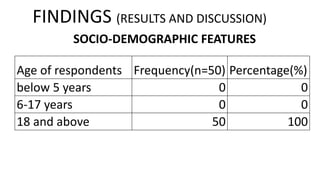
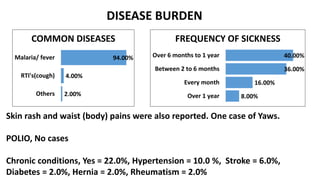
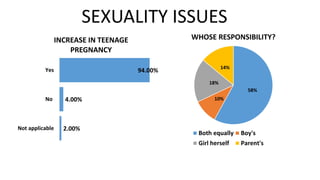
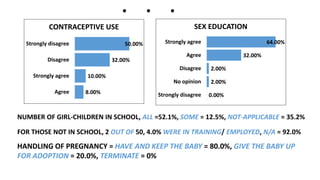
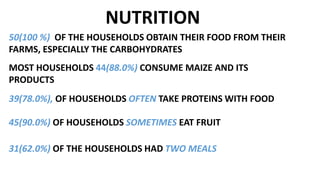
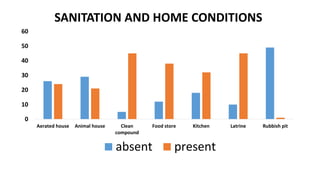
This document summarizes the results of a community diagnosis conducted in the Ankyease community in Ghana. It provides definitions of key terms and outlines the study objectives, methodology, and findings. The study assessed the socio-demographic characteristics, health status, sanitation, nutrition, and health-seeking behaviors of 50 households. Key findings included a high prevalence of malaria, teenage pregnancy, and lack of access to health facilities. The summary concludes with recommendations to improve sex education, sanitation, nutrition, and access to schools and health centers.



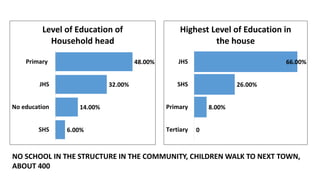
























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











