resphe inside of the lips, or on the fingernails may happen when a person is not getting as much oxygen as needed. The color of the skin may also appear pale or gray.
Grunting. A grunting sound can be heard each time the person exhales. This grunting is the body's way of trying to keep air in the lungs so they will stay open.
Nose flaring. The openings of the nose spreading open while breathing may indicate that a person is having to work harder to breathe.
Retractions. The chest appears to sink in just below the neck and/or under the breastbone with each breath--one way of trying to bring more air into the lungs.
Sweating. There may be increased sweat on the head, but the skin does not feel warm to the touch. More often, the skin may feel cool or clammy. This may happen when the breathing rate is very fast.
Wheezing. A tight, whistling or musical sound heard with each breath can indicate that the air passages may be smaller, making it more difficult to breathe.
Stridor. An inspiratory sound heard in the upper airway.
Accessory muscle use. The muscles of the neck appear to be moving when your child breathes in. This can also be seen under the rib cage or even the muscles between the ribs.
Changes in alertness. Low oxygen levels may cause your child to act very tired and may indicate respiratory fatigue.
Body positions. Low oxygen and difficulty breathing may force your child to thrust his or head backwards with the nose up in the air (especially if lying down). Or, your child may lean forward while sitting. A child automatically uses these positions as a last attempt to improve breathing.
The signs of respiratory distress may resemble other problems or medical conditions. Always consult your child's healthcare provider for a diagnosis, but if your child is having difficulty breathing, call 911 or go to the closest emergency room.Acute respiratory distress syndrome (ARDS) is the most severe form of acute respiratory failure characterized by diffuse alveolar and endothelial damage. The severe pathophysiological changes in lung parenchyma and pulmonary circulation together with the effects of positive pressure ventilation profoundly affect heart lung interactions in ARDS. The term pulmonary vascular dysfunction (PVD) refers to the specific involvement of the vascular compartment in ARDS and is expressed clinically by an increase in pulmonary arterial (PA) pressure and pulmonary vascular resistance both affecting right ventricular (RV) afterload. When severe, PVD can lead to RV failure which is associated to an increased mortality. The effect of PVD on RV function is not only a consequence of increased pulmonary vascular resistance as afterload is a much more complex phenomenon that includes all factors that oppose efficient ventricular ejection. Impaired pulmonary vascular mechanics including increased arterial elastance and augmented wave-reflection phenomena are commonly seen in ARDS and can additionally affect RV afterload. The use of
VIP ℂall Girls Kandivali west Mumbai 8250077686 WhatsApp: Me All Time Serviℂe...
ards-pocket-card-4.7-qr.pdfrespiratory d
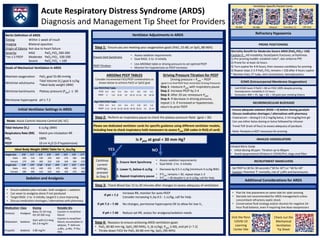
1. Acute Respiratory Distress Syndrome (ARDS)
Diagnosis and Management Tip Sheet for Providers
Berlin Definition of ARDS
Timing Within 1 week of insult
Imaging Bilateral opacities
Origin of Edema Not due to heart failure
Severity
*on ≥ 5 PEEP
Mild
Moderate
Severe
PaO2:FiO2 200-300
PaO2:FiO2 100-200
PaO2:FiO2 < 100
Goals of Mechanical Ventilation in ARDS
Maintain oxygenation PaO2 goal 55-80 mmHg
Minimize volutrauma
Tidal Volume (Vt) goal 6 cc/kg
*Ideal body weight (IBW)
Minimize barotrauma Plateau pressure (Pplat) ≤ 30
Permissive hypercapnia pH ≥ 7.2
Initial Ventilator Settings in ARDS
Step 1: Ensure you are meeting your oxygenation goals (PaO2 55-80, or SpO2 88-96%)
Sedation and Analgesia
Ensure Vent Synchrony
• Assess sedation requirements
• Goal RASS -2 to -3 initially
PEEP Titration
• Use ARDSNet table or driving pressure to set optimal PEEP
• Monitor for hypotension as PEEP increases
Step 2: Perform an inspiratory pause to check the plateau pressure Pplat (goal < 30)
Ventilator Adjustments in ARDS
Please see dedicated ventilator cards for specific guidance using different ventilator models,
including how to check inspiratory hold maneuvers to assess Pplat (QR codes in RUQ of card)
Is Pplat at goal < 30 mm Hg?
