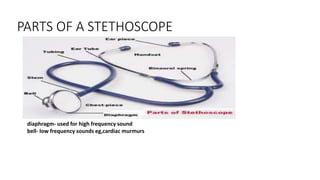
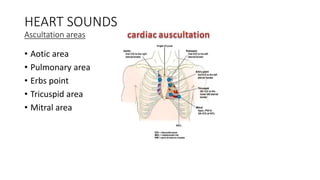
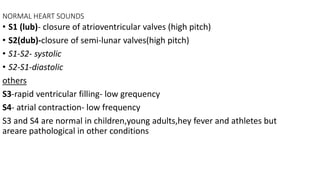
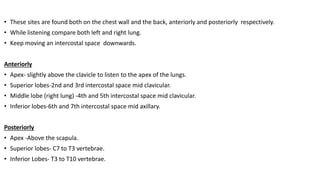
This document discusses auscultation of various body systems including the heart, lungs, abdomen, and arteries. It describes the parts of a stethoscope and locations for listening. For the heart, it covers normal heart sounds and murmurs, including causes and characteristics. Assessment of specific murmurs is also outlined. For the lungs, it describes normal and abnormal breath sounds such as wheezes, crackles, and rubs. Anatomy of the lungs and auscultation sites are provided. The abdomen section notes listening for bowel sounds or bruits. Artery bruits are also discussed.






























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















