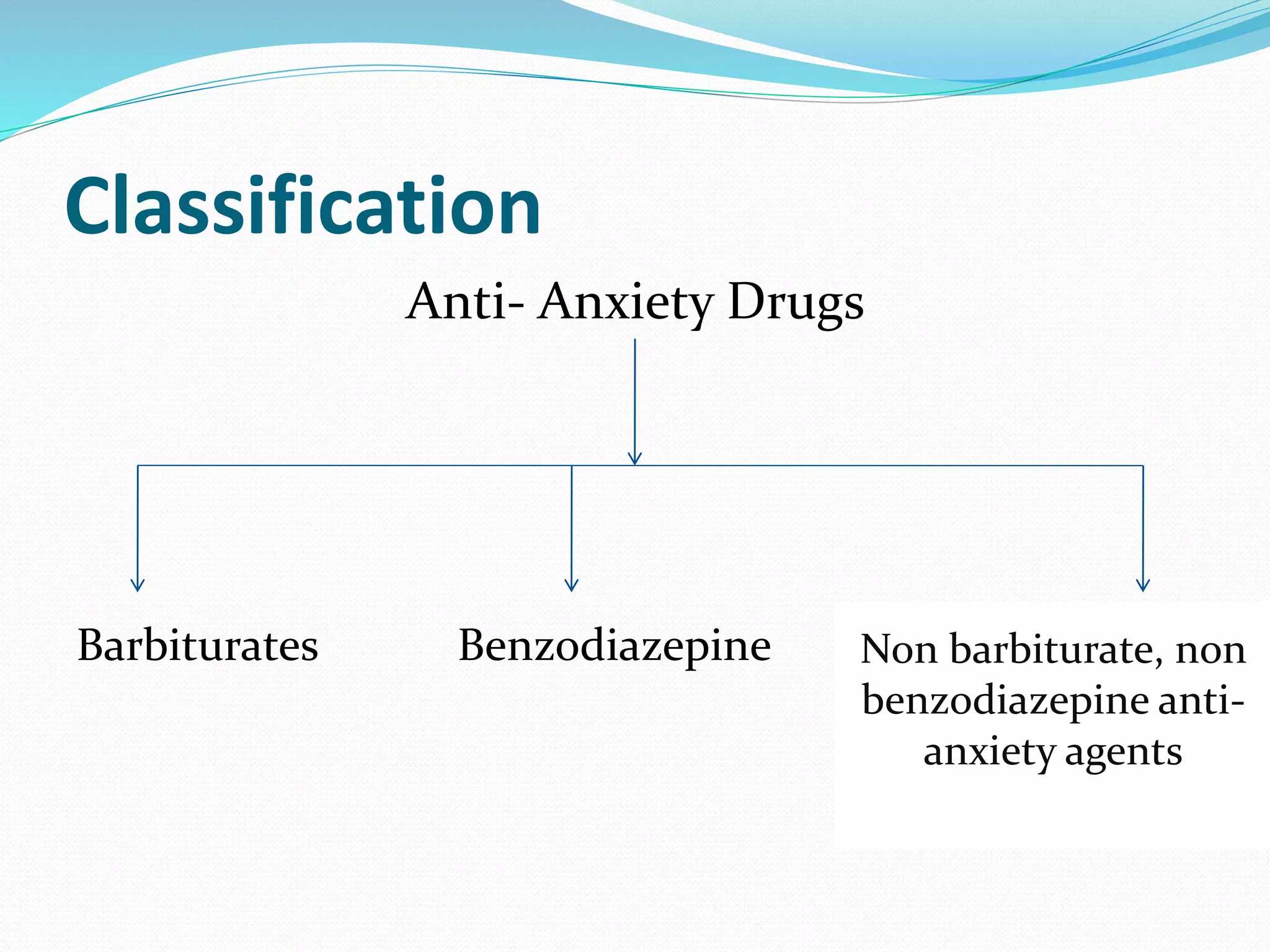
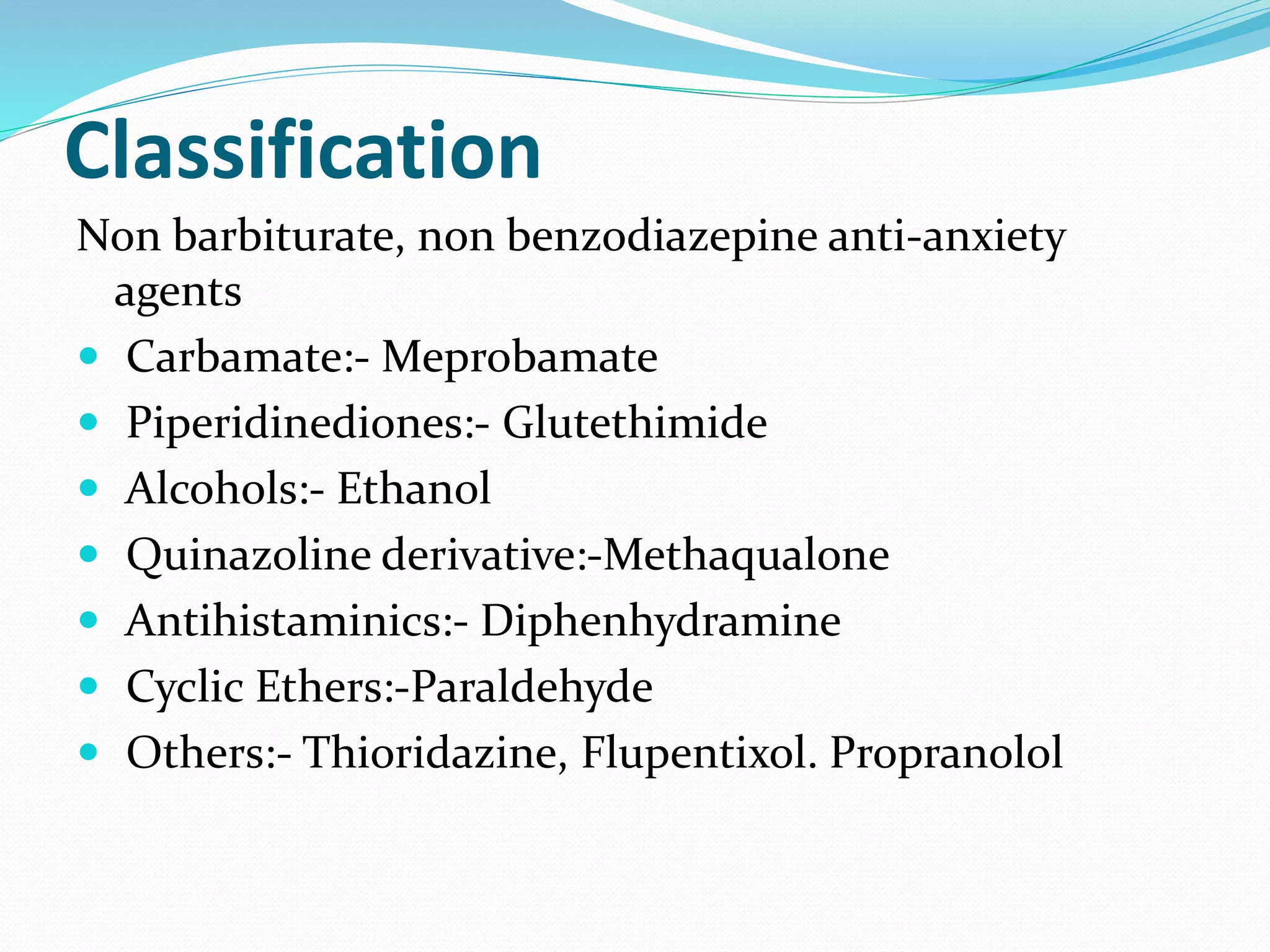
This document discusses anti-anxiety drugs, including their classification, mechanisms of action, indications, and nursing considerations. It describes how anxiety results from an imbalance of chemicals in the brain and how anti-anxiety medications work by potentiating GABA receptors. Major drug classes covered are barbiturates, benzodiazepines, and non-benzodiazepines. Common drugs discussed are diazepam, midazolam, phenobarbital, and choral hydrate. Indications, dosages, routes of administration, side effects, nursing implications, and patient education are summarized for safe and effective use of these medications.