
Download to read offline
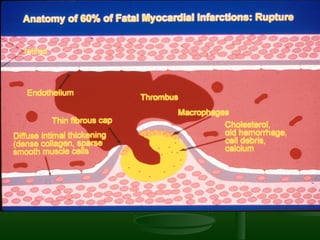
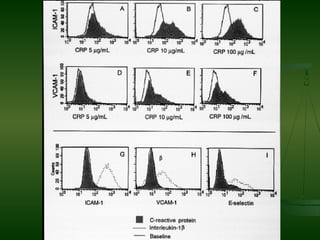

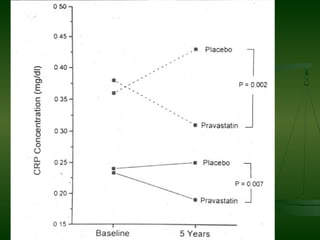
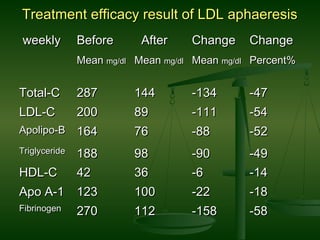
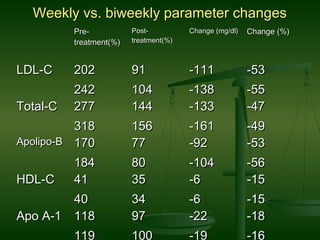
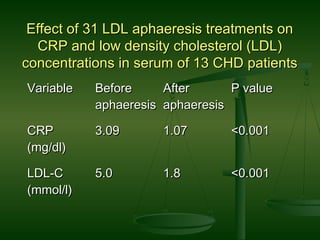
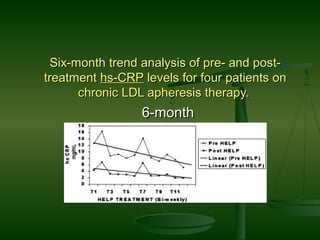
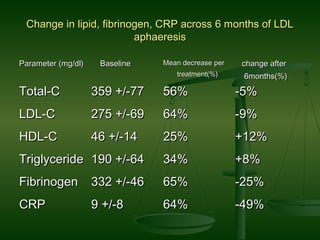
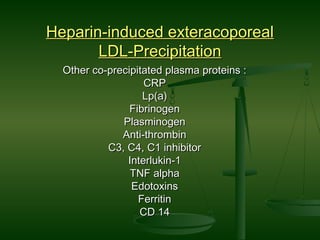
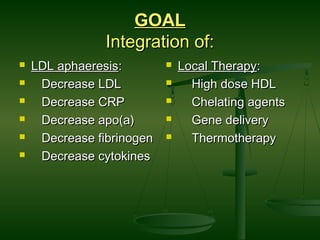
This document discusses atherosclerosis and various therapies aimed at reducing inflammation and LDL levels to treat it. It first covers that atherosclerosis is caused by plaque buildup in arteries and is the leading cause of heart disease. It then discusses evidence that atherosclerosis is an inflammatory condition influenced by inflammatory markers like CRP. The role of therapies targeting LDL, HDL, and inflammation like statins, aspirin, and LDL apheresis are covered. LDL apheresis involves removing LDL and other inflammatory compounds from the bloodstream and clinical trials show it reduces LDL and CRP levels.
































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


