The document discusses three scales used to assess anxiety:
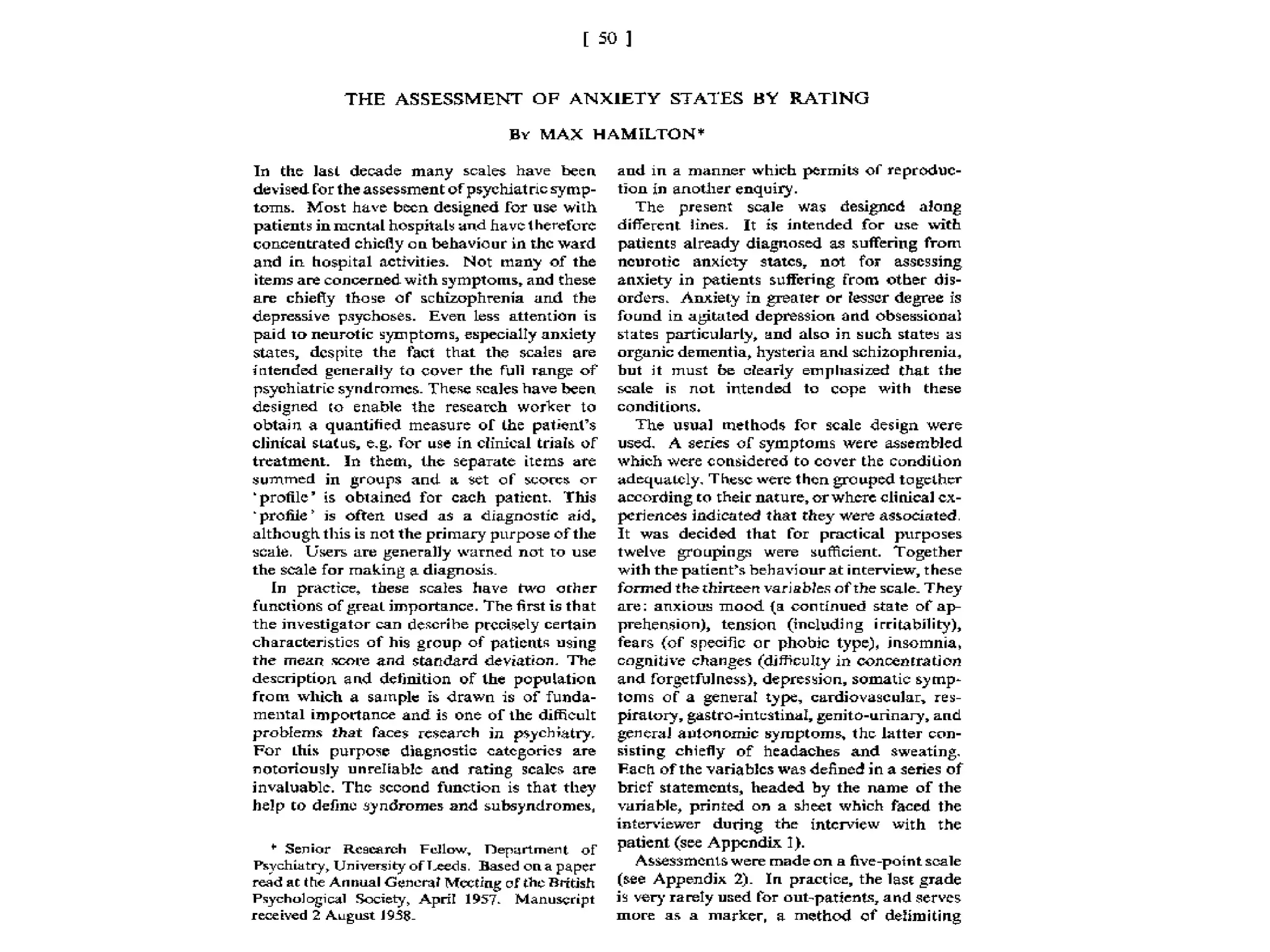
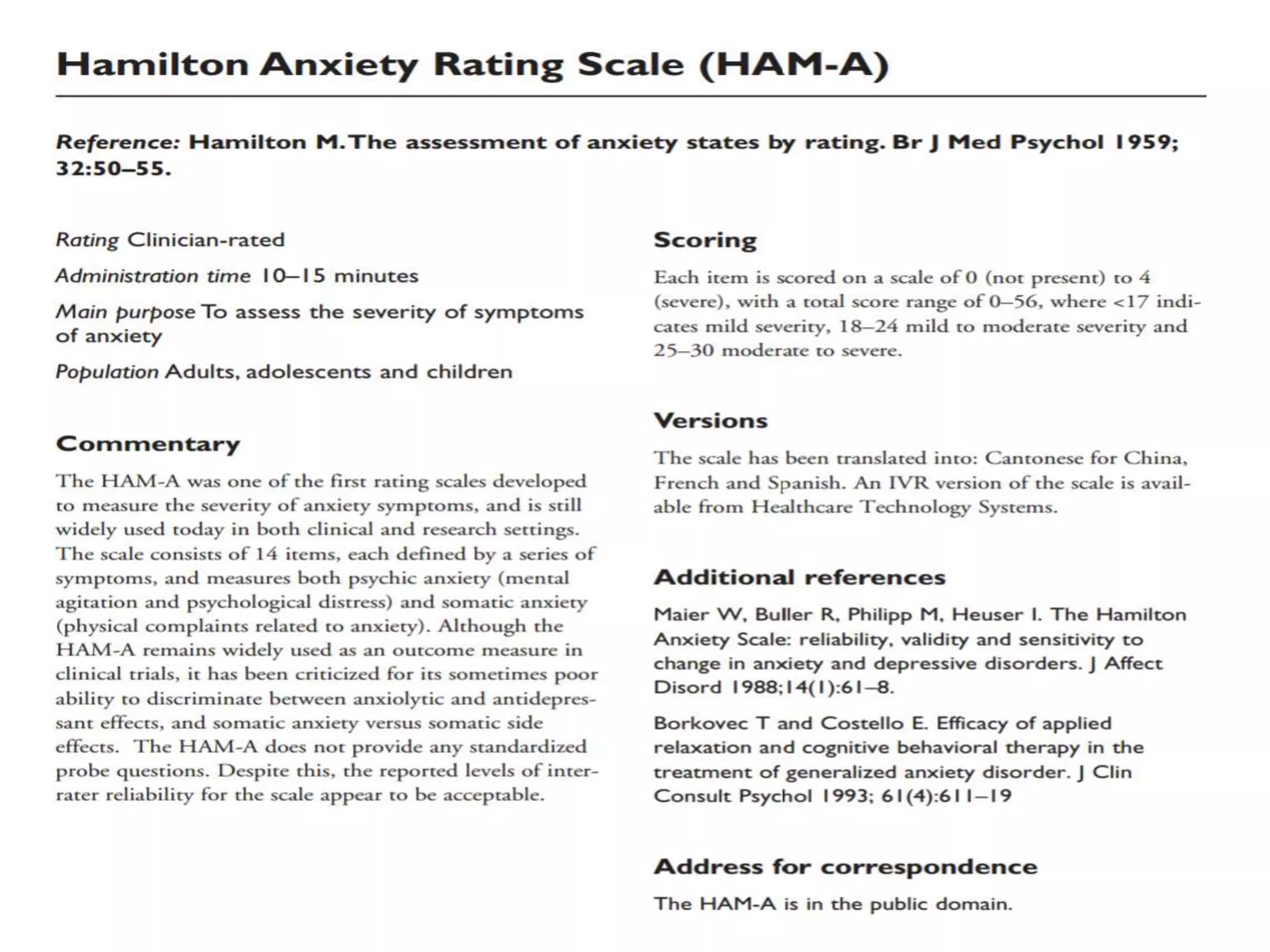
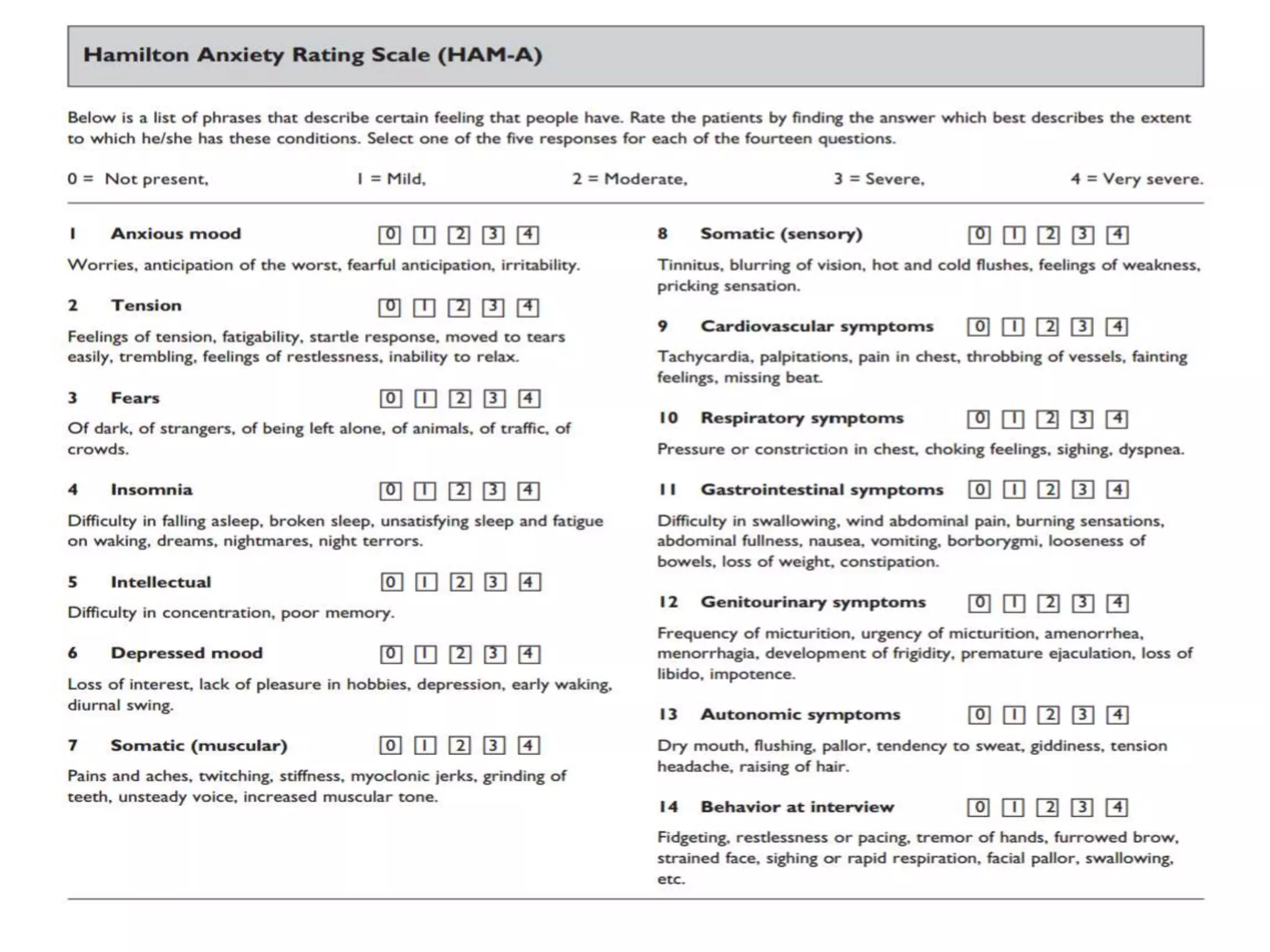
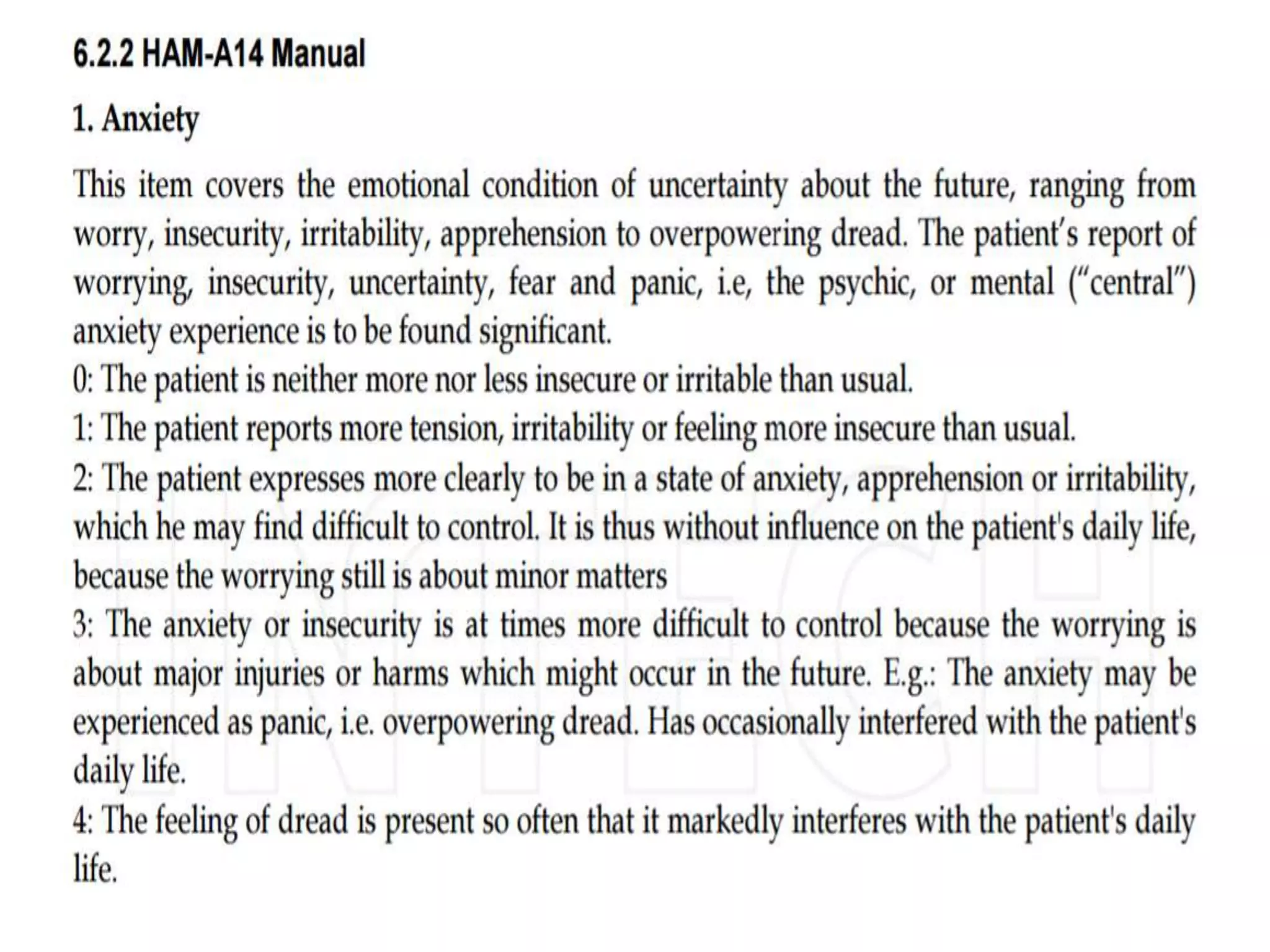
