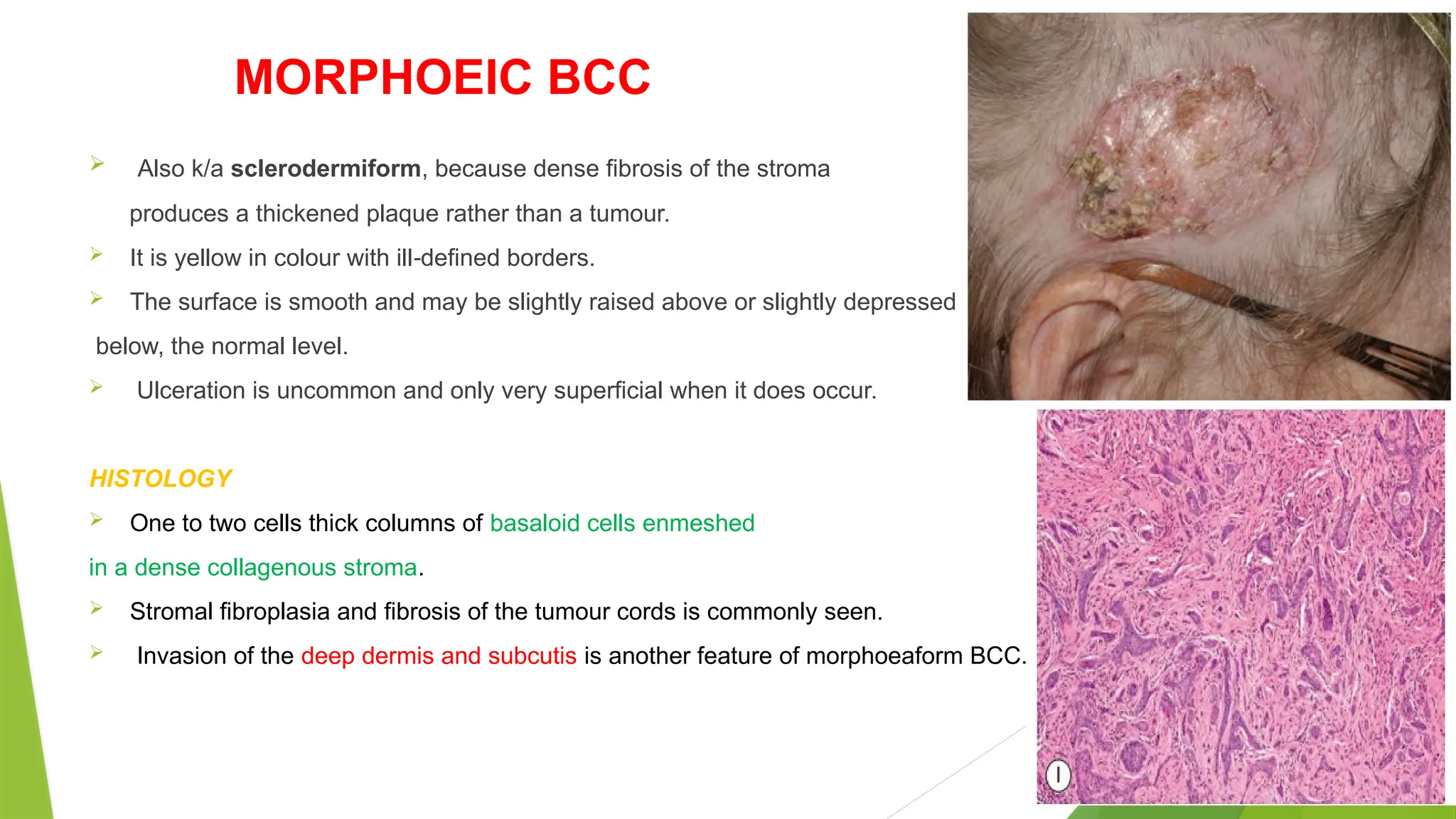
MORPHOEIC BCC
Alsok/a sclerodermiform, because dense fibrosis of the stroma
produces a thickened plaque rather than a tumour.
It is yellow in colour with ill defined borders.
‐
The surface is smooth and may be slightly raised above or slightly depressed
below, the normal level.
Ulceration is uncommon and only very superficial when it does occur.
HISTOLOGY
One to two cells thick columns of basaloid cells enmeshed
in a dense collagenous stroma.
Stromal fibroplasia and fibrosis of the tumour cords is commonly seen.
Invasion of the deep dermis and subcutis is another feature of morphoeaform BCC.
22.
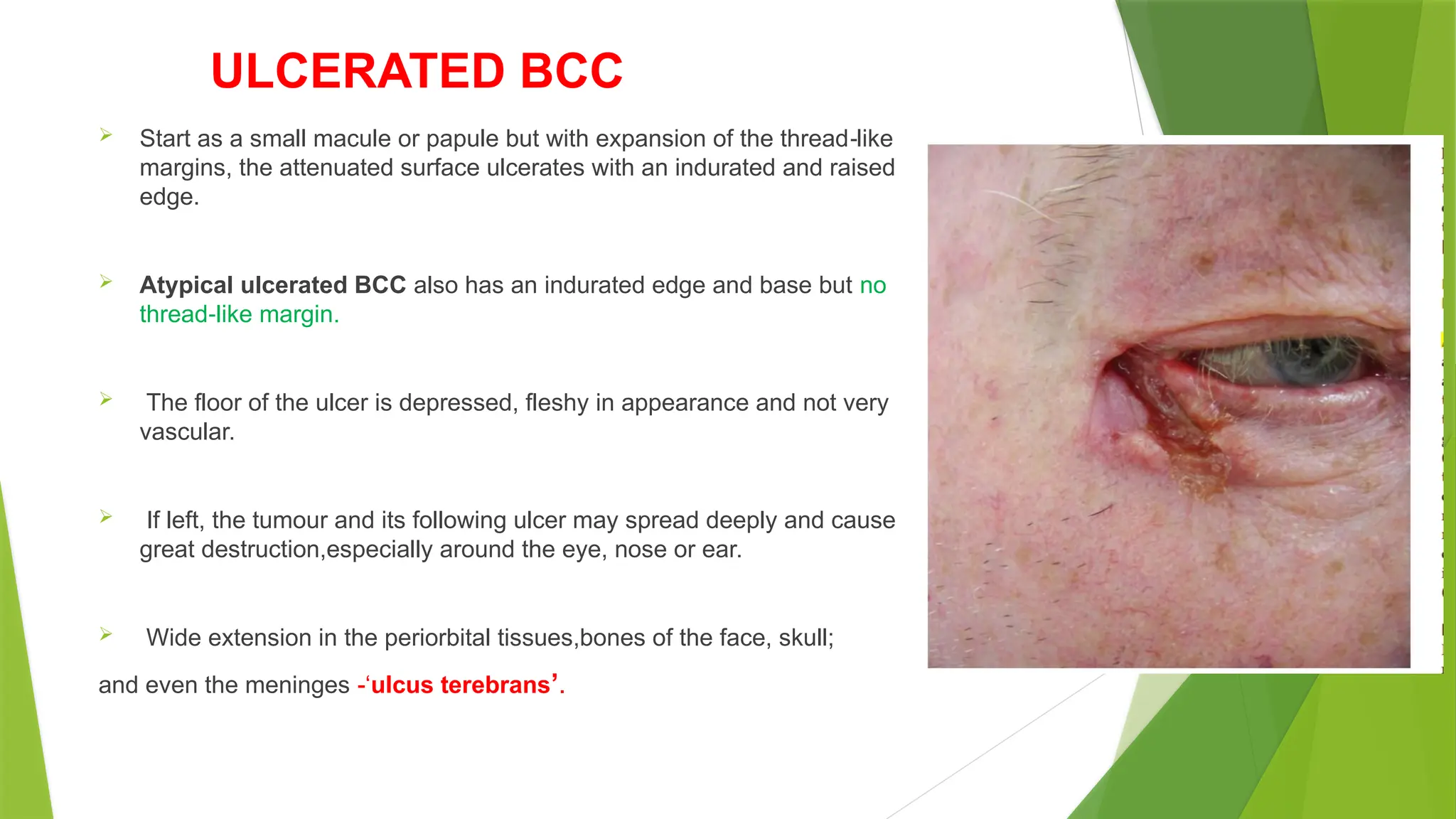
ULCERATED BCC
Startas a small macule or papule but with expansion of the thread like
‐
margins, the attenuated surface ulcerates with an indurated and raised
edge.
