Downloaded 243 times


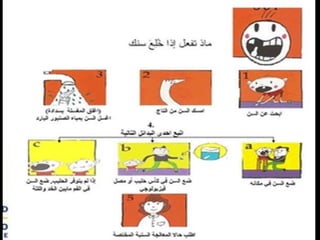

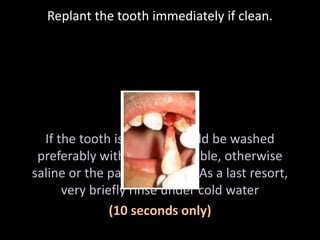



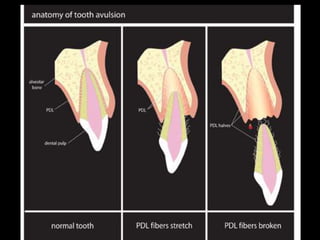




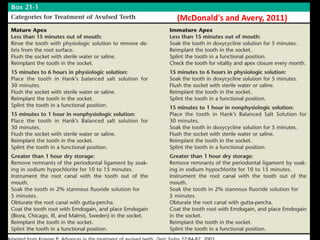


- Avulsion of permanent teeth most commonly involves maxillary central incisors in children ages 7-9 years old when they are erupting. Boys experience avulsion more than girls. - If a tooth is avulsed, it should be replanted immediately if clean or cleaned and replanted. It is important to replant the tooth within 10 minutes for the best prognosis. - After replantation, the tooth should be splinted for 10-14 days and the patient should receive antibiotics and follow up dental treatment which may include root canals or monitoring depending on the maturity of the root.

























![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)





























![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











