Download as PDF, PPTX



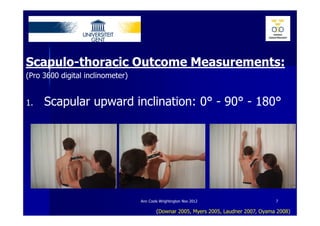
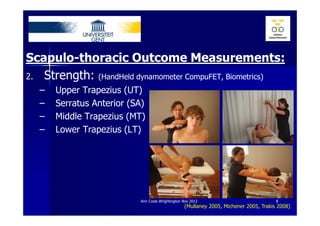
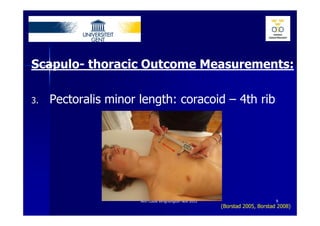
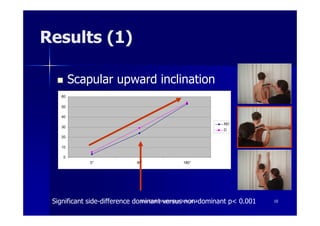
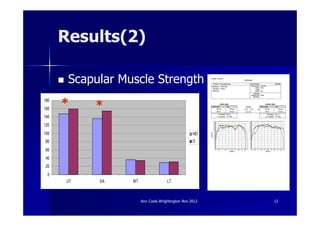
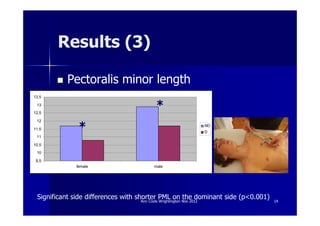

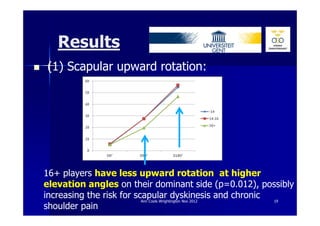

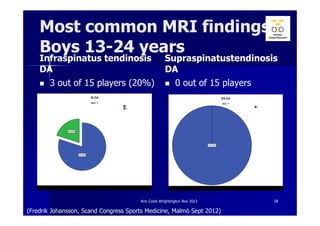
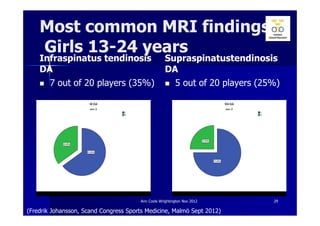
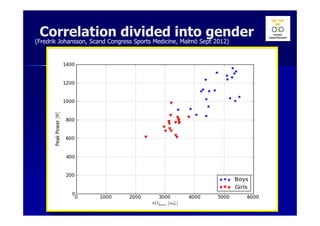
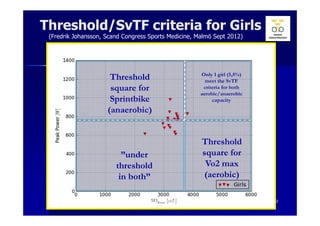
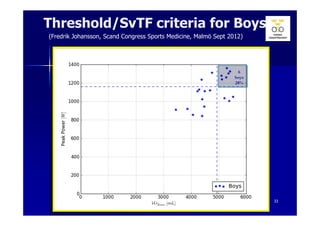
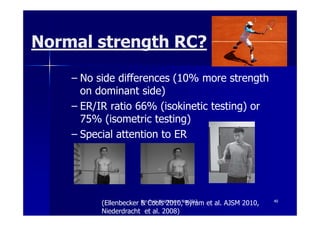
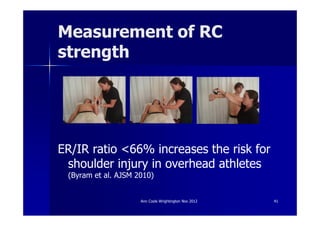
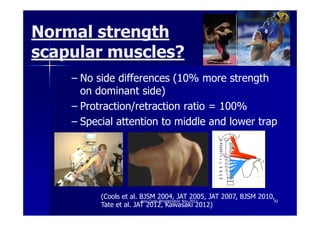
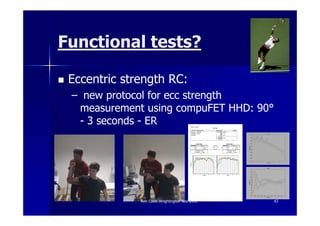



This document discusses screening tests for the shoulder girdle in elite tennis players. It describes studies that examined strength, range of motion, and muscle imbalances in adolescent tennis players in Sweden. The studies found increased upward rotation of the scapula on the dominant side, as well as strength imbalances between dominant and non-dominant sides. MRI screening of elite players found high rates of tendinosis, especially in the infraspinatus and supraspinatus tendons. The implications are that screening can help identify risk factors for injury and guide return-to-play criteria focusing on normal strength, range of motion, and function.
![Ann cools 2 internal impingement [compatibiliteitsmodus]](https://cdn.slidesharecdn.com/ss_thumbnails/anncools2internalimpingementcompatibiliteitsmodus-121207052327-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Ann cools 1 clinical exam [compatibiliteitsmodus]](https://cdn.slidesharecdn.com/ss_thumbnails/anncools1clinicalexamcompatibiliteitsmodus-121207051539-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)