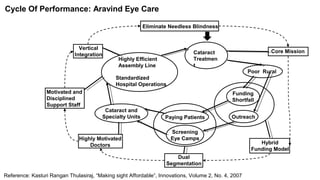
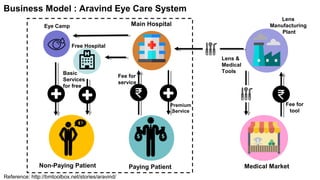
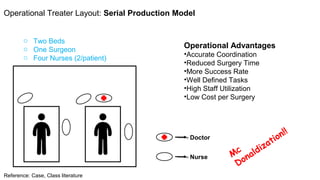
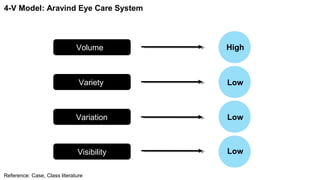
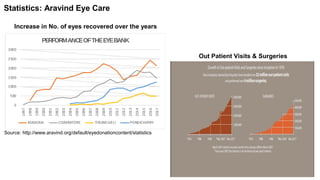
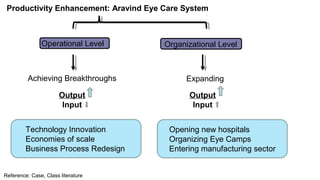
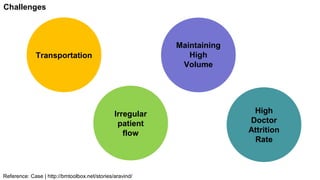
The document presents a case study of the Aravind Eye Care System, showcasing its innovative operational model that combines high-volume, low-cost eye care with a dual financing mechanism catering to both paying and non-paying patients. Founded by Dr. G. Venkataswamy, the system aims to eliminate needless blindness through efficient assembly line practices, outreach programs, and a highly motivated staff. Key challenges include maintaining a strong value system and addressing high doctor attrition rates while adapting to technological advancements.