Atypical ulcerated BCC also has an indurated edge and base but no
thread like margin.
‐
The floor of the ulcer is depressed, fleshy in appearance and not very
vascular.
If left, the tumour and its following ulcer may spread deeply and cause
great destruction,especially around the eye, nose or ear.
Wide extension in the periorbital tissues,bones of the face, skull;
and even the meninges -‘ulcus terebrans’.
23.
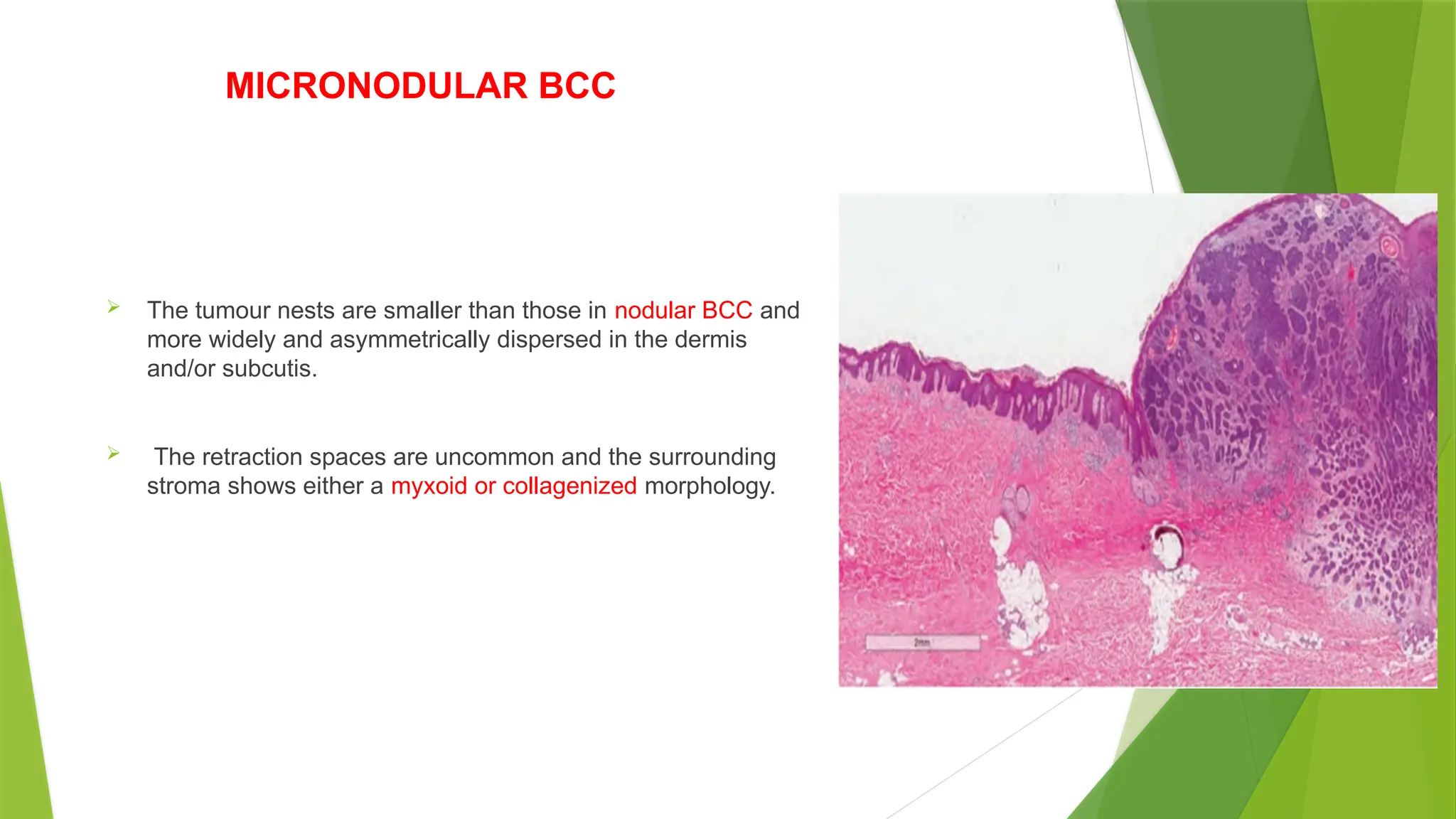
MICRONODULAR BCC
Thetumour nests are smaller than those in nodular BCC and
more widely and asymmetrically dispersed in the dermis
and/or subcutis.
The retraction spaces are uncommon and the surrounding
stroma shows either a myxoid or collagenized morphology.
24.