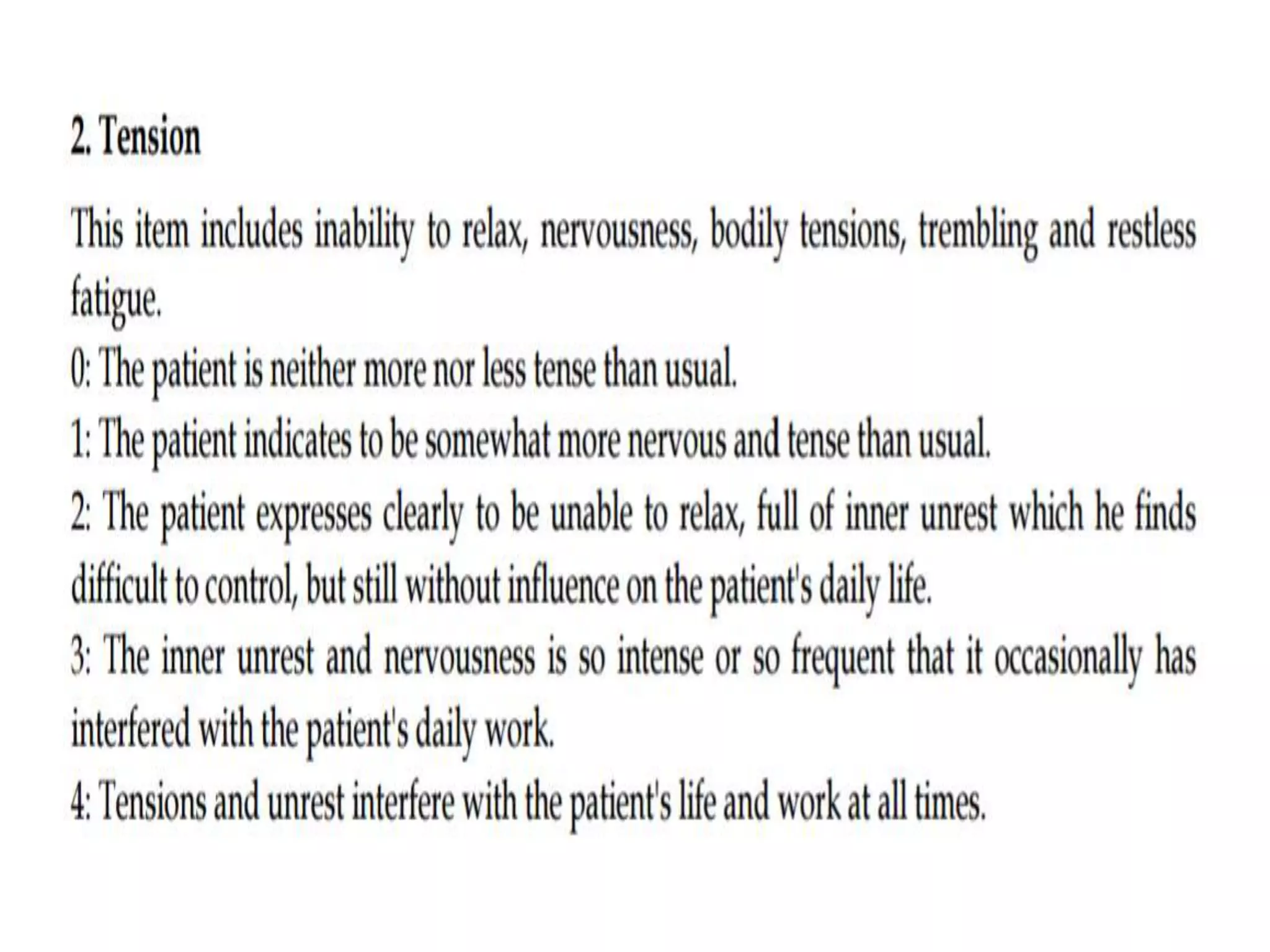
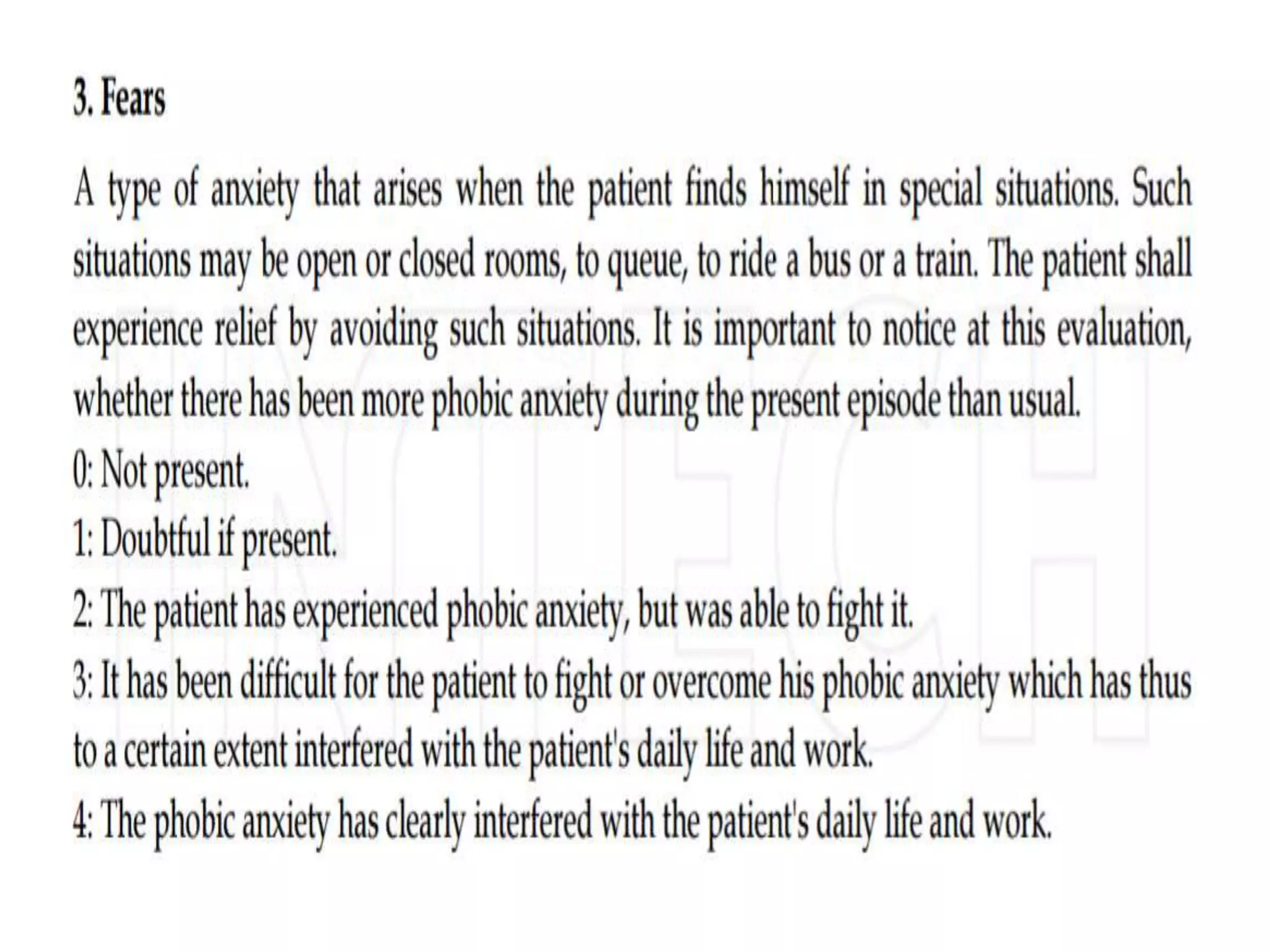
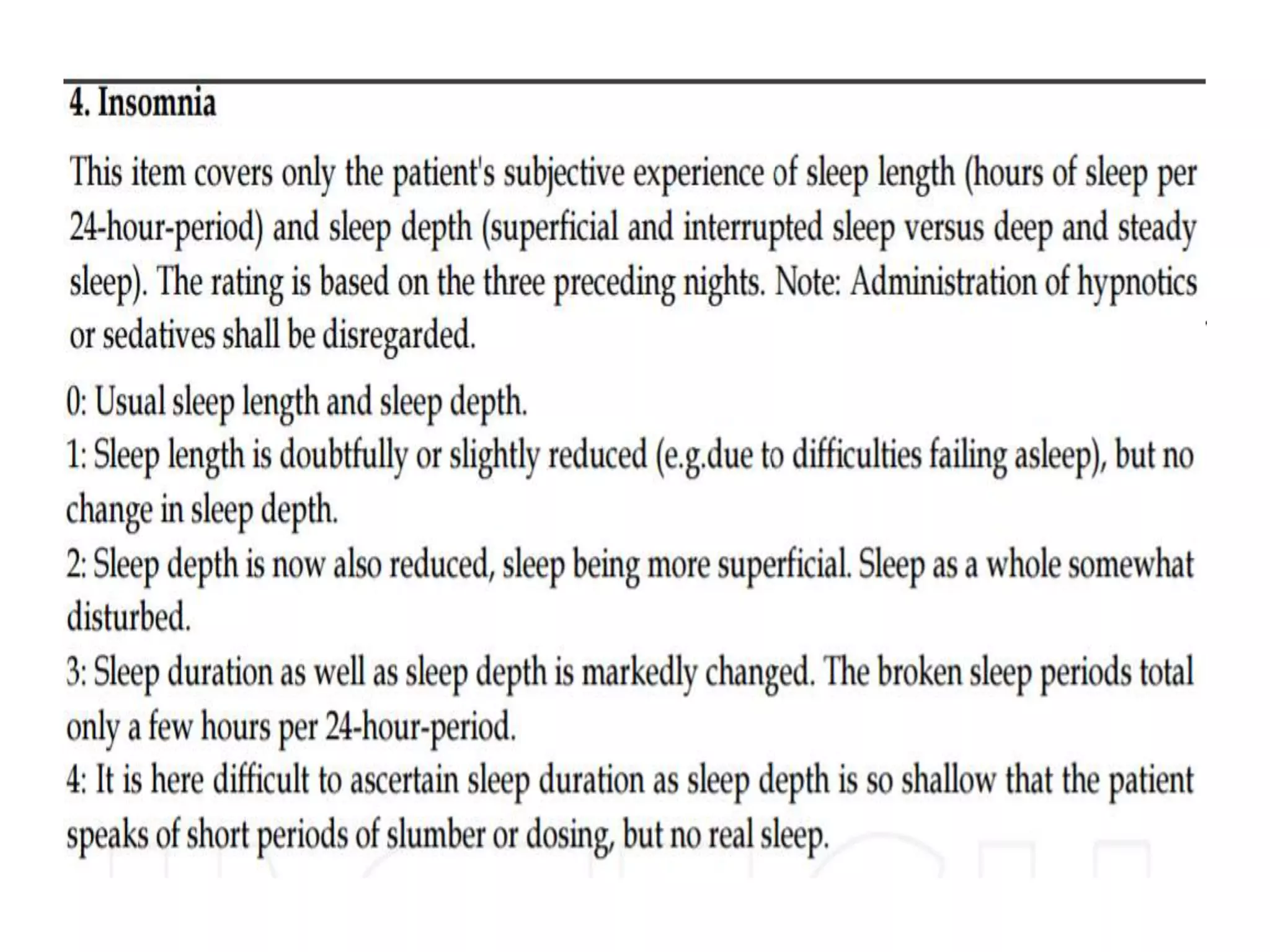
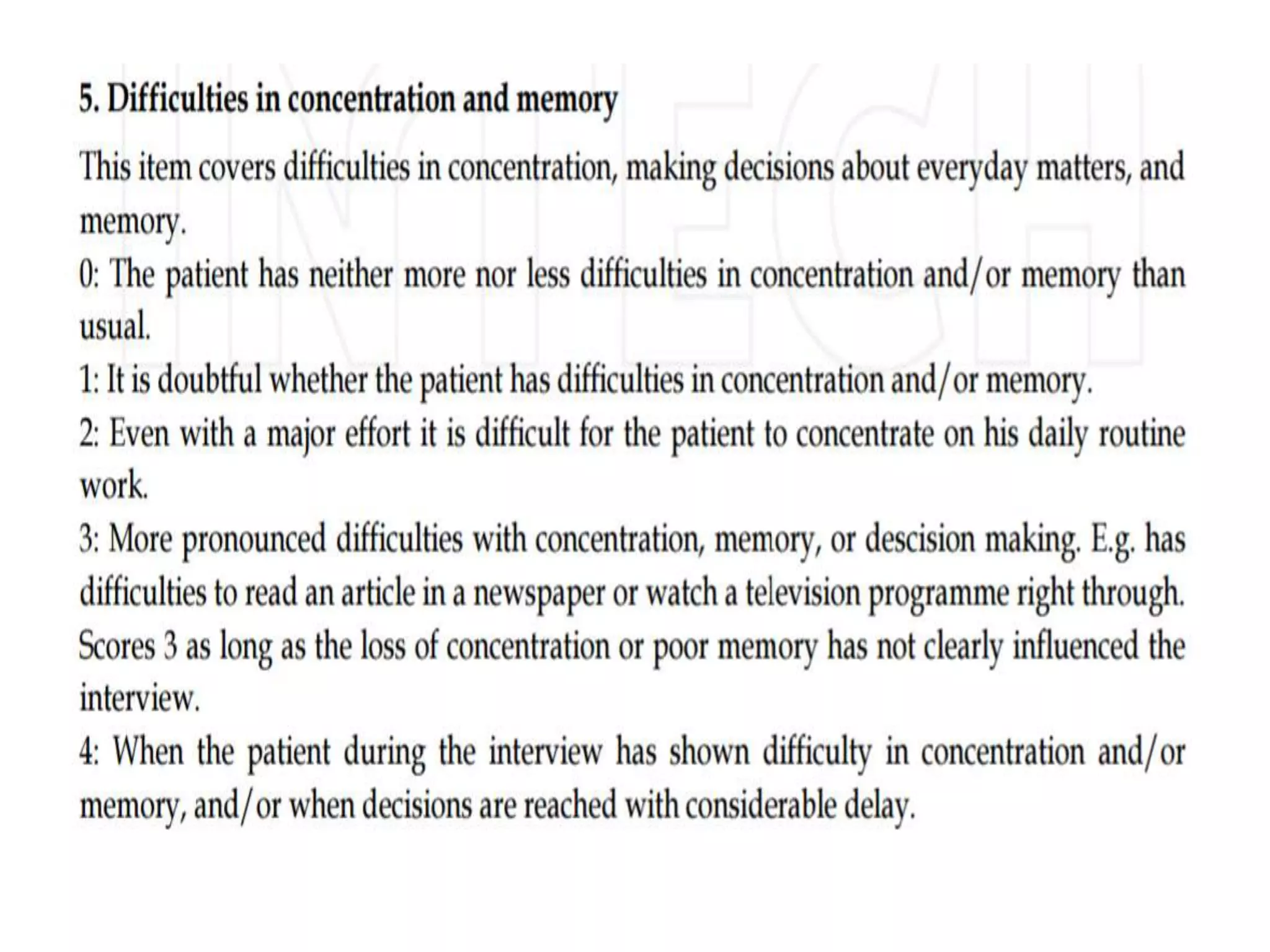
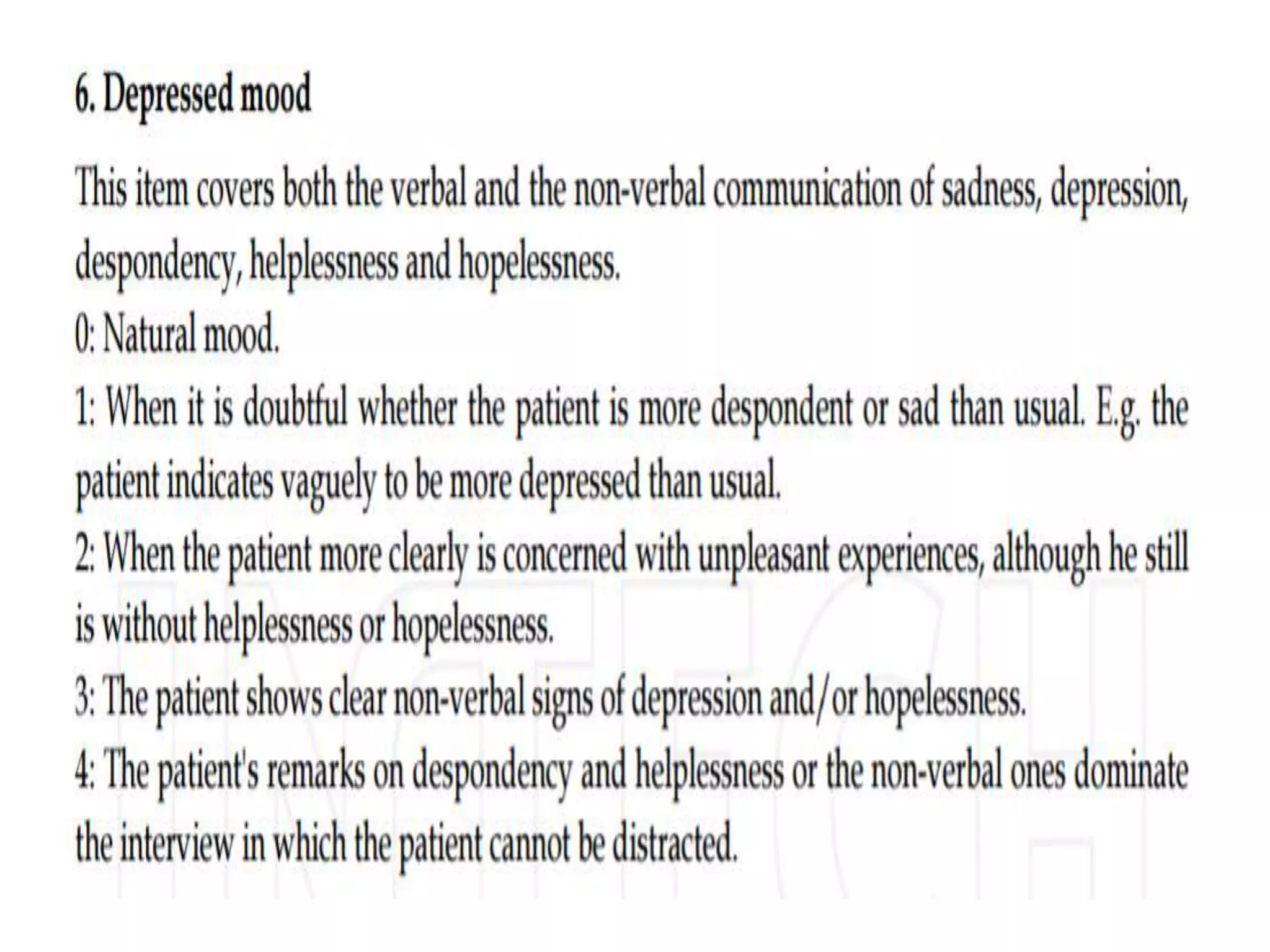
