Downloaded 17 times
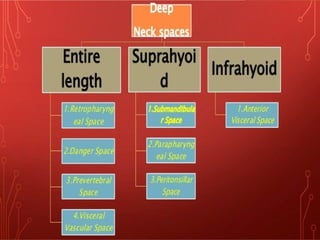
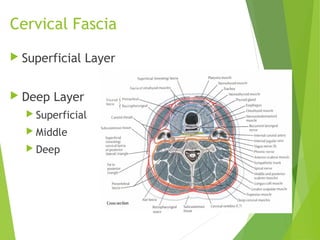
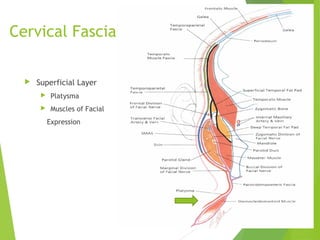
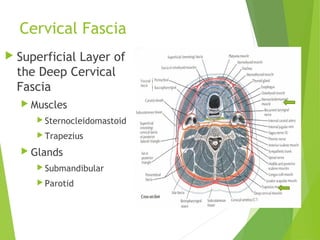
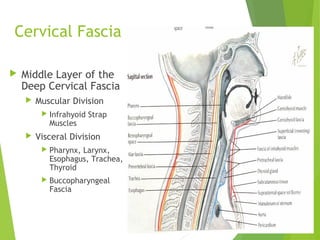
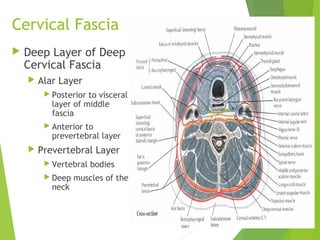
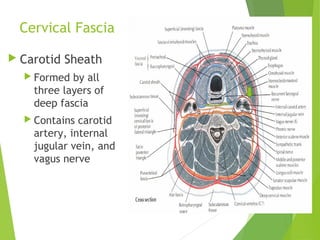
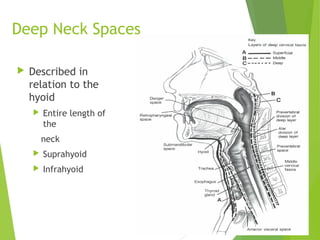
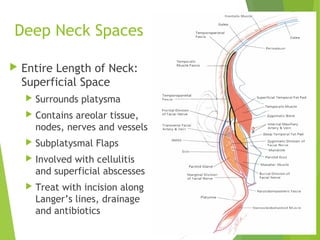
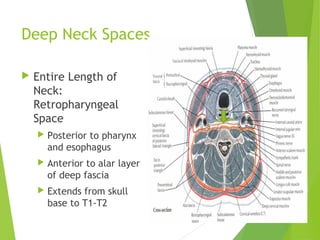
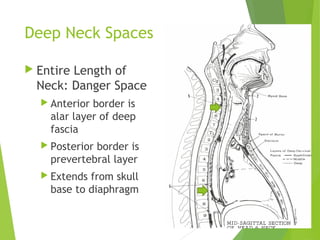
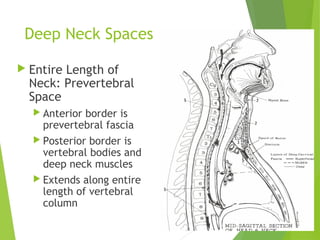
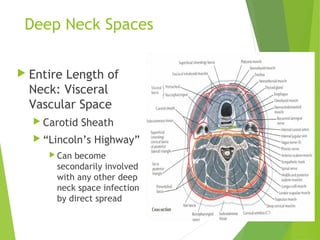
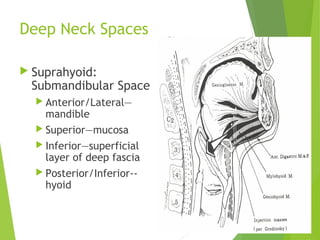
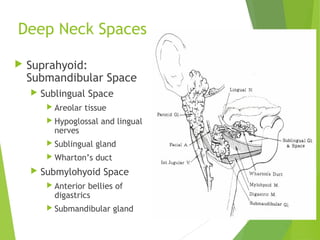
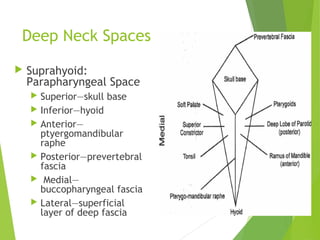
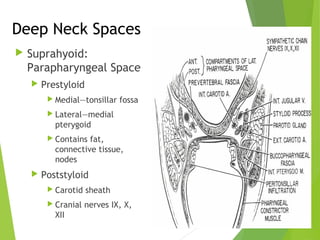
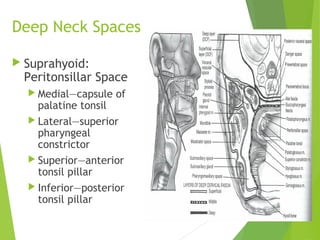
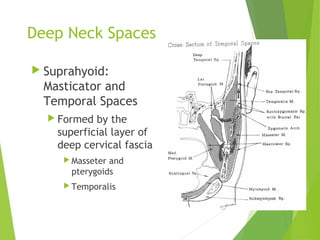
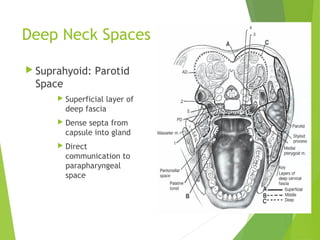
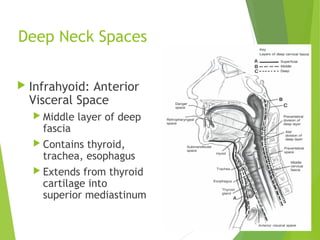







The document discusses the anatomy and clinical considerations of deep neck spaces and cervical fascia, detailing their layers and the structures they contain. It covers potential infections in these areas, their presentations, imaging techniques for diagnosis, treatment strategies, and possible complications associated with deep neck space infections. Key focus is given to distinctions between various spaces, such as retropharyngeal, prevertebral, and parapharyngeal spaces, including treatment protocols and complications that may arise.









































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