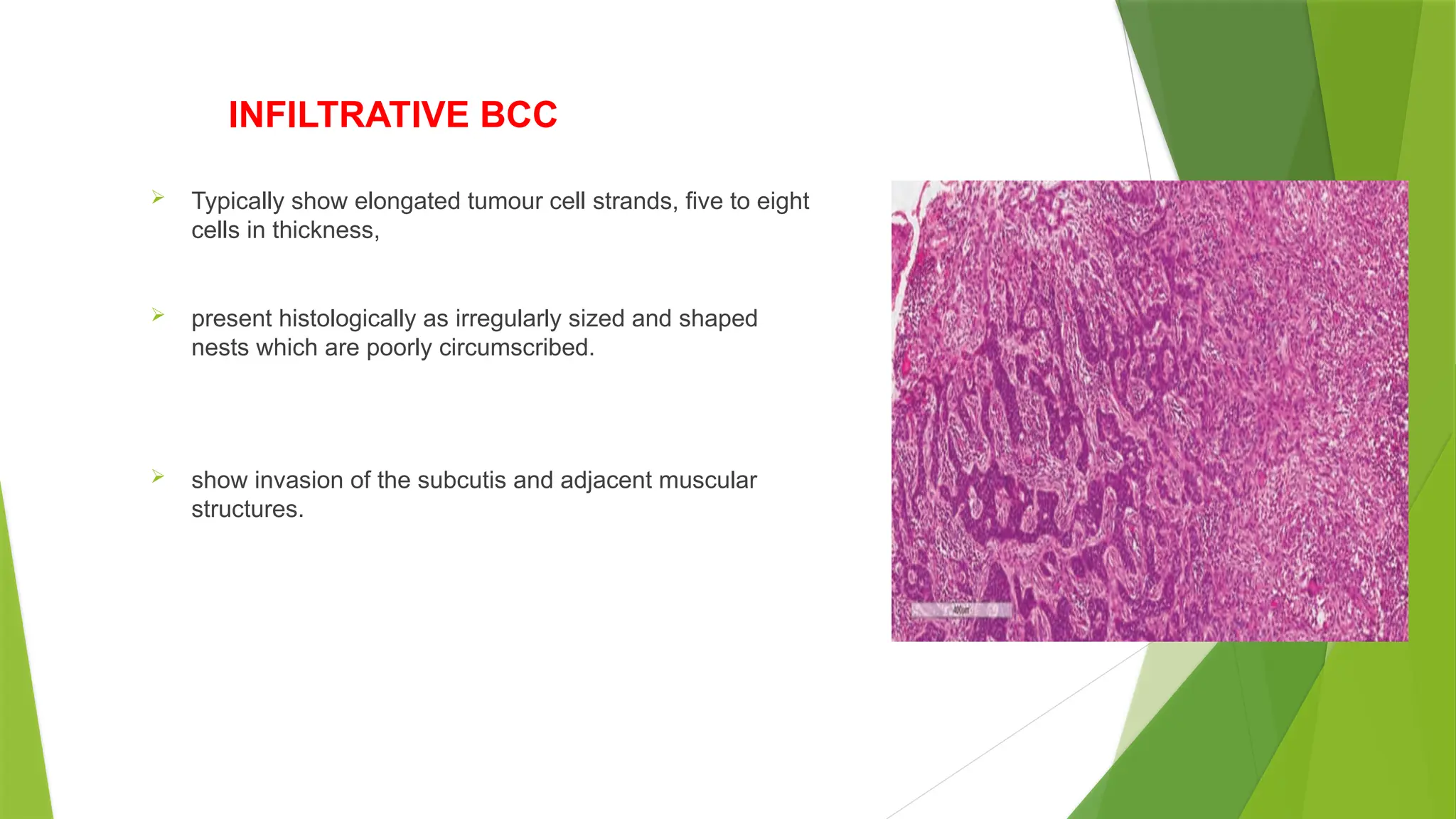
INFILTRATIVE BCC
Typicallyshow elongated tumour cell strands, five to eight
cells in thickness,
present histologically as irregularly sized and shaped
nests which are poorly circumscribed.
show invasion of the subcutis and adjacent muscular
structures.
25.
ADVANCED AND METASTATICBCC
1–2%.
Mutilation of the face or scalp, with destruction of the nose or eye and exposure of the
paranasal sinuses or the skull, dura or brain may eventually result in death .
bloodstream metastasis - deposits in the viscera or spinal column have caused the
symptoms of the terminal illness.
Tumour cells spread via the lymphatics to the regional lymph nodes before disseminating.
26.
FEATURES OF METASTATICBCC
Large size >3cm and locally aggressive
Recurrent
Younger age onset
Morpheaform MC
Median time to metastasise is 9years
10% survival rate.
INVESTIGATIONS
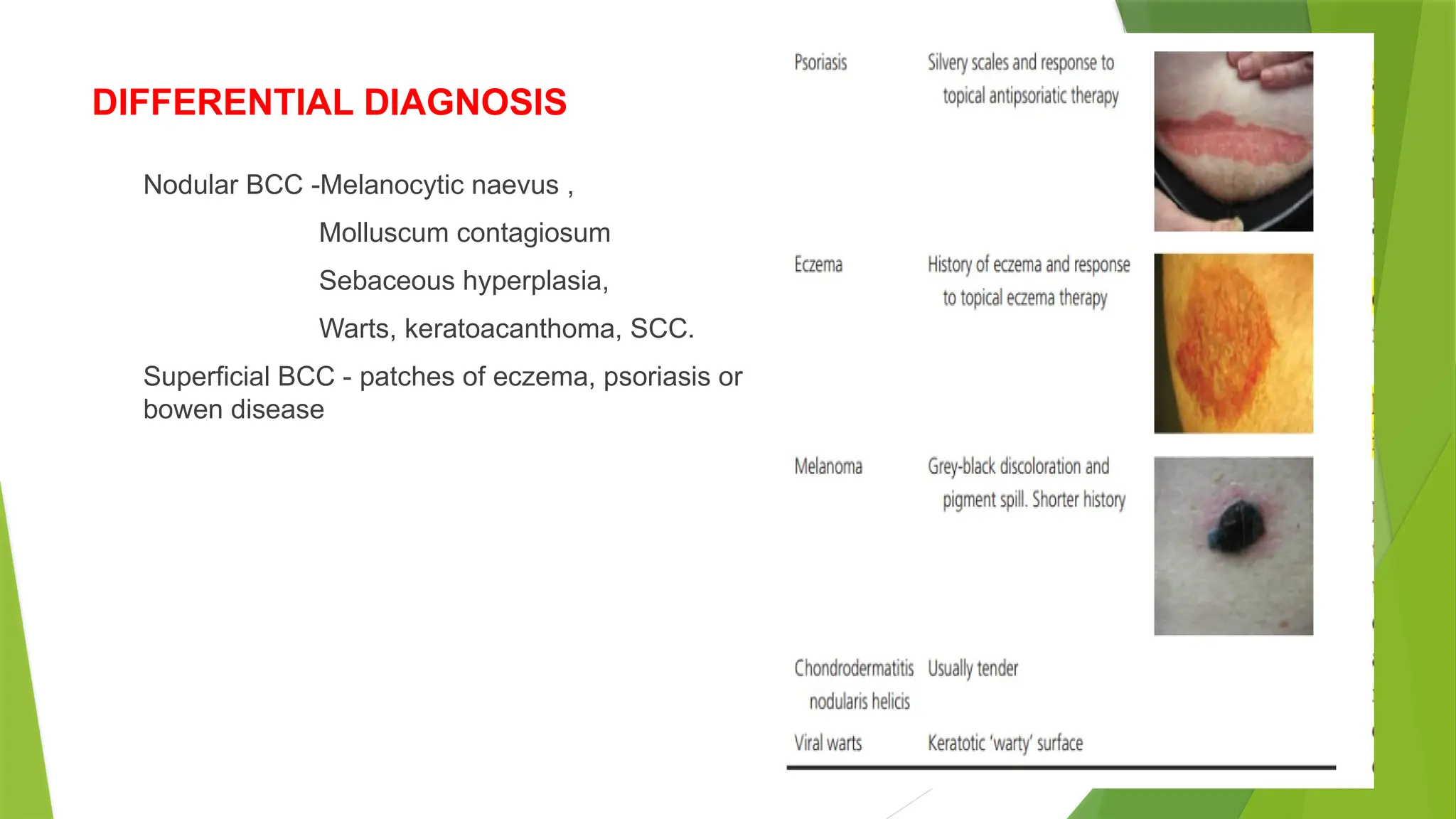
The diagnosisof BCC is primarily clinical.