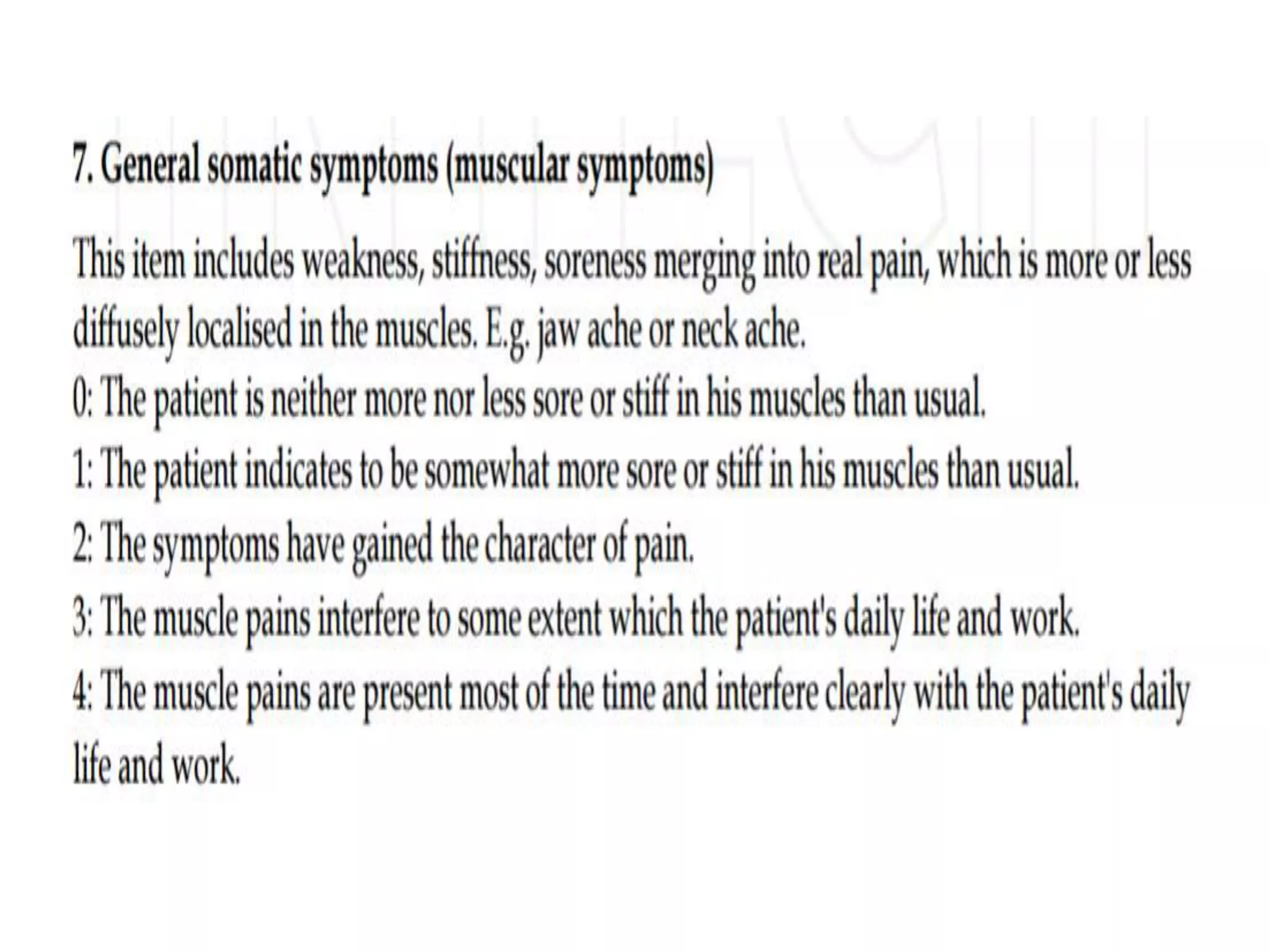
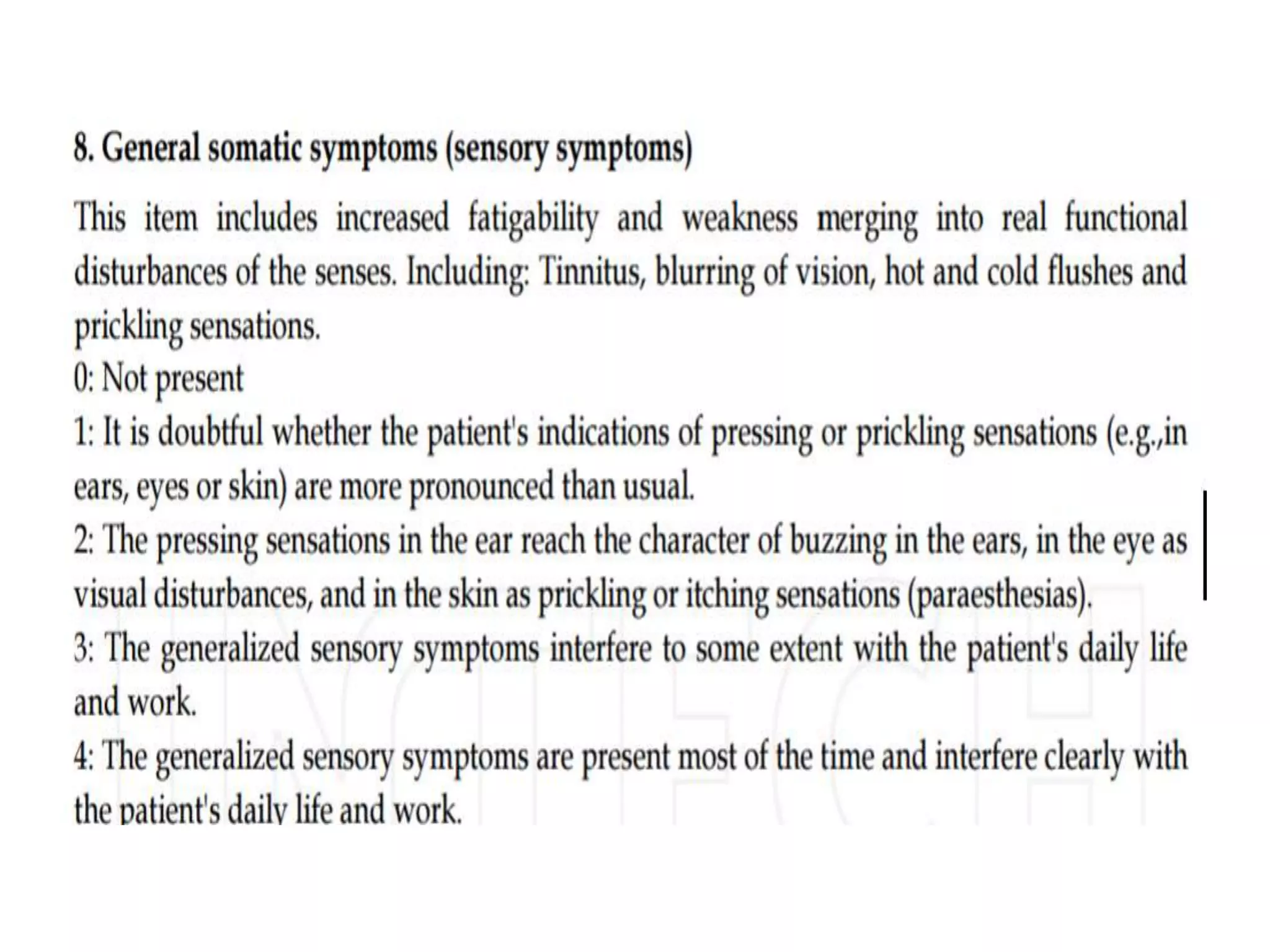
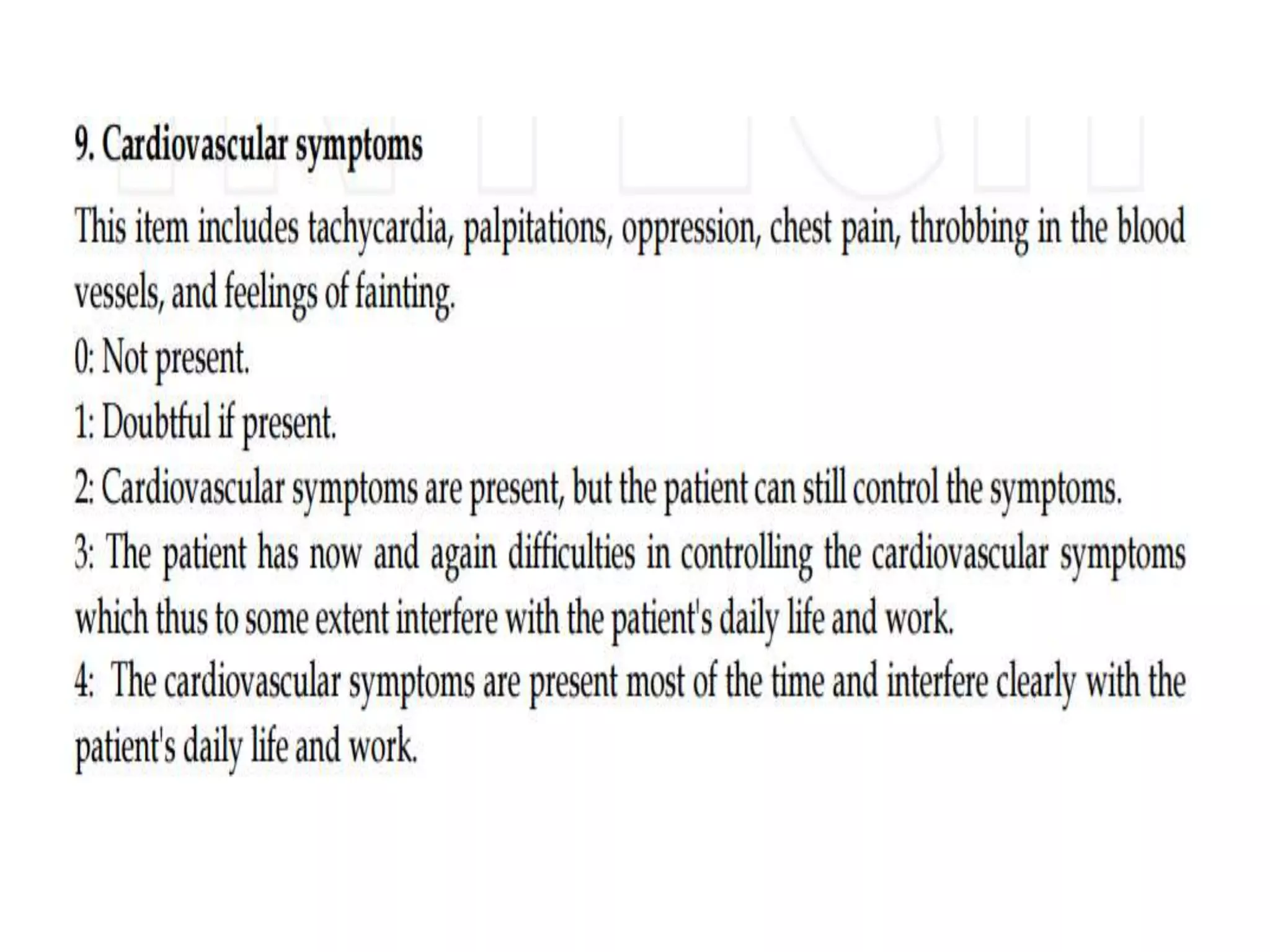
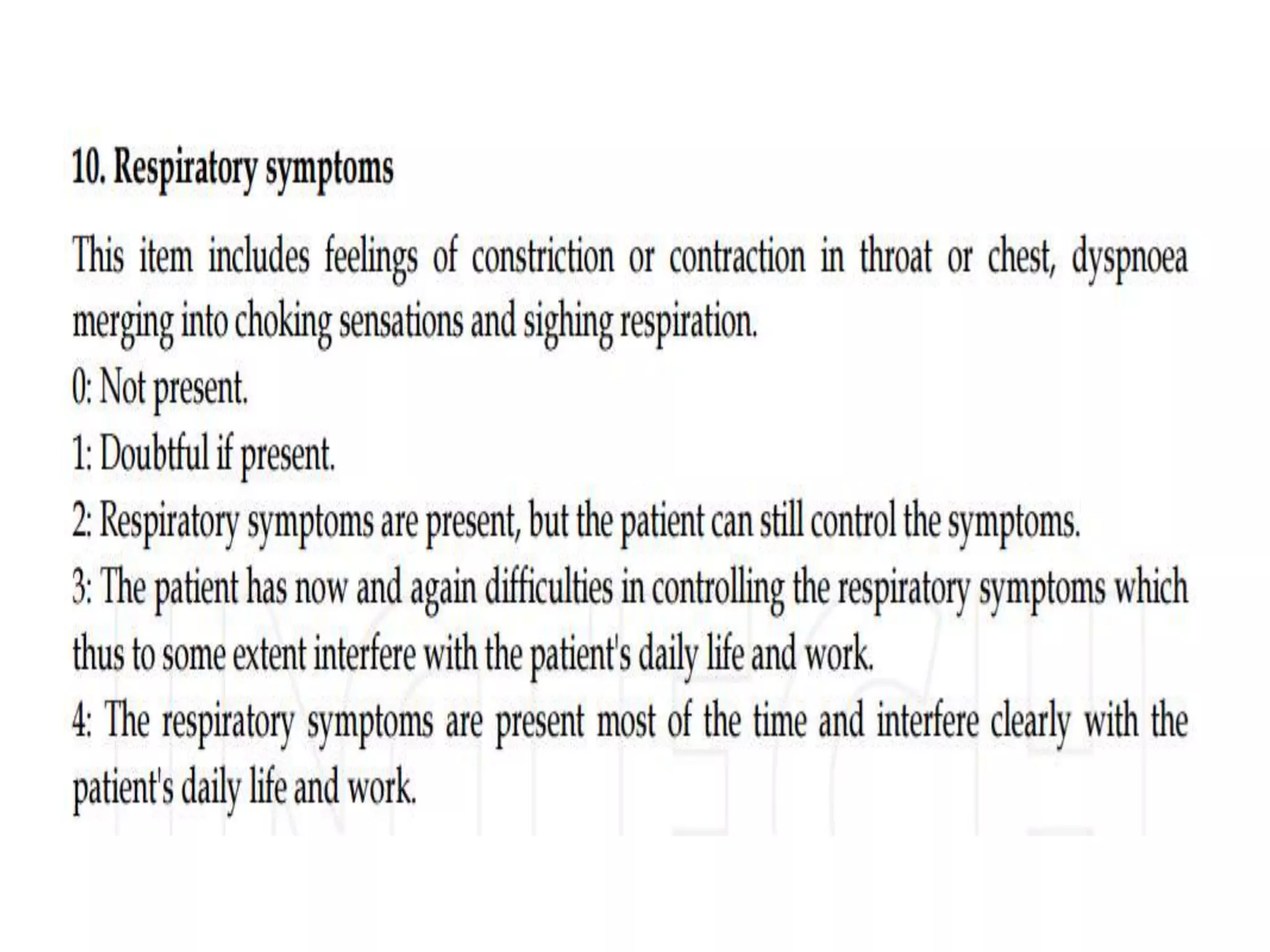
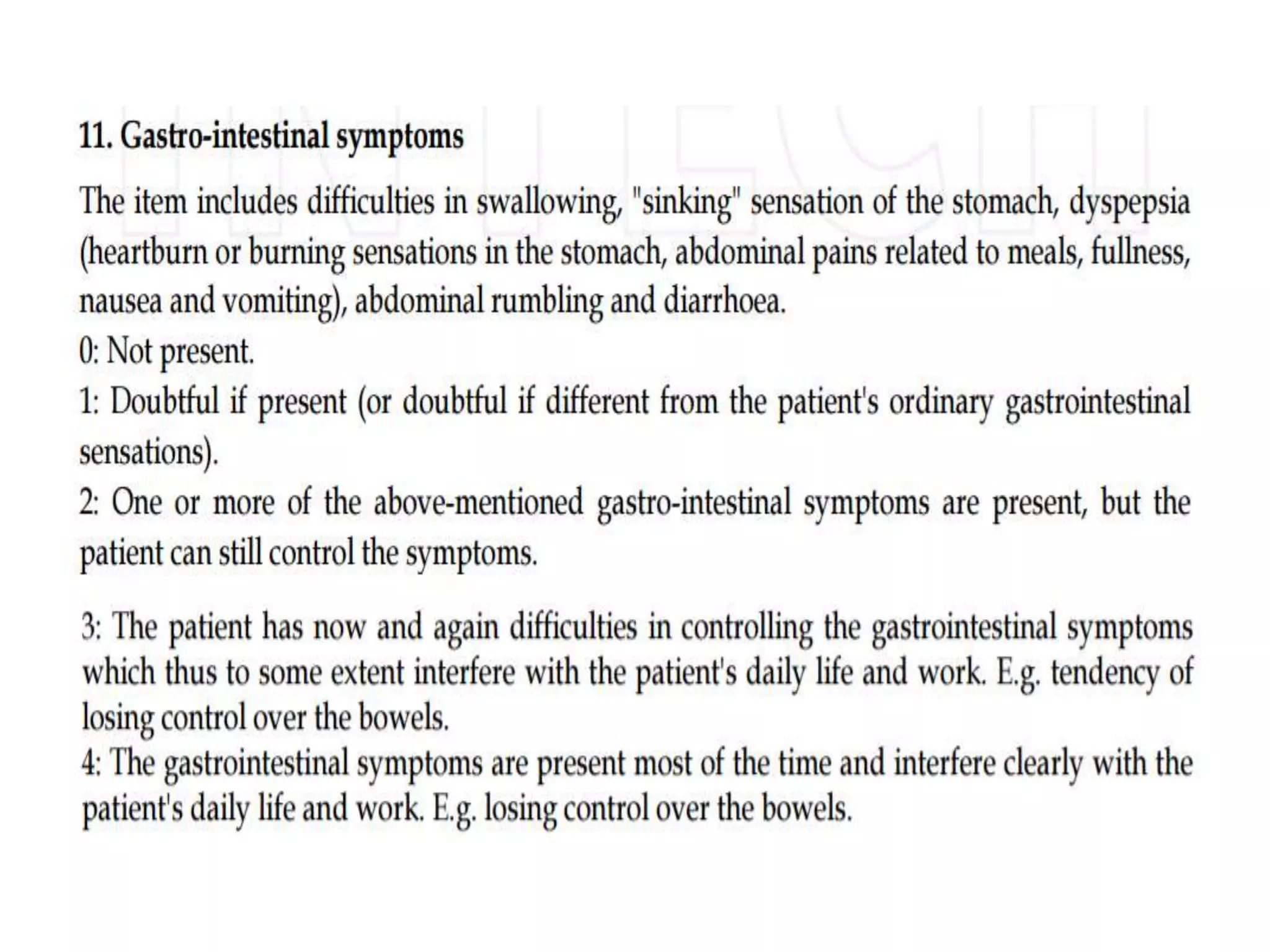
