Deep neck spaces are anatomical compartments in the neck, defined by the deep cervical fascia, that play a crucial role in understanding various pathologies, particularly infections.
Similar to Deep neck spaces are anatomical compartments in the neck, defined by the deep cervical fascia, that play a crucial role in understanding various pathologies, particularly infections.
Deep neck spaces are anatomical compartments in the neck, defined by the deep cervical fascia, that play a crucial role in understanding various pathologies, particularly infections.
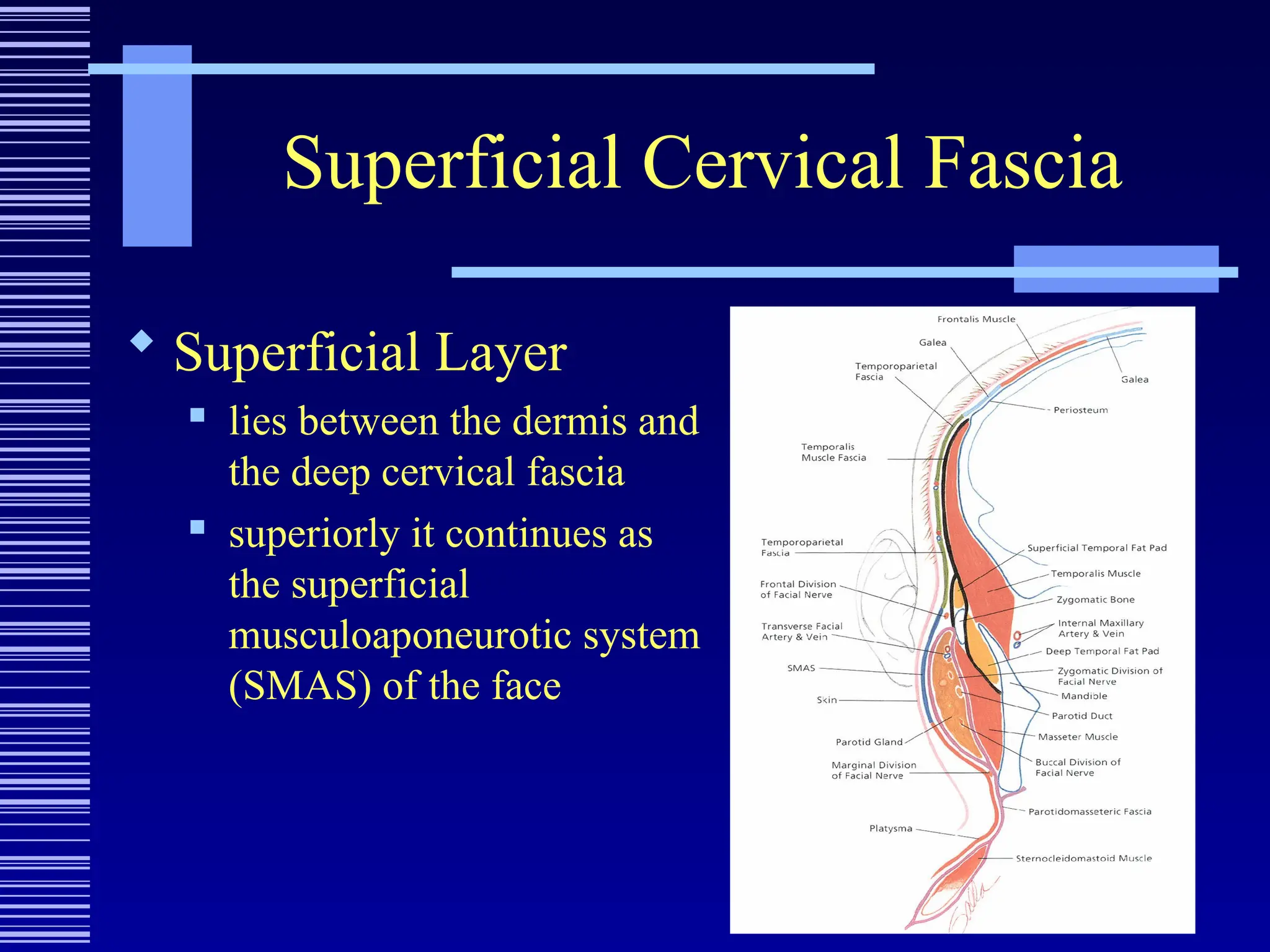
Superficial Cervical Fascia
Superficial Layer
lies between the dermis and
the deep cervical fascia
superiorly it continues as
the superficial
musculoaponeurotic system
(SMAS) of the face
5.