YES
Continue
current
settings,
proceed
to Step 3
NO
Step 3: Check Blood Gas 15 to 20 minutes after changes to assess adequacy of ventilation
If pH < 7.2
Increase RR, monitor for auto-PEEP
Consider increasing VT by 0.5 - 1 cc/kg, call for help
If pH 7.2 – 7.40 No changes, permissive hypercapnia OK to allow for low VT
If pH > 7.40 Reduce set RR, assess for analgesia/sedation needs
Step 4: Reassess to ensure achieving ARDS ventilation goals
• PaO2 60-80 mm Hg, SpO2 (90-94%), Vt (6 cc/kg), Pplat (<30), and pH (> 7.2)
• Titrate down FiO2 for PaO2 60-80 mm Hg, SpO2 (90-94%)
Refractory Hypoxemia
PRONE POSITIONING
Mortality Benefit for Moderate-Severe ARDS (PaO2:FiO2< 150)
Caution if… HD instability; facial/pelvic fractures; arrhythmias
1) Pre-proning huddle: establish roles*, don airborne PPE
2) Prone for at least 16 hours
3) Turn supine for 4-8 hours, then reassess candidacy for proning
4) Repeat steps 2-3 if PaO2:FiO2 remains < 150 after 4 hours supine
* Monitor lines, ET tube, vent connections, hemodynamics
NEUROMUSCULAR BLOCKADE
- Ensure adequate sedation (RASS <-4) before staring paralytic
- Discuss medication shortages / alternatives with pharmacy
- Cisatracium – dosing 0.1-0.2 mg/kg bolus, 2-10 mcg/kg/min gtt
- Can use either bolus dosing or bolus followed by infusion
- Trend TOF (train of four) to assess adequacy of paralysis
- Note: Paralysis is NOT necessary for proning
Medication Class Dosing Notable SEs
Fentanyl Analgesic
Bolus 25-50 mcg
Gtt 50-200 mcg
Caution in renal/liver
failure
Midazolam Sedative
Start with 0.5-4mg
Gtt 2-8 mg/hr
Caution in renal/liver
failure; accumulates in
adipose, ↑ delirium
Propofol Sedative 5-80 mg/hr
↓BPs, ↓HRs, ↑TGs;
PRIS
• Ensure sedation plan includes both analgesic + sedation
• Can wean to analgesia alone if not paralyzed
• Target RASS -2 to -3 initially; target 0-1 once improving
• Discuss medication shortages / alternatives with pharmacy
Additional Considerations for ARDS
• Plan for line placement on same side for safer proning
• Steroids not recommended for ARDS management unless
concomitant refractory septic shock
• Conservative fluid strategy and/or diuresis for negative 24-
hour fluid balance, even if requiring low dose vasopressors
INHALED VASODILATORS
Inhaled Nitric Oxide
• Initial dosing 40 ppm. Titration up to 80ppm
• Avoid epoprostenol (iFlolan) in COVID/PUI, clogs viral filter
Mode: Assist Control-Volume Control (AC-VC)
Tidal Volume (VT) 6 cc/kg (IBW)
Respiratory Rate (RR) Match pre-intubation RR
FiO2 100%
PEEP 10 cm H2O (5 if hypotensive)
ECMO (Extracorporeal Membrane Oxygenation)
• Call ECMO team if PaO2 < 80 on FIO2 100% despite proning,
hemodynamic instability X 12 hours
• Exclusions: BMI > 45, Age > 65, > 30 pack year smoking history
RECRUITMENT MANEUVERS
- Set PEEP to 30 for 30 seconds (“30 for 30”) or “40 for 40”
- Caution: Potential ↑ mortality, risk of ↓BPs and barotrauma
Driving Pressure Titration for PEEP
Driving pressure = Pplat – PEEP
(goal is to find PEEP that minimizes Driving Pressure)
Step 1: measure Pplat with inspiratory pause
Step 2: Increase PEEP by 2-4
Step 3: After 20 sec remeasure Pplat
Step 4: If decrease in driving pressure,
repeat 1-3. if increased or hypotension,
return to prior PEEP
ARDSNet PEEP TABLES
Consider incremental FiO2/PEEP combinations as
shown below to achieve PaO2 or SpO2 goal
Ideal Body Weight (IBW) Table for VT 6cc/kg
Height (in) 5'0" 5'1" 5'2" 5'3" 5'4" 5'5" 5'6" 5'7"
Male 300 310 330 340 360 370 380 400
Female 270 290 300 310 330 340 360 370
Height (in) 5'8" 5'9" 5'10" 5'11" 6'0" 6'1" 6'2" 6'3"
Male 410 420 440 450 470 480 490 510
Female 380 400 410 420 440 450 470 480
1. Ensure Vent Synchrony
• Assess sedation requirements
• Goal RASS -2 to -3 initially
2. Lower VT below 6 cc/kg • Decrease by 0.5-1 cc/kg (minimum 4 cc/kg IBW)
3. Repeat inspiratory pause
• If Pplat remains > 30, repeat steps 1-3
• If Pplat > 30 despite Vt at 4 cc/kg, call for help
High PEEP/FiO2 Table
FiO2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
PEEP 5-14 14-16 16-18 18-20 18-20 20-22 22 22-24
Low PEEP/FiO2 Table
FiO2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
PEEP 5 5-8 8-10 10 10-12 12-14 18 18-24
Ventilator Specific Pocket Cards
PB 840 PB 980 Maquet Hamilton C1 OR Vent
Visit the Penn
COVID-19
Learning
Center Site
Check out the
Mechanical
Ventilation
Tip Sheet