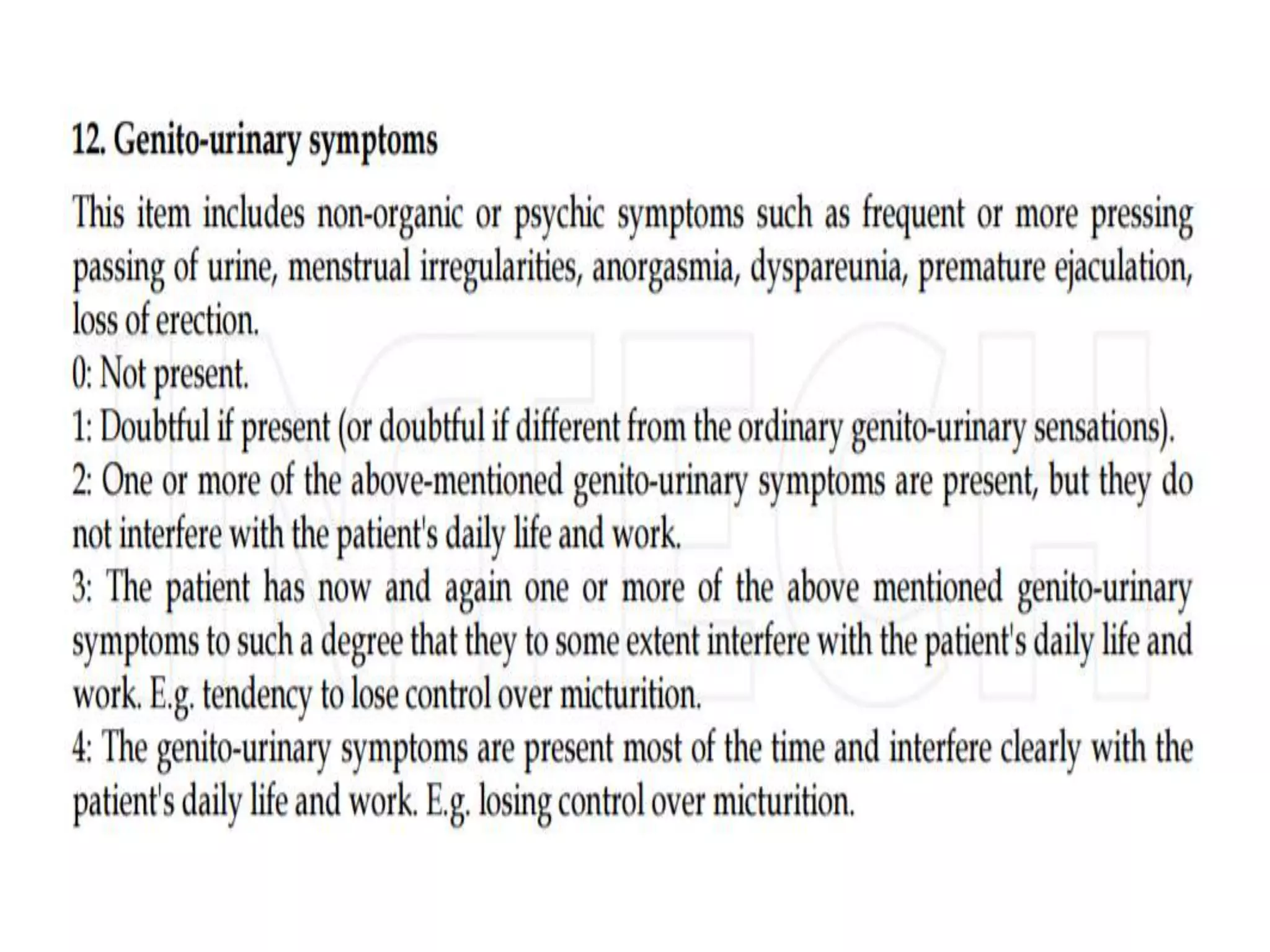
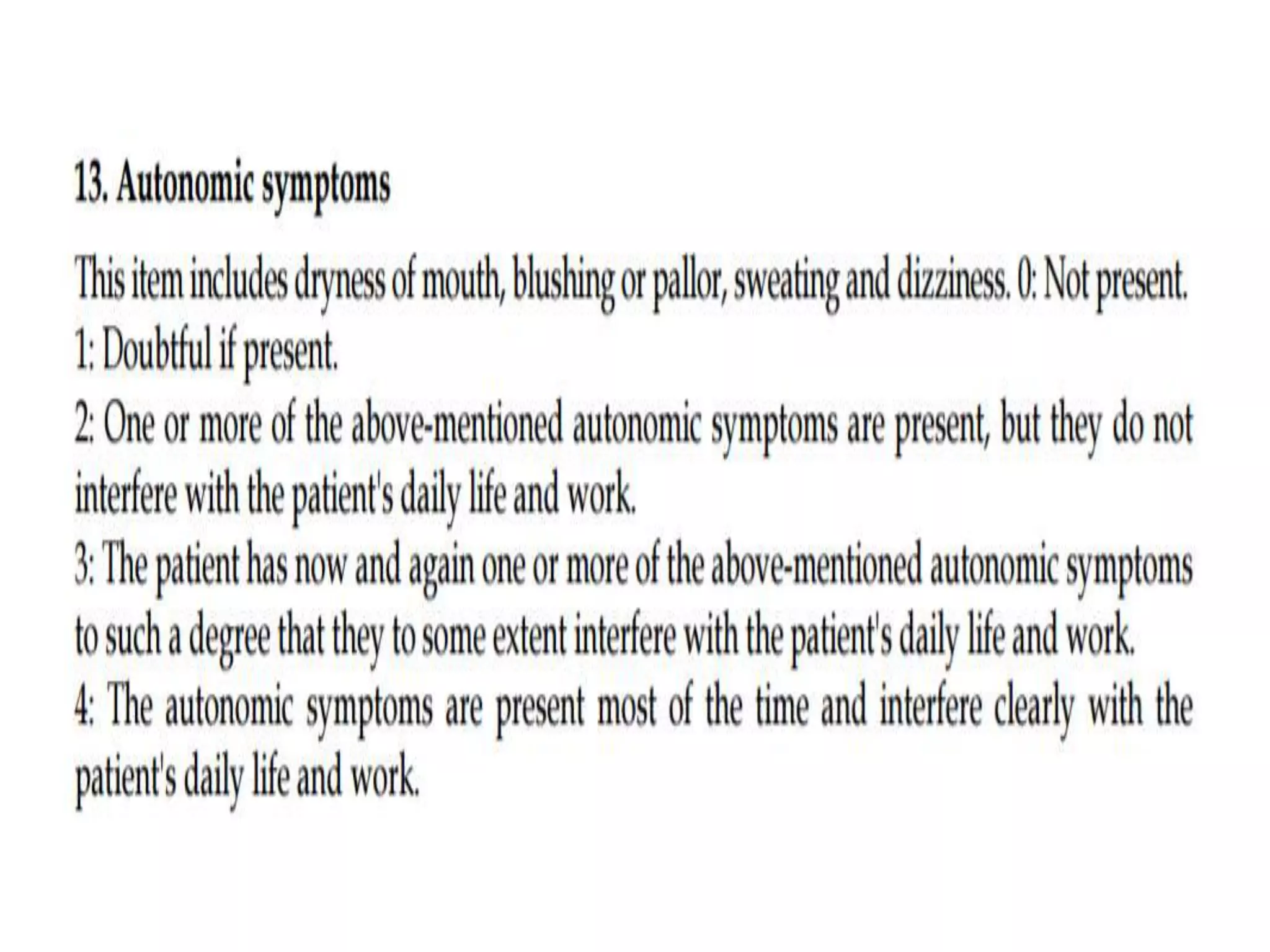
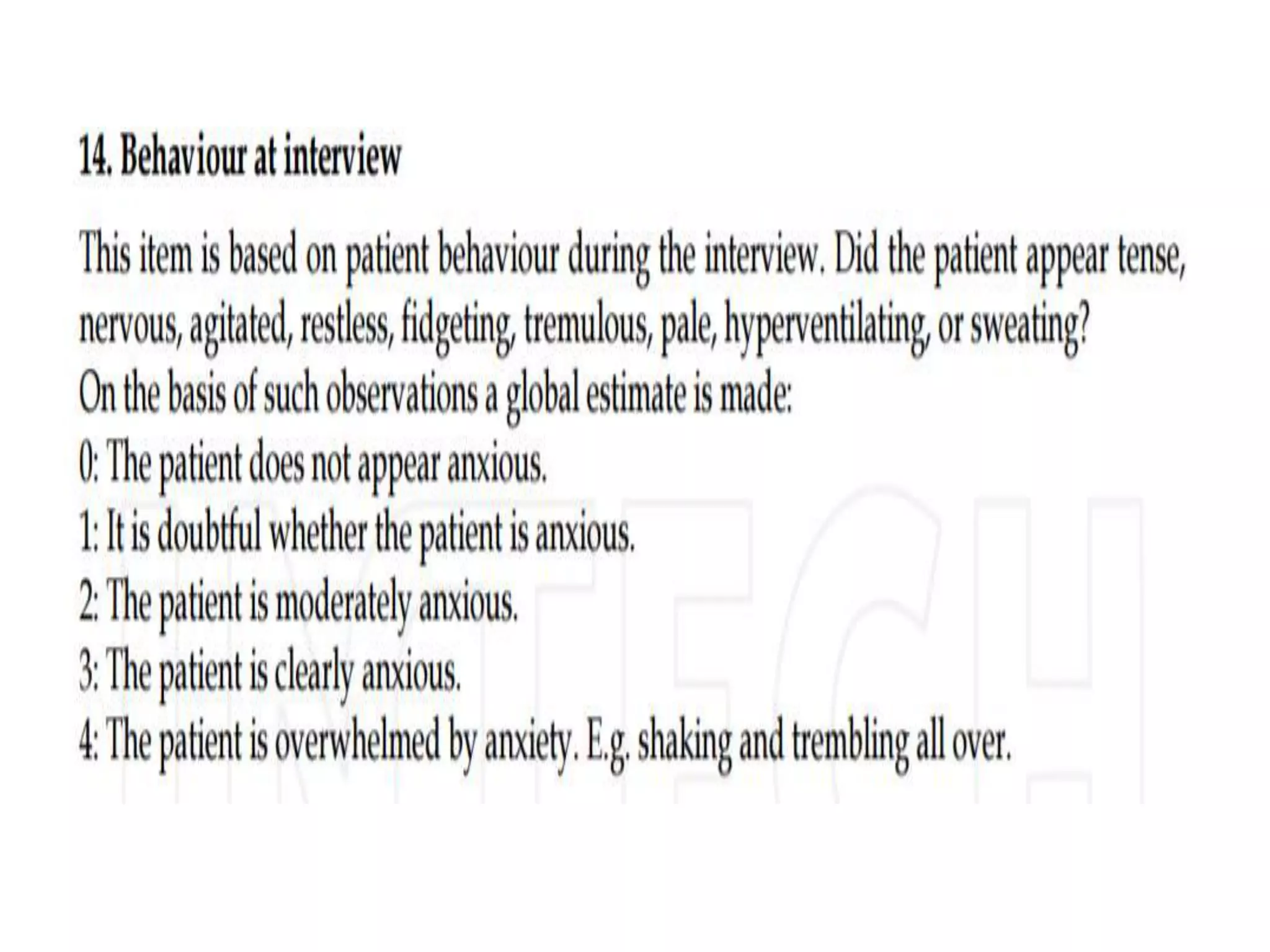
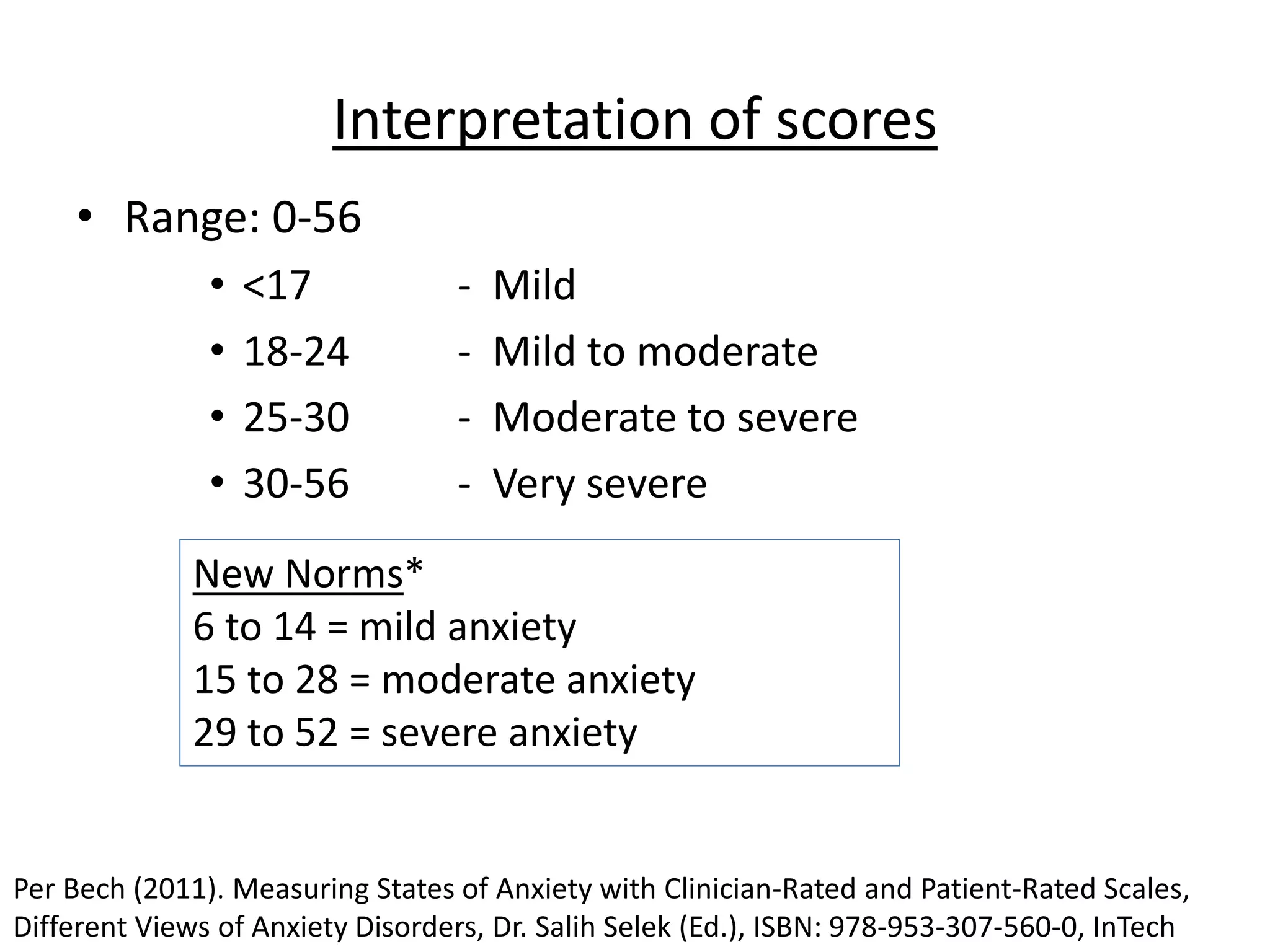