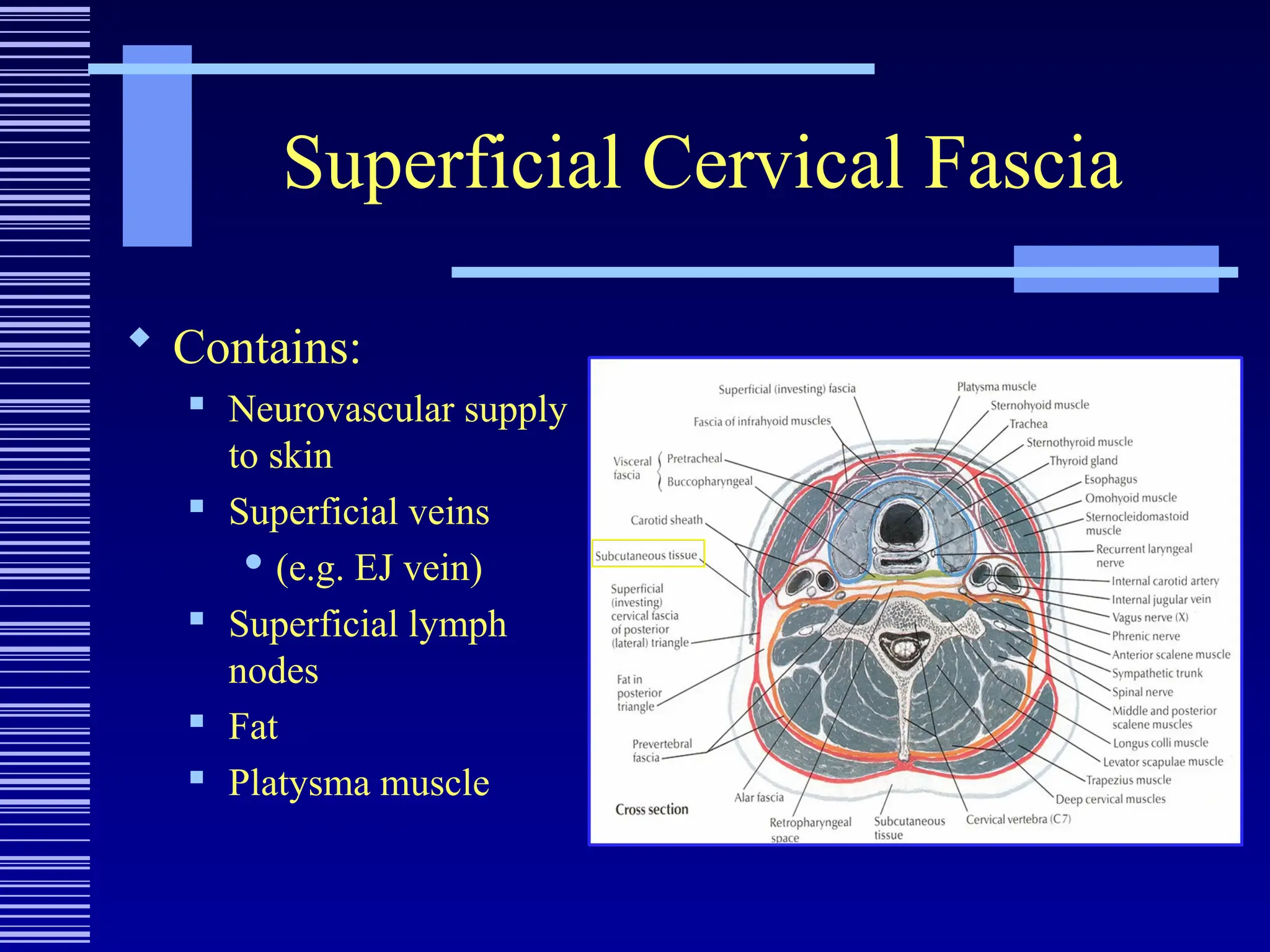
Superficial Cervical Fascia
Contains:
Neurovascular supply
to skin
Superficial veins
(e.g. EJ vein)
Superficial lymph
nodes
Fat
Platysma muscle
6.