In clinically challenging cases, a biopsy is required.
Nodular BCC- shave biopsy
Morphoeic BCC - punch biopsy
Non invasive techniques for the diagnosis of BCC include
‐
Dermoscopy
High frequency ultrasound,
‐
Optical coherence tomography and
In vivo confocal microscopy.
30.
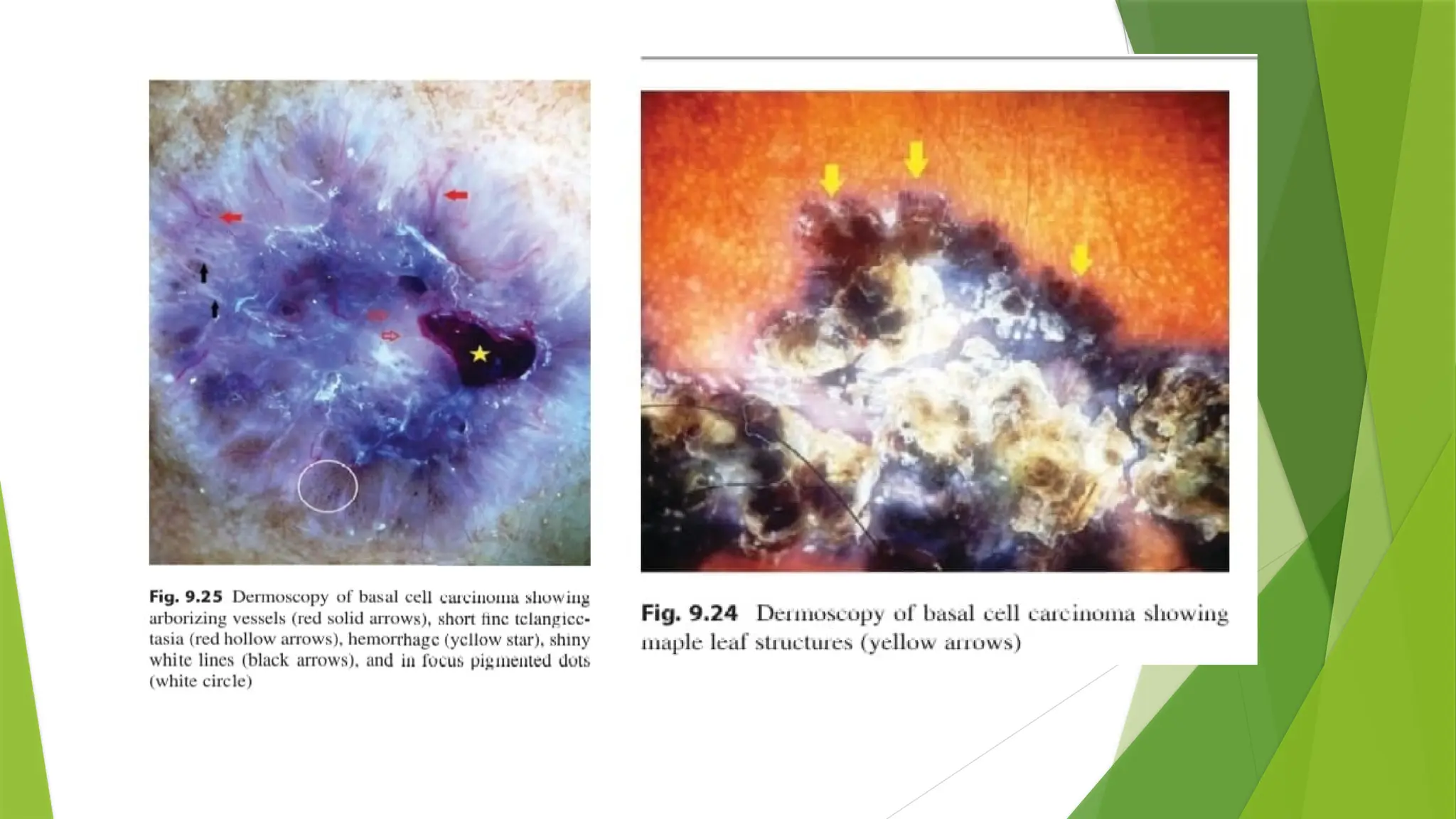