1. The Hamilton Anxiety Rating Scale (HAM-A) is a 14-item clinician-rated scale that assesses both psychic (mental) and somatic (physical) symptoms of anxiety. It has good reliability and validity. Scores below 17 indicate mild anxiety.
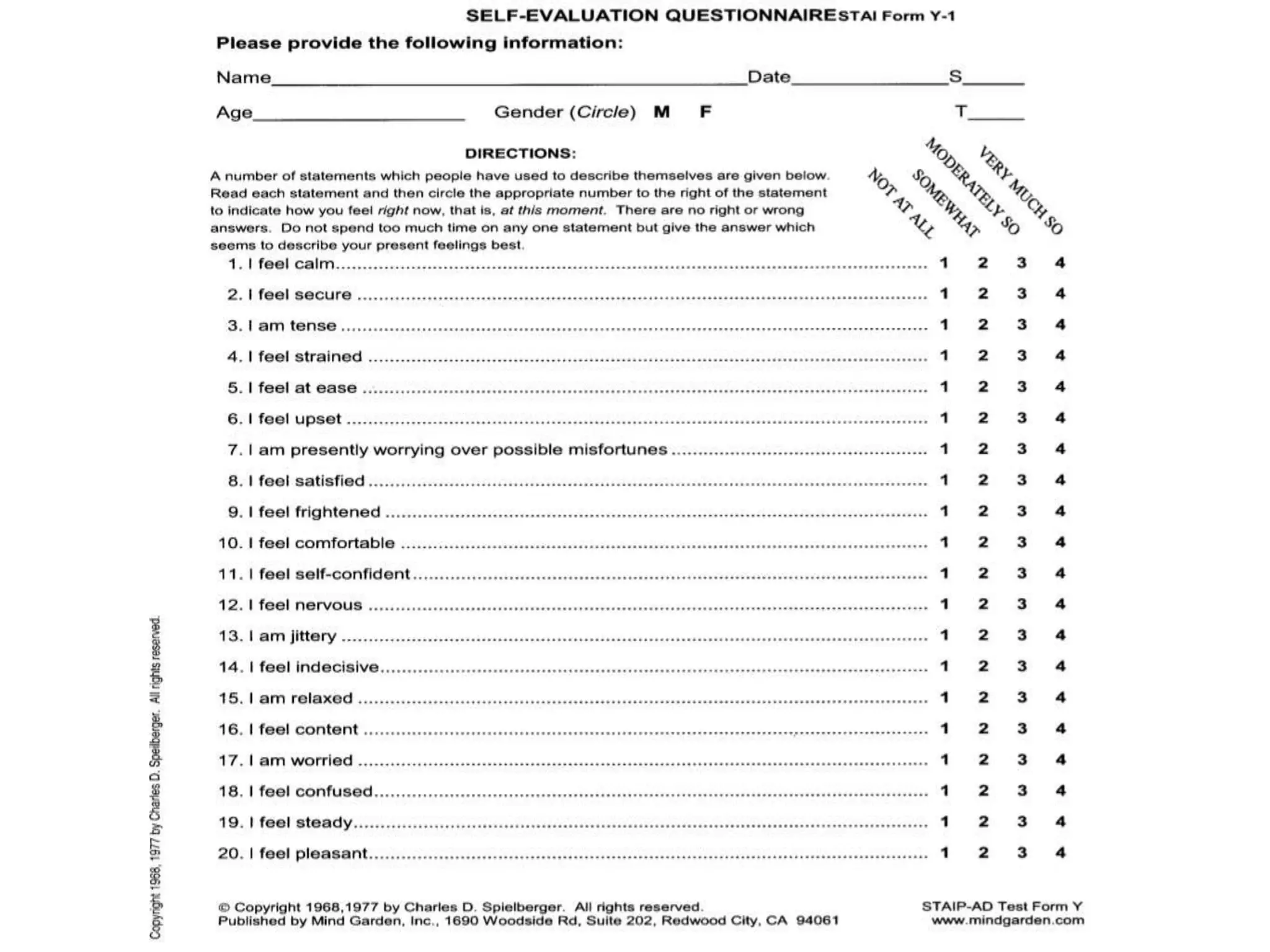
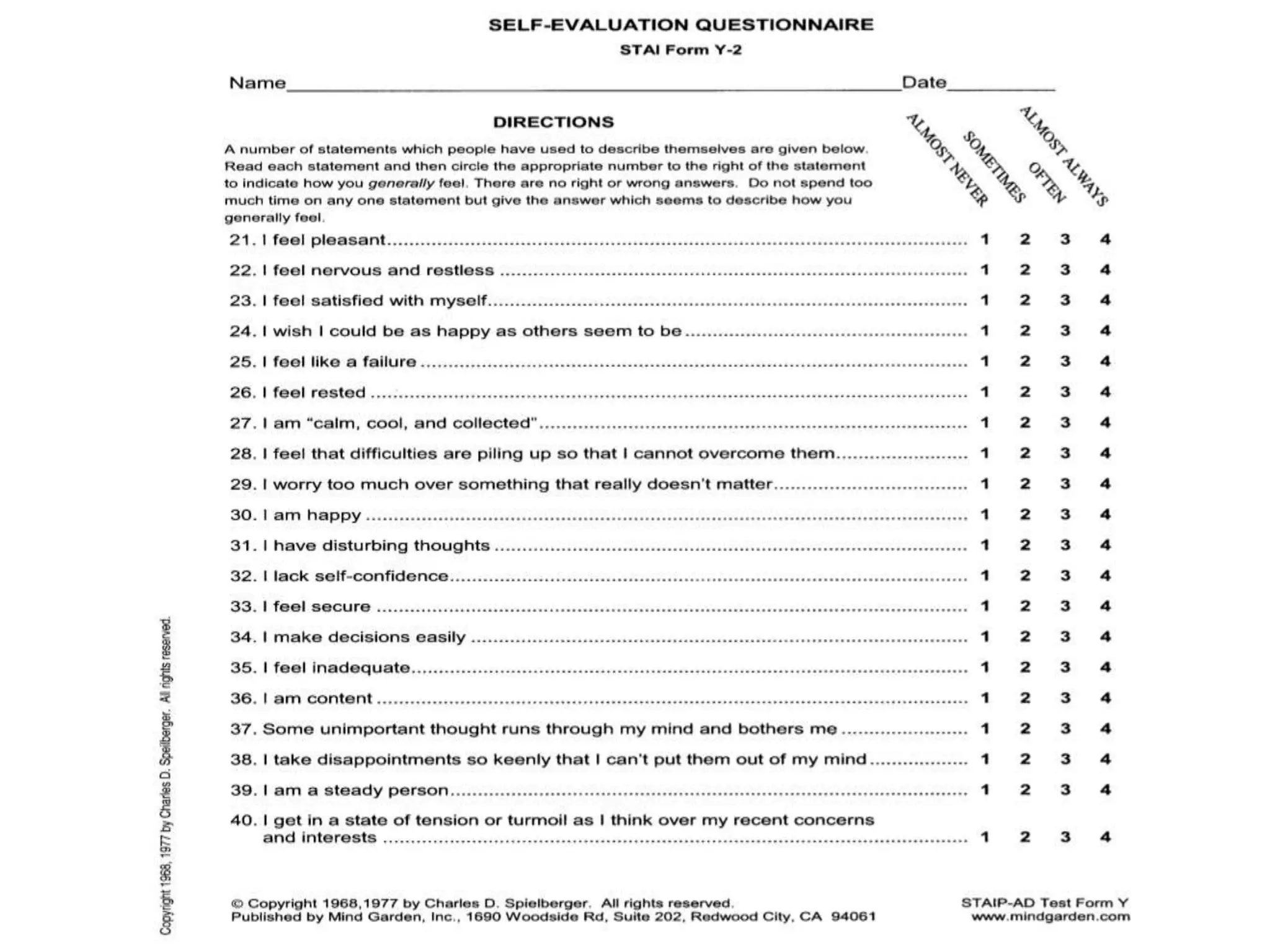
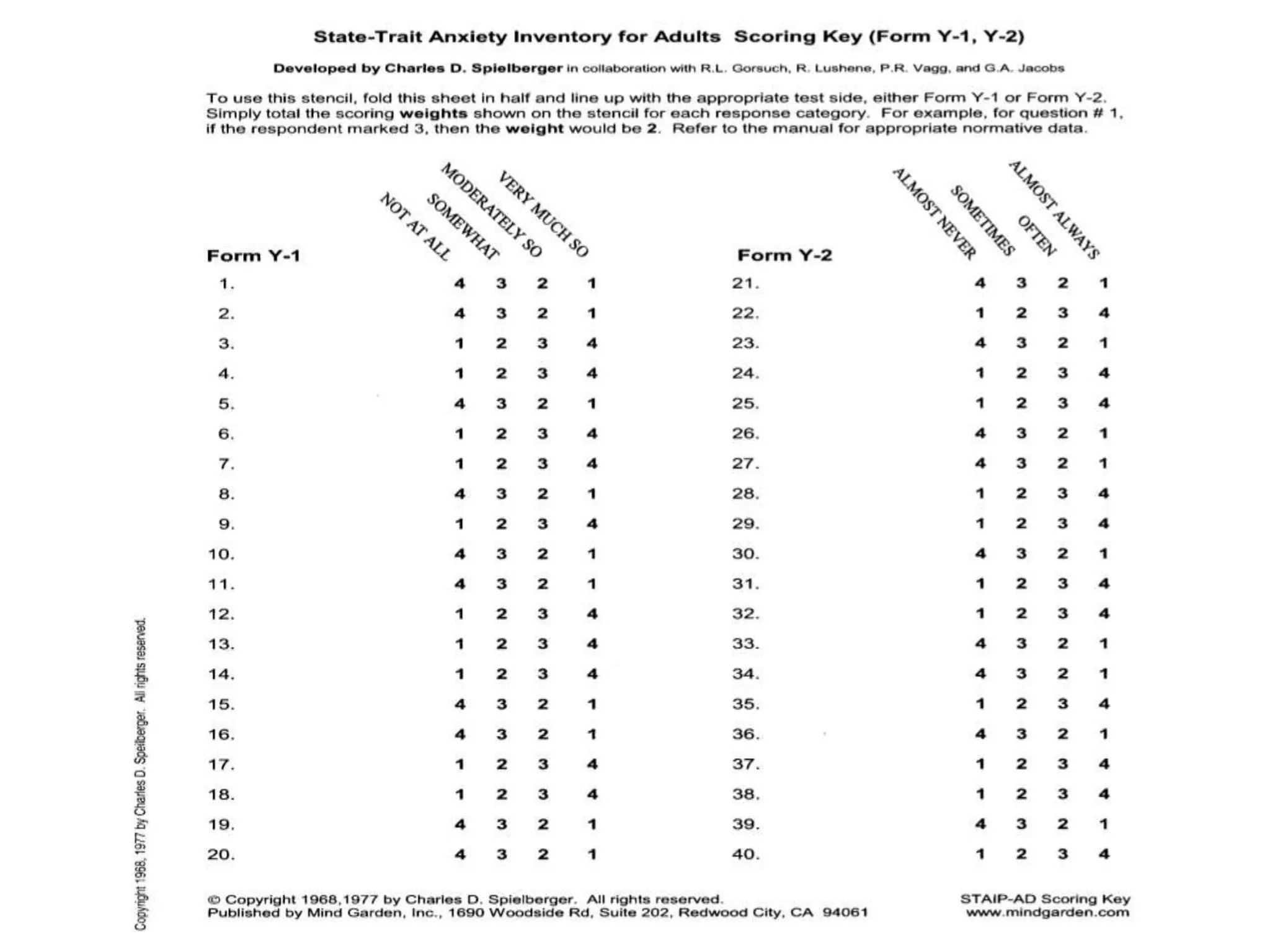
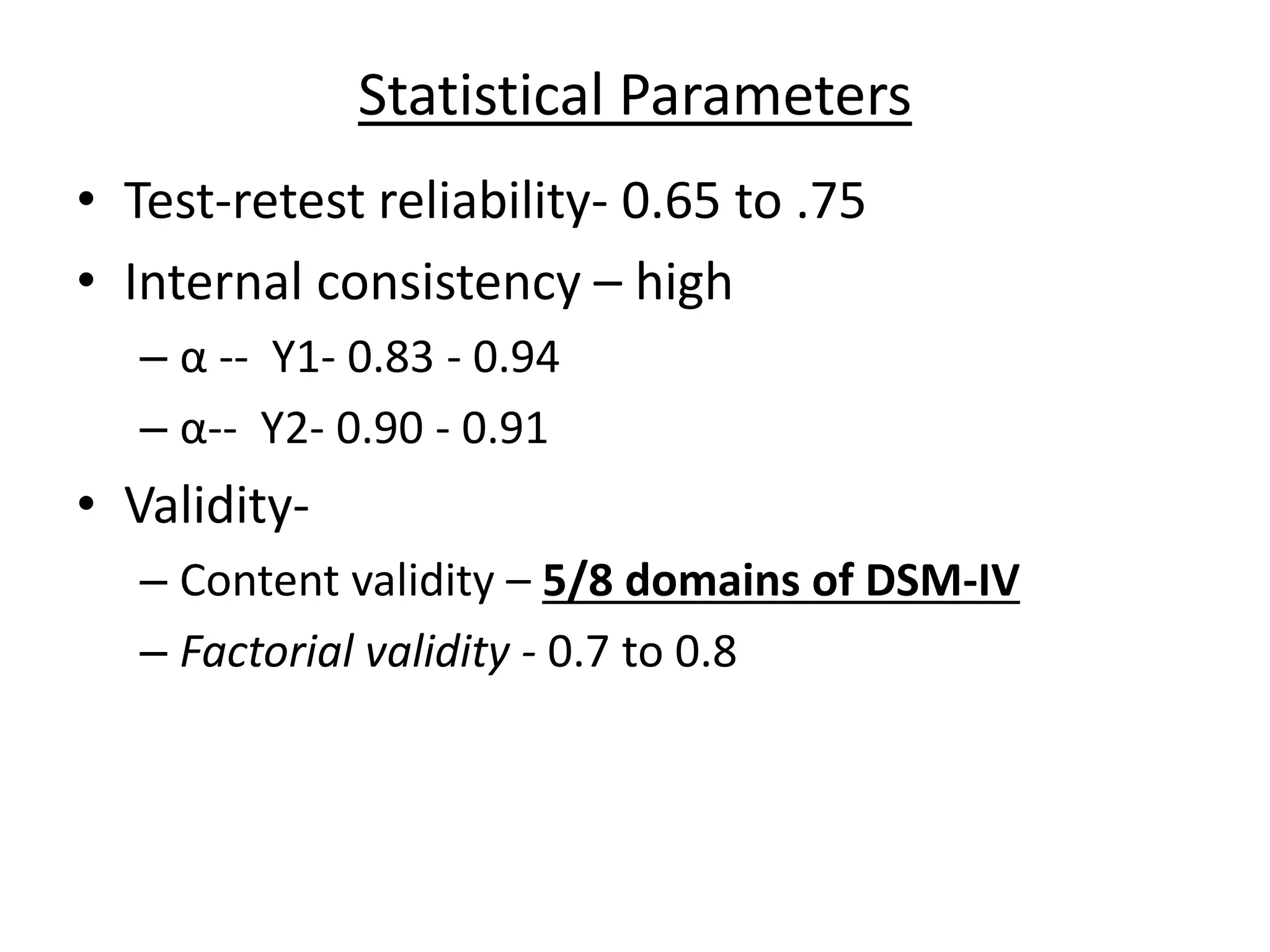
2. The State-Trait Anxiety Inventory (STAI) contains 40 self-report items divided into state and trait anxiety subscales. It can differentiate anxiety from depression and has high reliability. Cut-off scores indicate clinical levels of anxiety.
