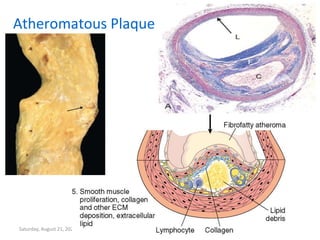
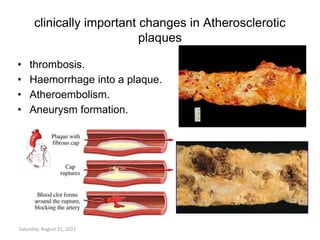
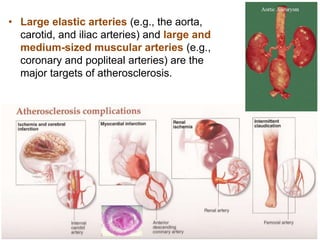
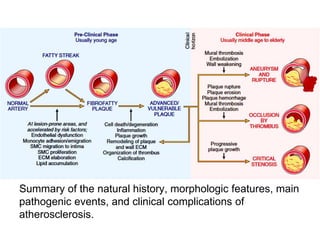
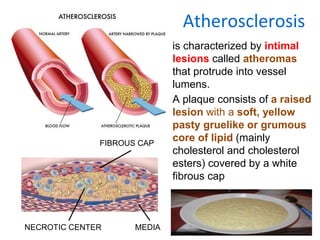
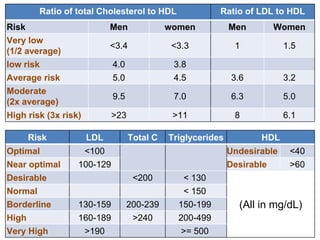
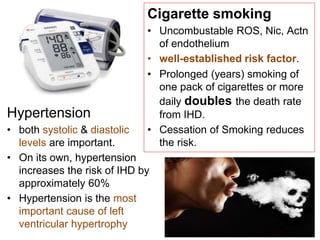
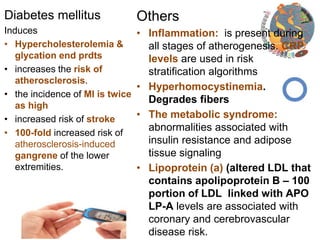
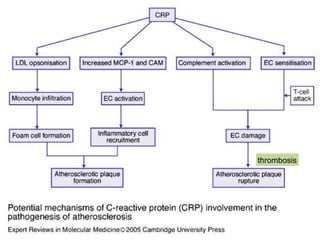
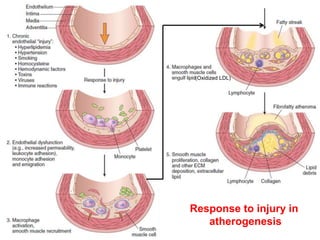
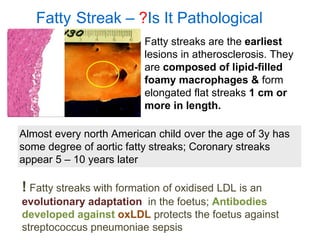
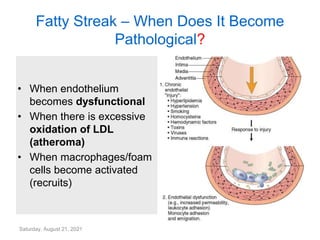
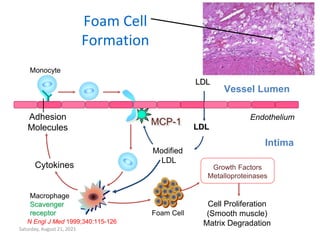
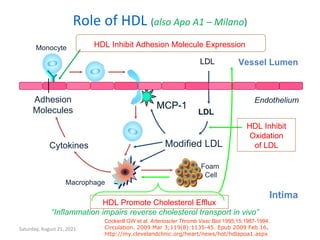
Atherosclerosis is characterized by fatty streaks and plaques within arteries. Plaques consist of accumulated lipids, inflammatory cells, and a fibrous cap. Over time, plaques can rupture, leading to thrombosis. The major risk factors include age, male sex, family history, hyperlipidemia, hypertension, smoking, and diabetes. These risk factors cause endothelial injury and accumulation of lipids in the vessel wall, recruiting monocytes that become foam cells. As plaques grow, they can cause complications like thrombosis, hemorrhage, embolism, or aneurysm.

![Saturday, August 21, 2021
Homocysteine
Homocysteine degrades and inhibits the formation of the three main structural
components of arteries: collagen, elastin and proteoglycans. In proteins, homocysteine
permanently degrades cysteine disulfide bridges and lysine amino acid
residues,[7] affecting structure and function.](https://image.slidesharecdn.com/1797027-231009001036-774d32d1/85/17970_27-1Atherosclerosis-pptx-20-320.jpg)