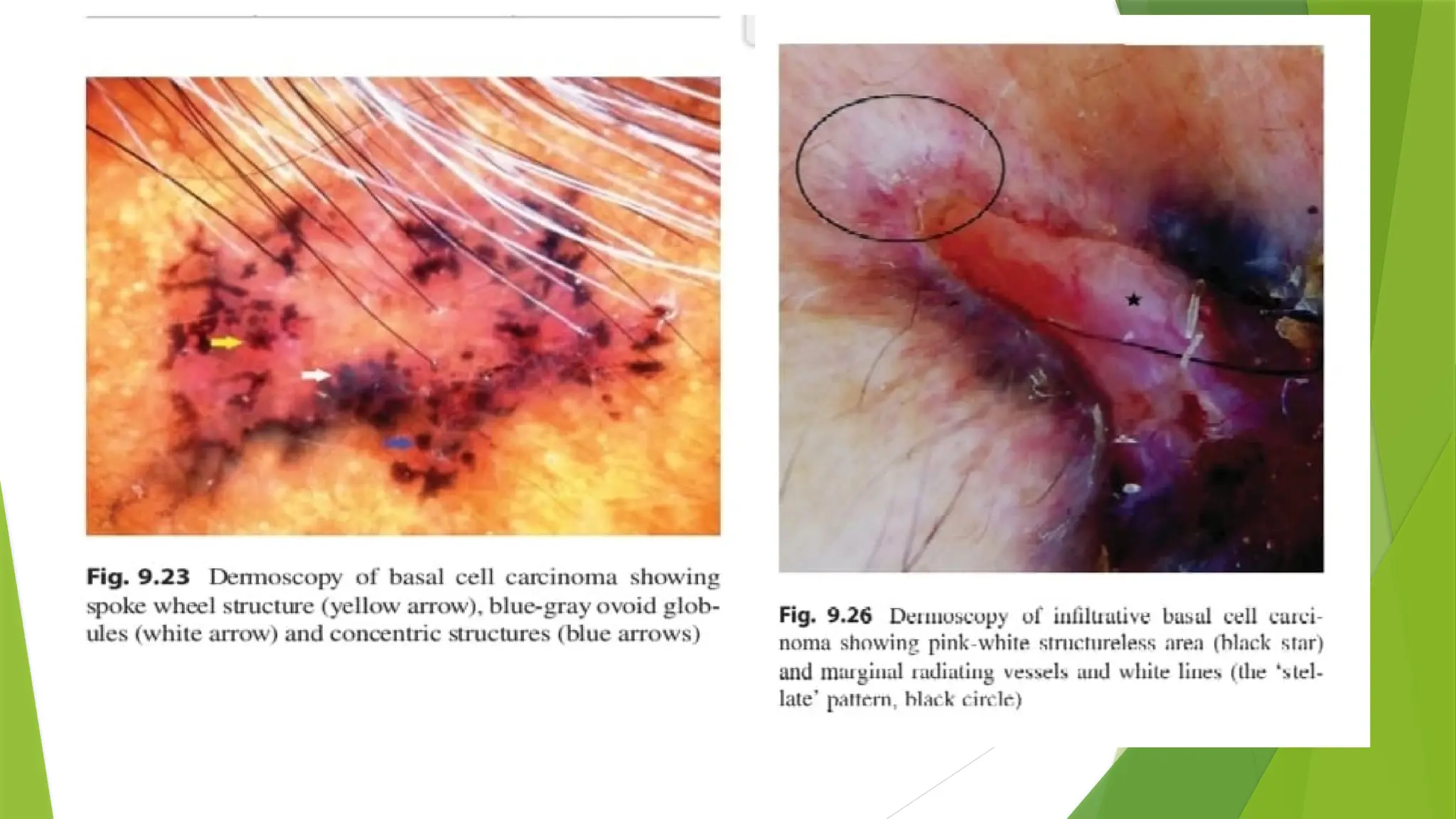
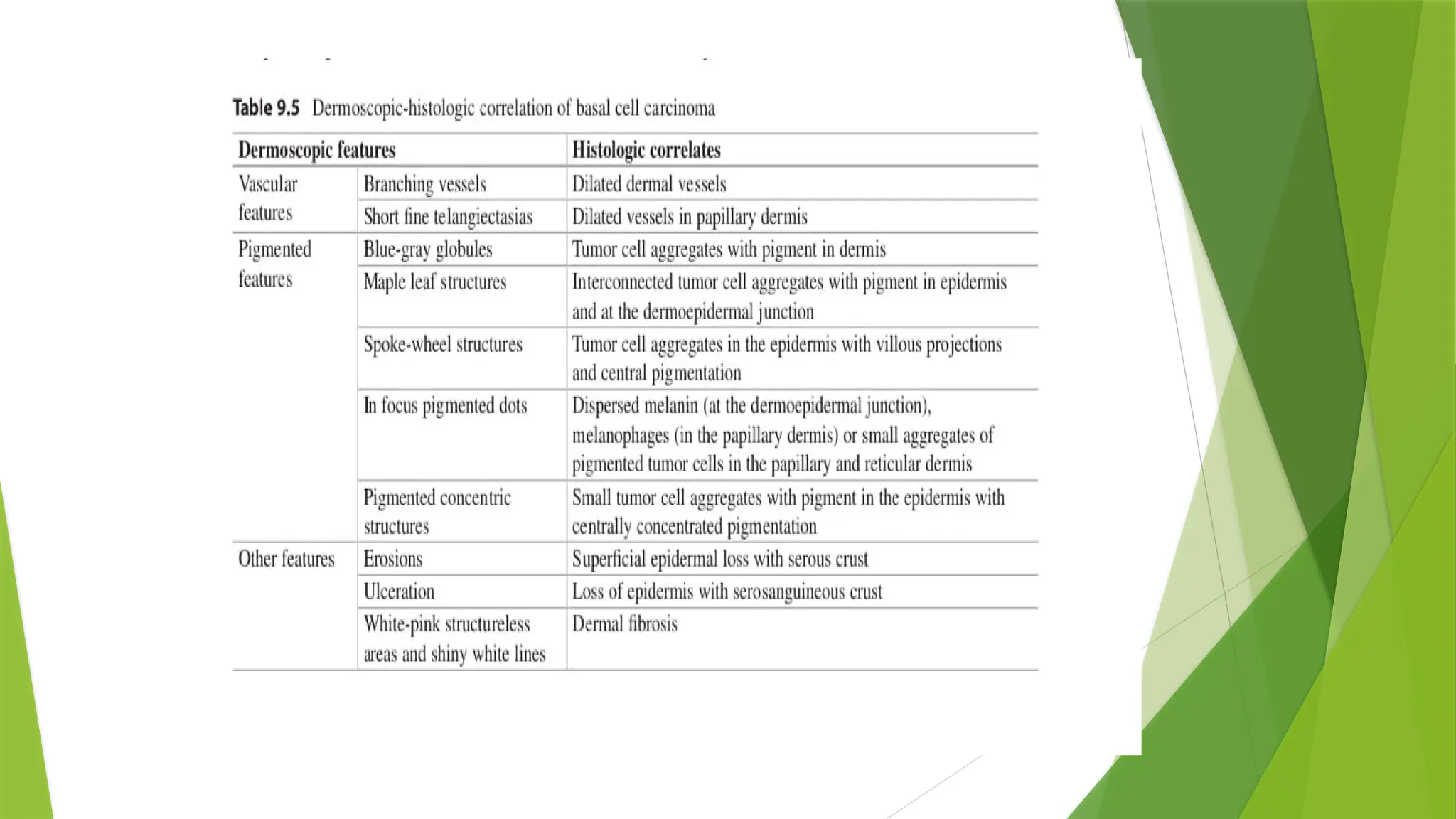
DERMOSCOPY
white andgrey brown structureless areas
‐
blue grey globules
‐
spoke wheel areas
‐
concentric structures
maple leaf like areas
Vasculature includes –
Atypical red , arborizing, comma and
telangiectactic vessels.