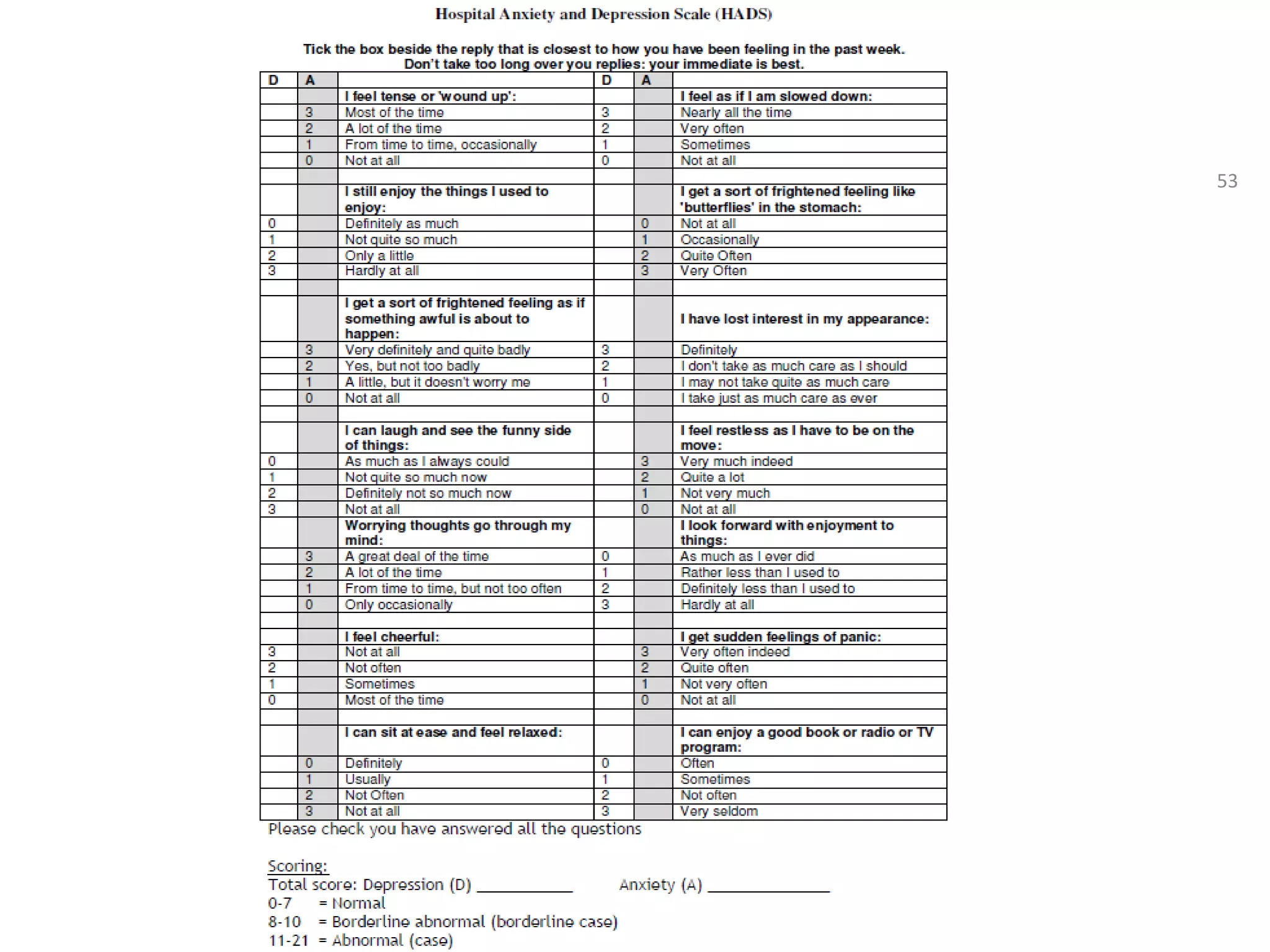
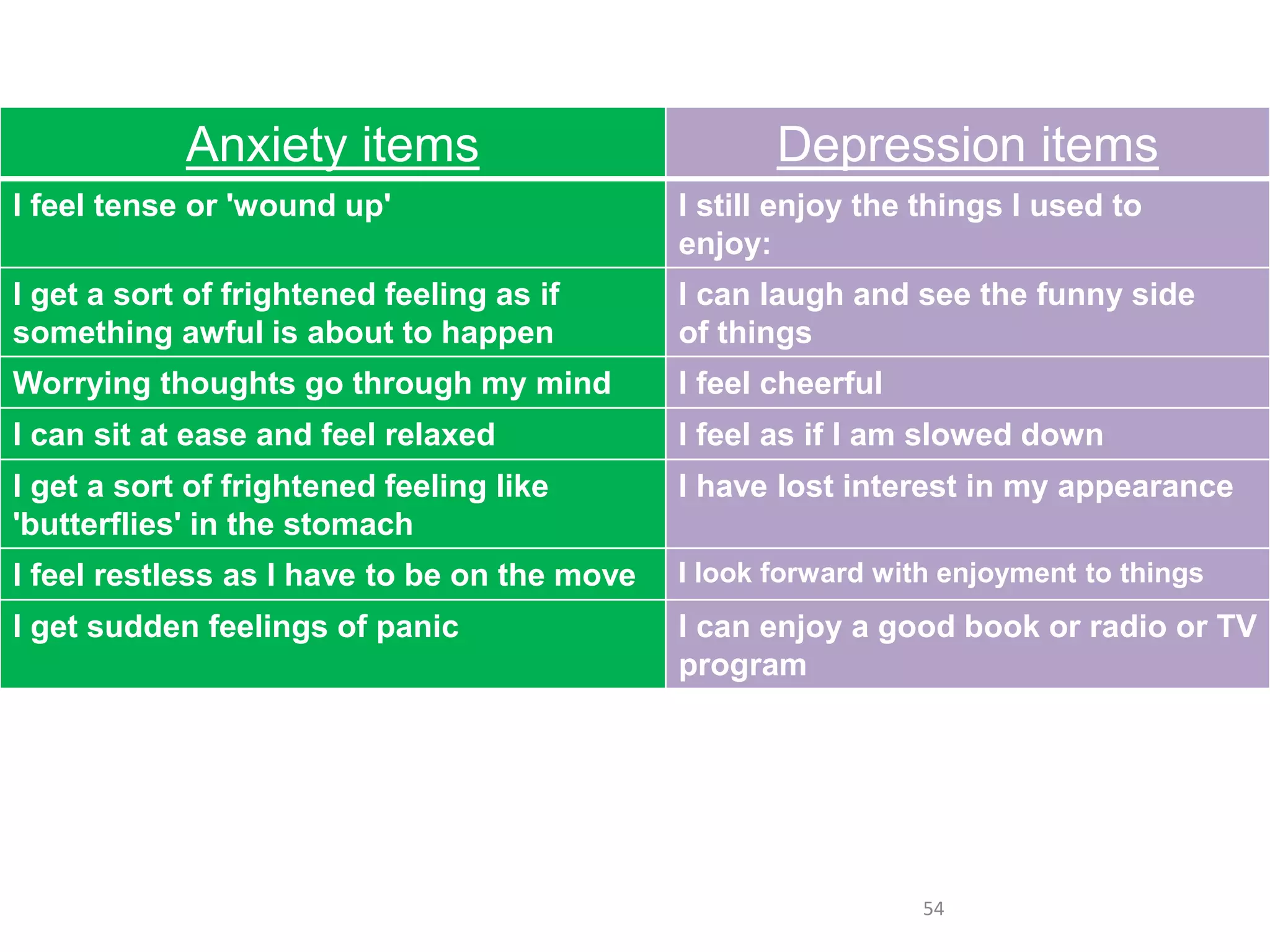
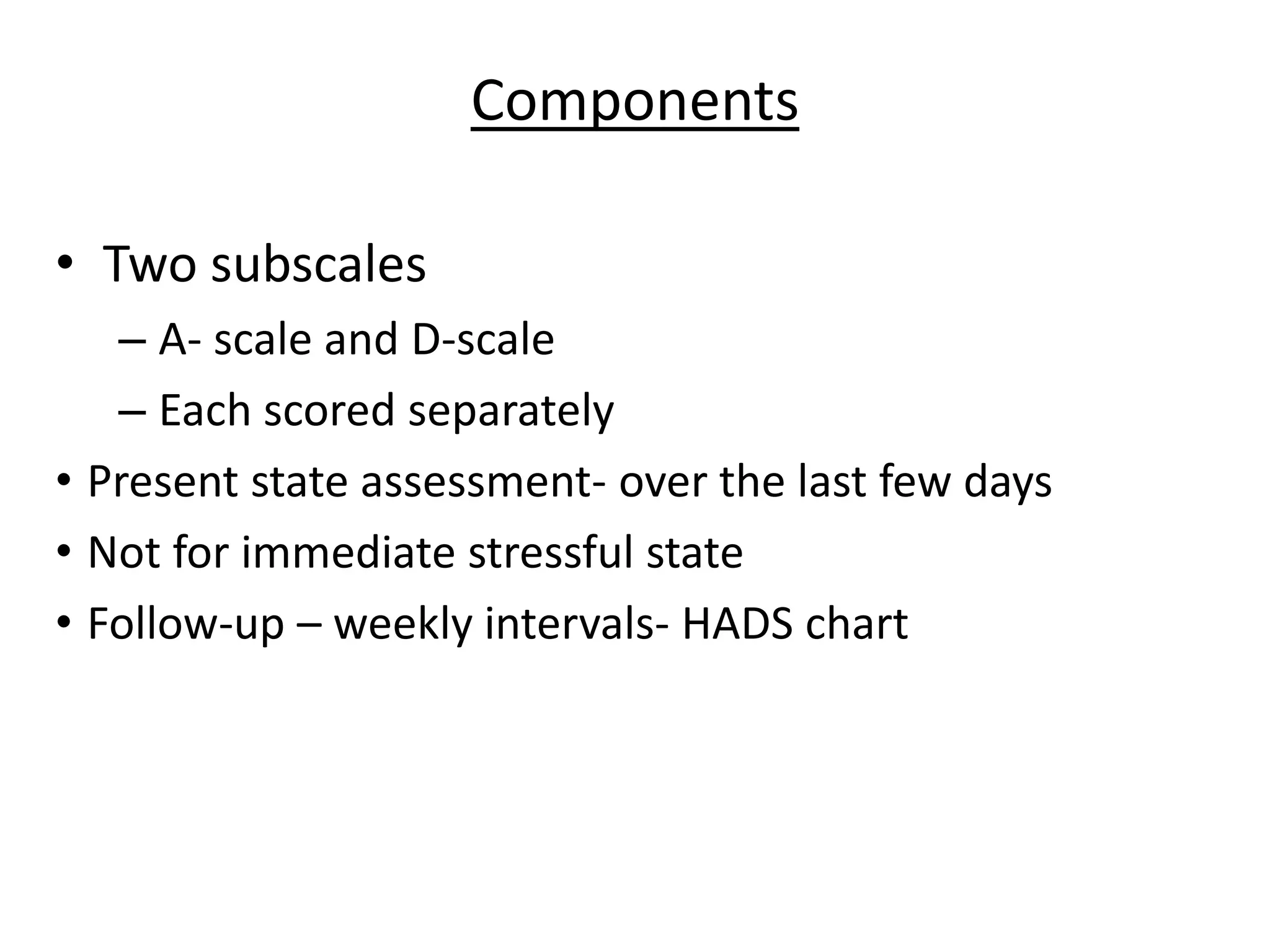
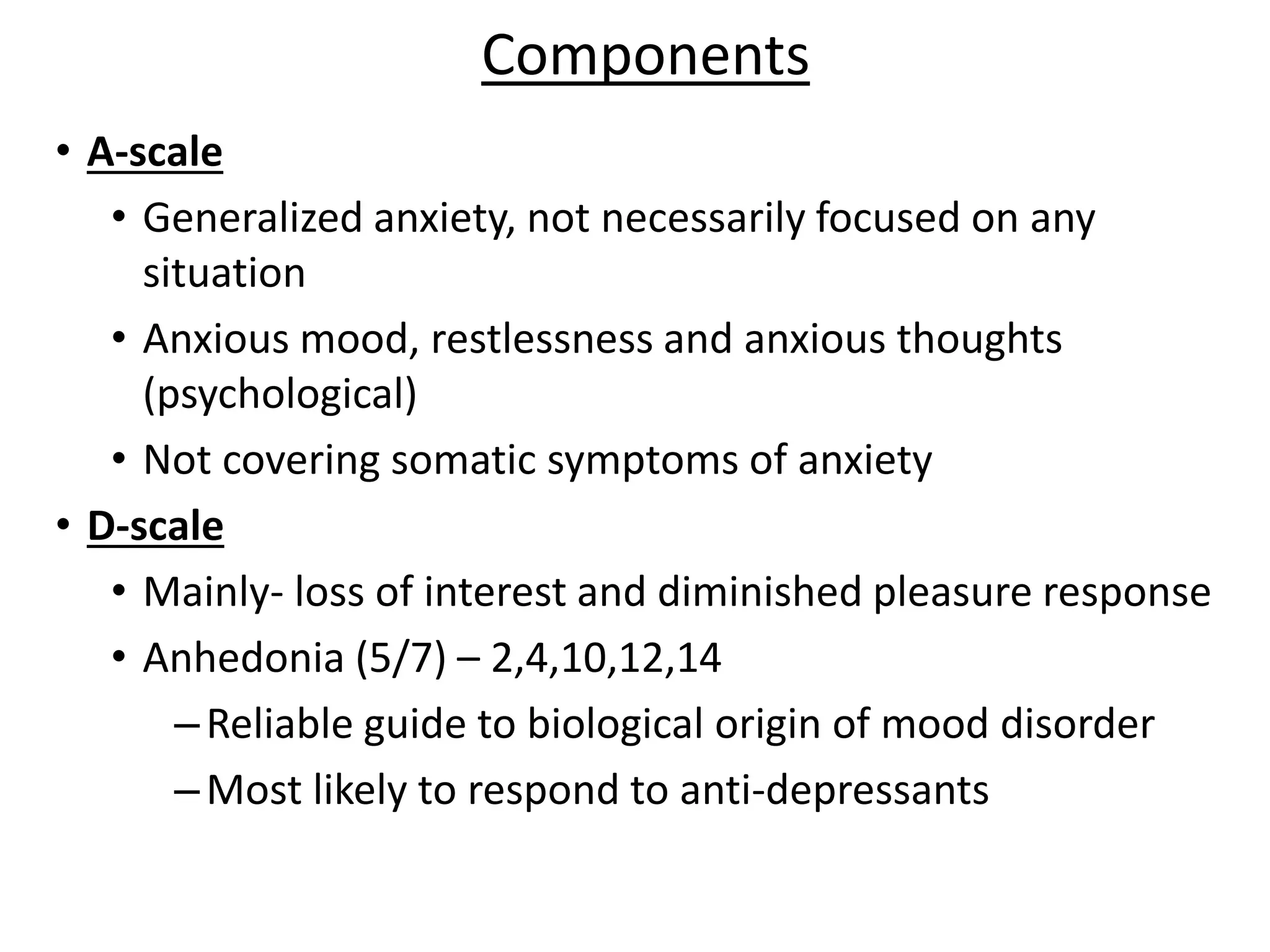
3. The Hospital Anxiety and Depression Scale (HADS) is a 14-item self-report scale with anxiety and depression subscales

![Psychodiagnostic technique[1]](https://cdn.slidesharecdn.com/ss_thumbnails/psychodiagnostictechnique1-191031121907-thumbnail.jpg?width=640&height=640&fit=bounds)


![Rorschach psychodignostics[1]](https://cdn.slidesharecdn.com/ss_thumbnails/rorschachpsychodignostics1-191030073734-thumbnail.jpg?width=640&height=640&fit=bounds)





































































