



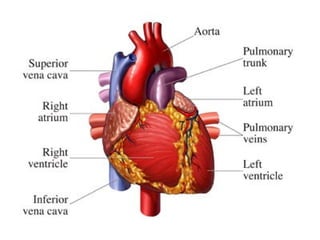

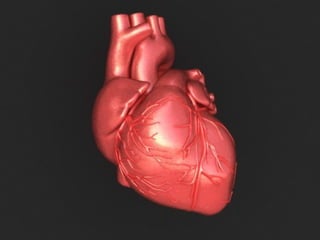
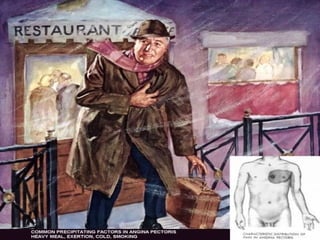






















































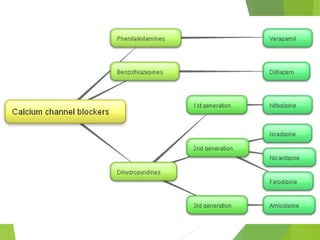















































































































The document provides detailed information about the human heart, including its function, statistics, and various types of angina pectoris. It outlines antianginal drugs, their classifications, mechanisms, and side effects, alongside the roles of other medications in managing heart conditions. It also discusses the importance of gradual withdrawal of certain drugs and implications of combining treatments for effective cardiovascular care.





























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









