1) The study aimed to determine if incomplete inhibition of platelet thromboxane production by aspirin (ASA), as measured by urinary 11-dehydro thromboxane B2 levels, was associated with increased cardiovascular risk in patients in the CHARISMA trial.
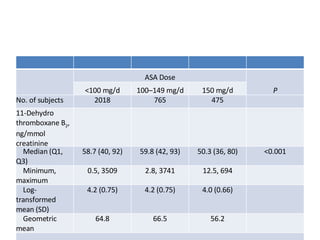
2) Urinary 11-dehydro thromboxane B2 levels were measured in 3261 patients to identify determinants of thromboxane production and whether clopidogrel added to ASA could reduce thromboxane biosynthesis.
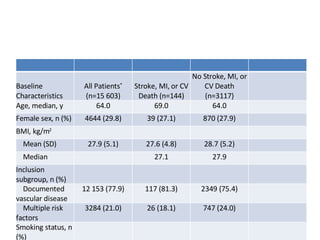
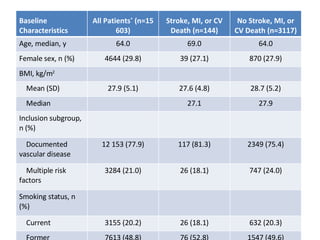
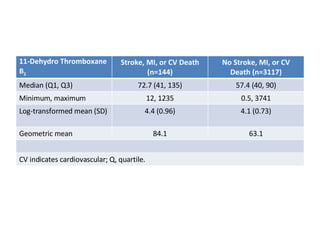
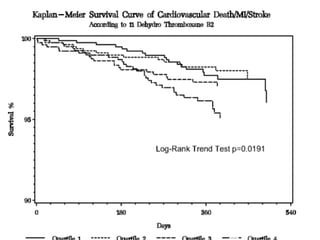
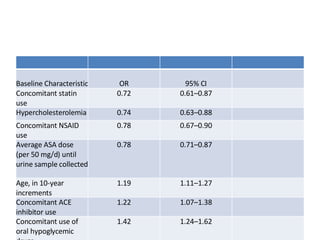
3) Baseline characteristics and outcomes were compared between patients who did and did not experience a primary endpoint of stroke, MI or cardiovascular death during follow-up. Determinants of urinary 11-dehydro throm