34.
MANAGEMENT
Clinical andhistological nature, size and site of tumour & patient factors determine the choice of treatment
of BCC.
AIM OF TREATMENT-
Complete removal or destruction of the BCC.
Achieving a good and acceptable cosmetic outcome.
MEDICAL MANAGEMENT SURGICAL MANAGEMENT
Imiquimod Excision
5FU MMS
PDT C&C
Intralesional INFA-2B Cryotherapy
HH INHIBITORS Lasers
RT
35.
MEDICAL MANAGEMENT
IMIQUIMOD
Stimulates tolllike receptor 7 and 8 expressed on dendritic cells and monocytes,
‐
Leading to increased production of cytokines and chemokines.
Promote both th1 innate and adaptive cell mediated immune responses
‐
Recognition and destruction of the tumour cells.
use in superficial BCC, with a maximum tumour diameter of 2 cm.
Topical 5% imiquimod cream, applied five times per week over 6 weeks is effective in clearing 69–100%
of superficial BCC and 42–76% of nodular BCC.
S/E- Erythema, pruritus, erosion, ulceration, dyspigmentation and scabbing.
Patients may experience flu like symptoms.
‐
36.
5 FLUOROURACIL
‐
5FU used to treat superficial BCCs , not recommended for the treatment of large, nodular
and high risk BCC.
5 FU disrupts DNA and RNA synthesis by inhibiting the enzyme
‐ Thymidylate synthetase.
Local irritation and skin reaction resulting in erythema, swelling, desquamation and
tenderness are common post treatment.
Requires prolonged course,twice daily for 6-12 weeks.
37.
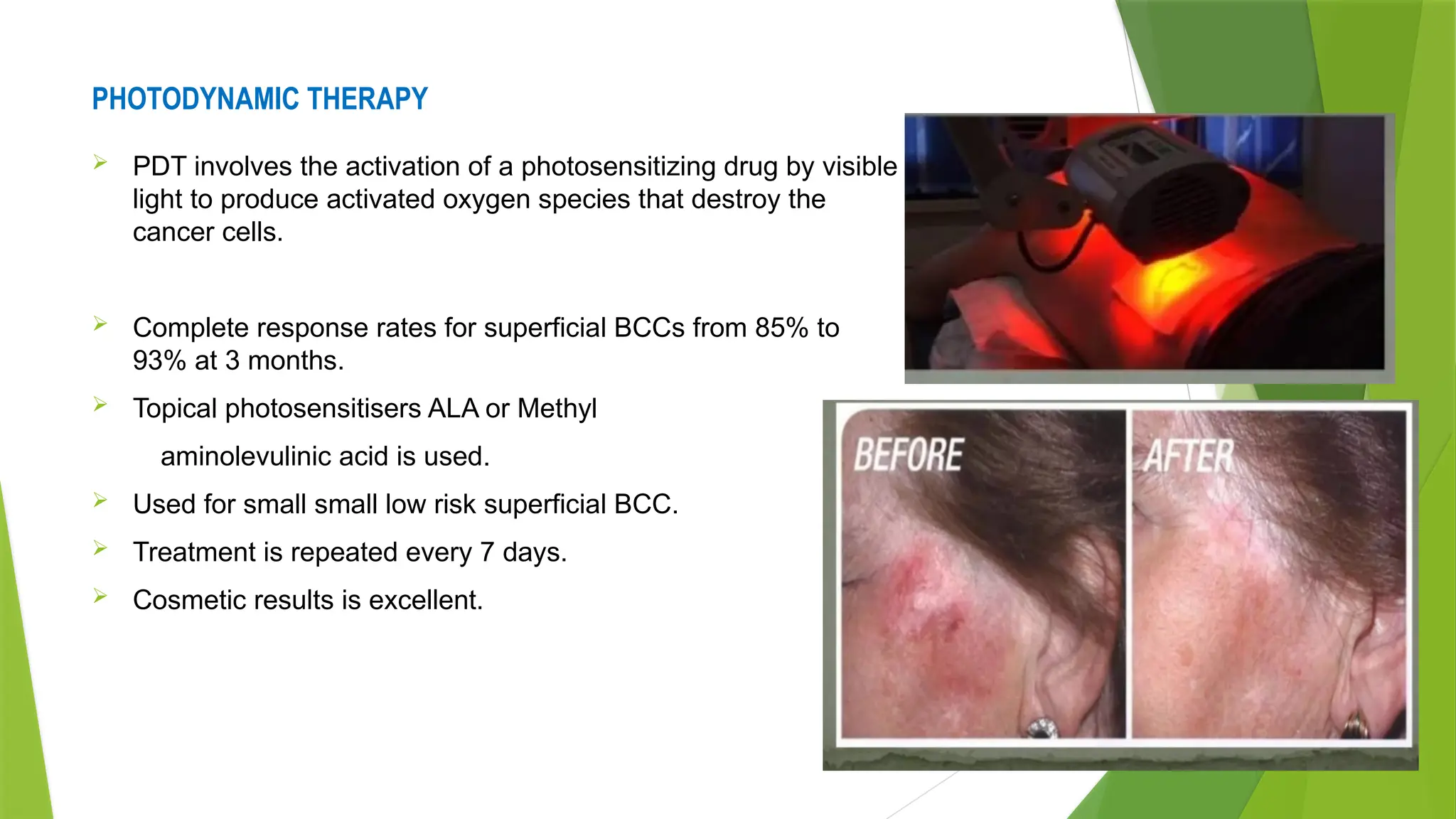
PHOTODYNAMIC THERAPY
PDTinvolves the activation of a photosensitizing drug by visible
light to produce activated oxygen species that destroy the
cancer cells.
Complete response rates for superficial BCCs from 85% to
93% at 3 months.
Topical photosensitisers ALA or Methyl
aminolevulinic acid is used.
Used for small small low risk superficial BCC.
Treatment is repeated every 7 days.
Cosmetic results is excellent.
38.
INTRALESIONAL INFΑ 2B
‐
High cure rates
1.5 million U IL inj ,3times/week for 3 weeks.
Limitations
High cost
Multiple sessions.
HEDGEHOG PATHWAY INHIBITORS
Vismodegib is an inhibitor of SMO used in the treatment of metastatic and locally advanced BCCs
DOSE-150 mg orally daily for 9-10 month.
Adverse reactions - fatigue, weight loss and dyspnoea, muscle spasm , aspiration, back pain, corneal
abrasion, dehydration, hyponatraemia , lymphopenia , pneumonia,
39.
