
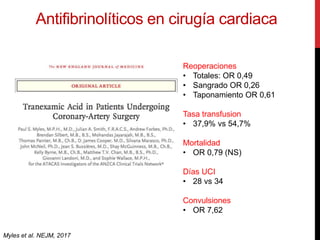
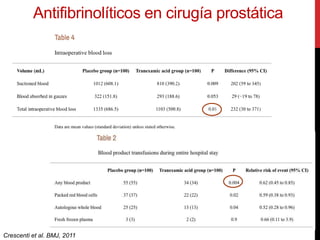
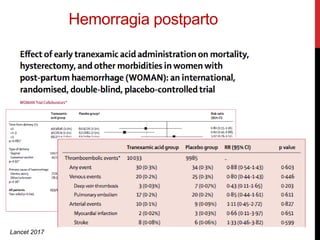
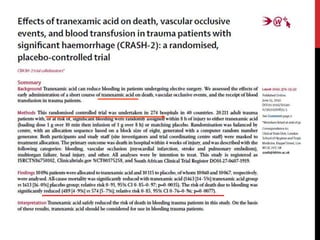
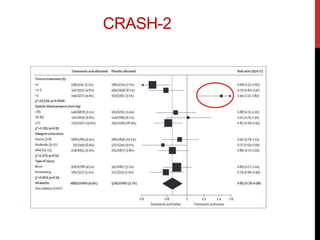
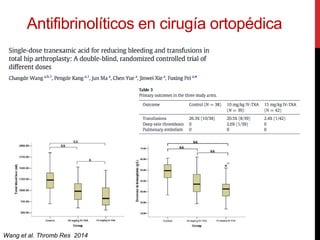
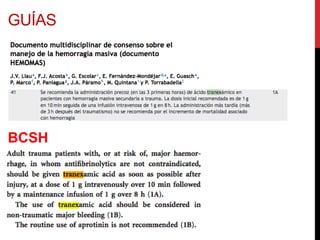
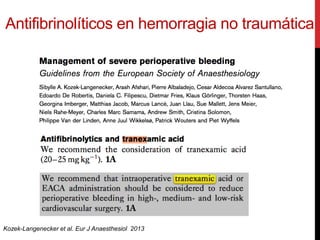
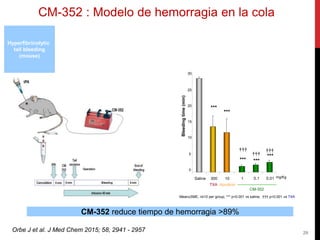
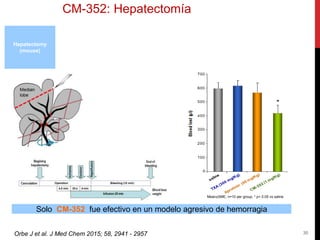

The document discusses pharmacological measures for the conservation of blood products, specifically focusing on antifibrinolytics like tranexamic acid and their efficacy in reducing blood loss during surgeries and trauma. It highlights the potential risks associated with these agents, including severe side effects and the need for safer alternatives in managing significant hemorrhages. Additionally, it introduces a new antifibrinolytic, CM-352, which shows promise in preclinical models for better management of bleeding without impairing hemostasis.




















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