SURGICAL METHODS
Surgical excision–
complete clearance can be achieved in approximately 95% of the well defined small BCC with a 4–5 mm surgical
‐
margin ,
recurrence rates are low
cosmetic outcomes are good.
may not be appropriate for recurrent, morphoeic or large BCC
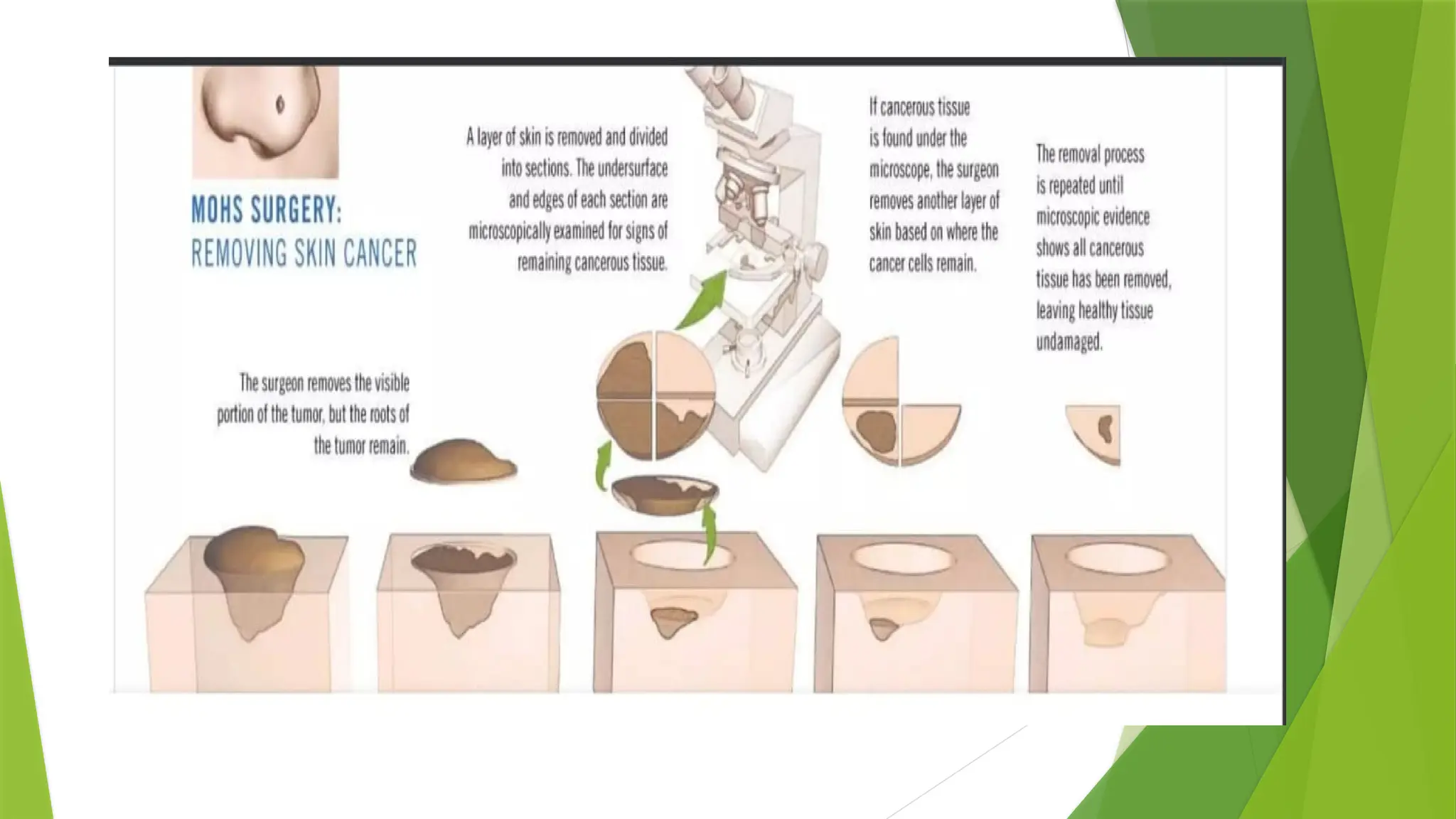
Mohs micrographic surgery
MMS offers superior histologic analysis of tumor margins while permitting maximal conservation of tissue
It is the treatment of first choice for primary & recurrent facial BCCs.
MMS is the treatment of choice for morpheaform, poorly delineated, incompletely removed BCCs.
41.
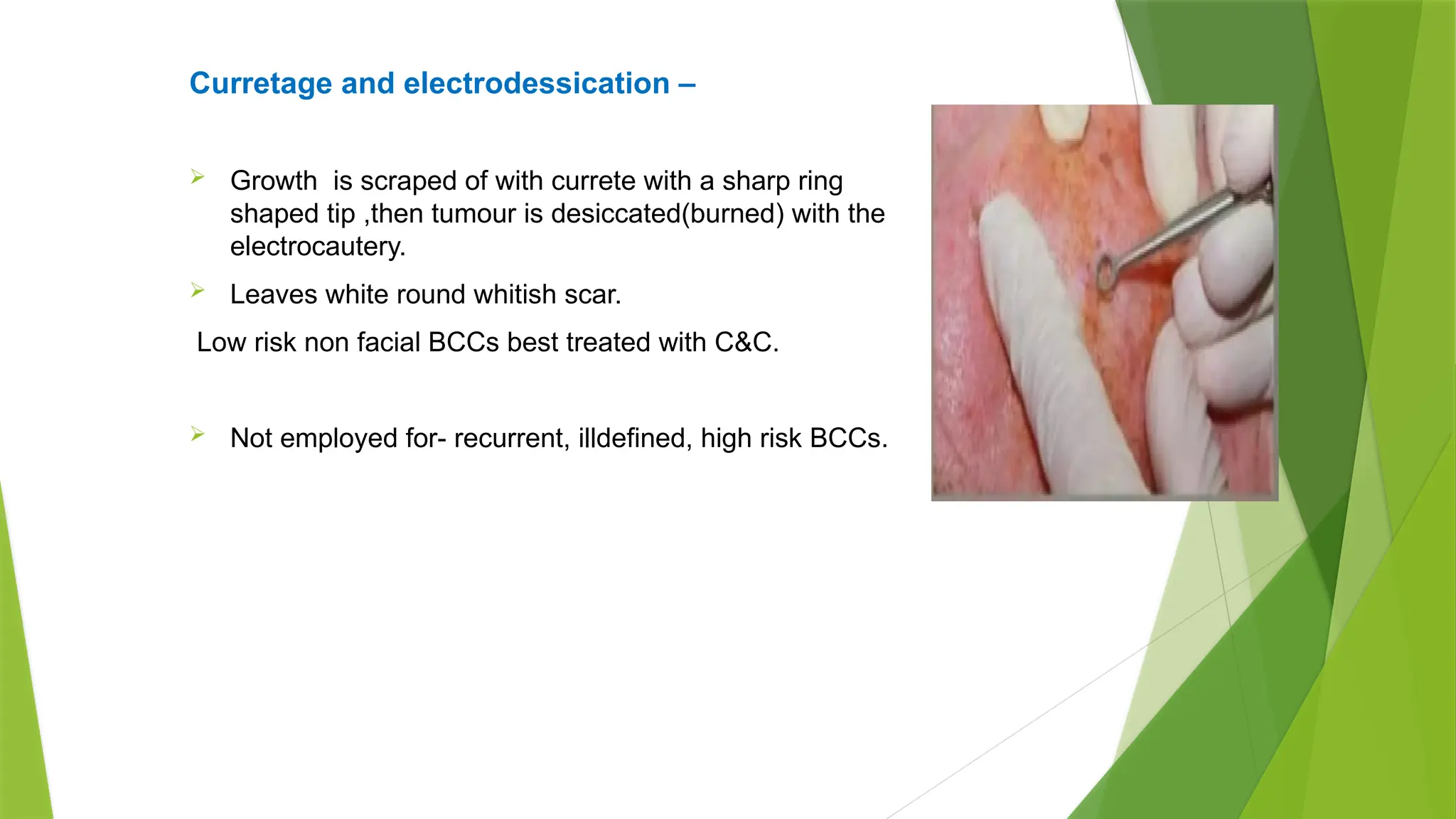
Curretage and electrodessication–
Growth is scraped of with currete with a sharp ring
shaped tip ,then tumour is desiccated(burned) with the
electrocautery.
Leaves white round whitish scar.
Low risk non facial BCCs best treated with C&C.
Not employed for- recurrent, illdefined, high risk BCCs.
42.
CRYOTHERAPY
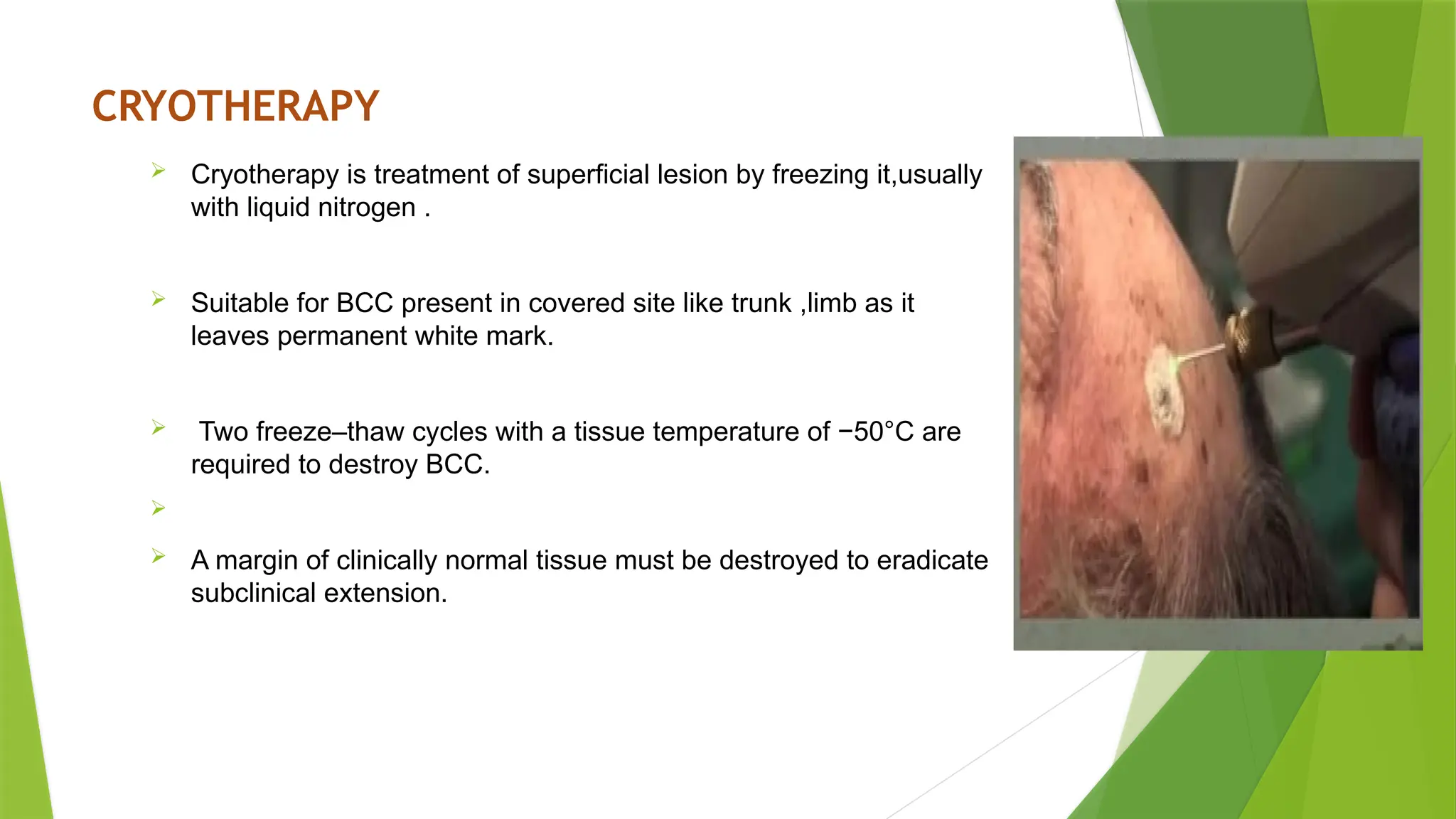
Cryotherapy istreatment of superficial lesion by freezing it,usually
with liquid nitrogen .
Suitable for BCC present in covered site like trunk ,limb as it
leaves permanent white mark.
Two freeze–thaw cycles with a tissue temperature of −50°C are
required to destroy BCC.
A margin of clinically normal tissue must be destroyed to eradicate
subclinical extension.
43.
RADIATION THERAPY
Superficialand electron beam radiotherapy or brachytherapy are effective in primary or surgically recurrent ,
high risk BCC.
‐
RT may be used as a palliative modality in improving the quality of life in patients with advanced disease
Given in fractionated dose of 10-16 fractions for <5cm & 15-30 divided doses for >5cm tumours
RT advantages – effective in troublesome areas nose, ear and eyelid.
useful in elderly patient where surgery can not be performed.
Recurrent tumours,
Disadvantage- Radiation necrosis of skin
Expensive and time consuming as many session needed.
Tumours with poorly defined clinical margins
Incomplete clearance and recurrences after radiotherapy are higher and cosmosis is poor when compared
with surgical excision.