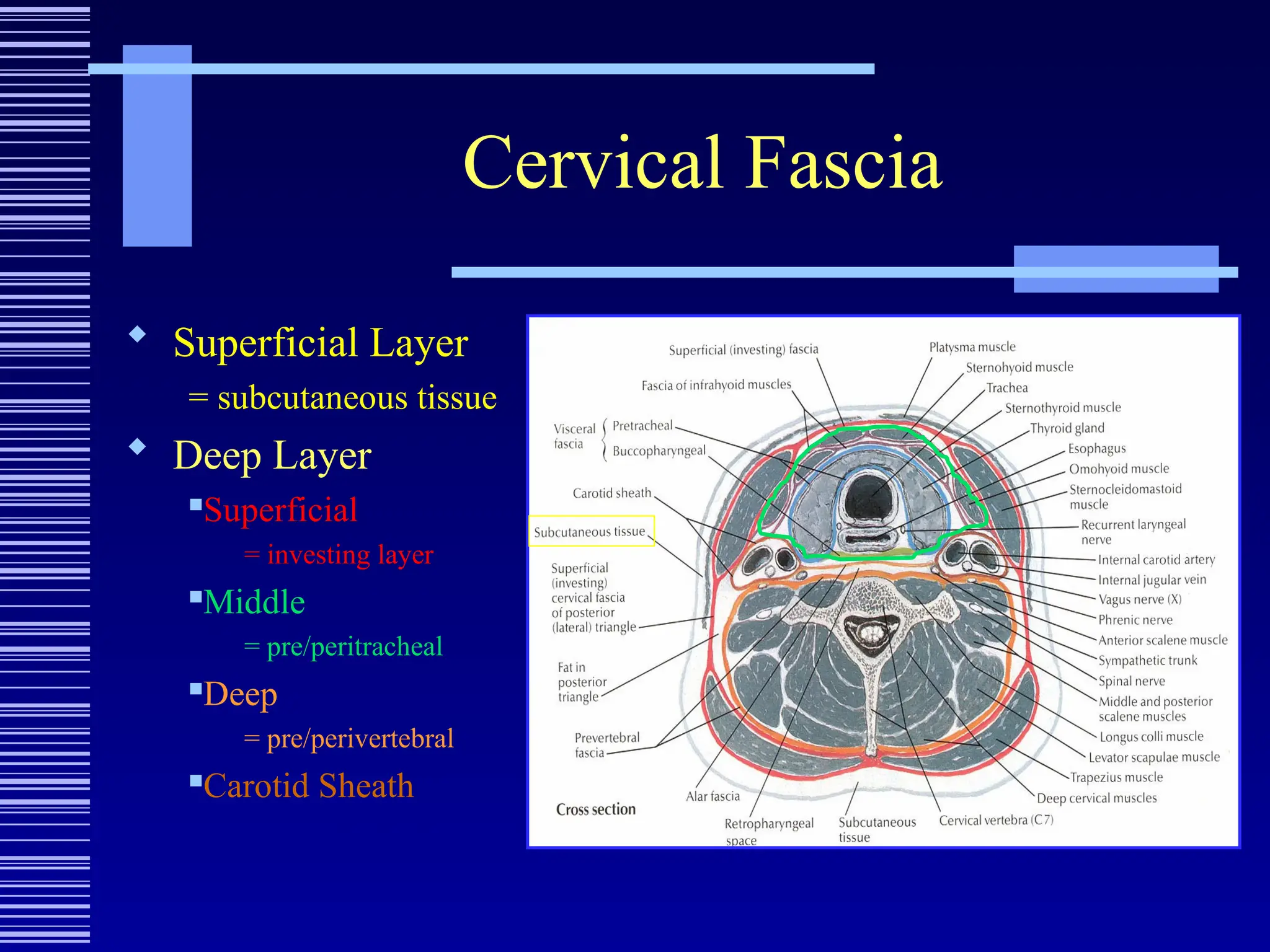
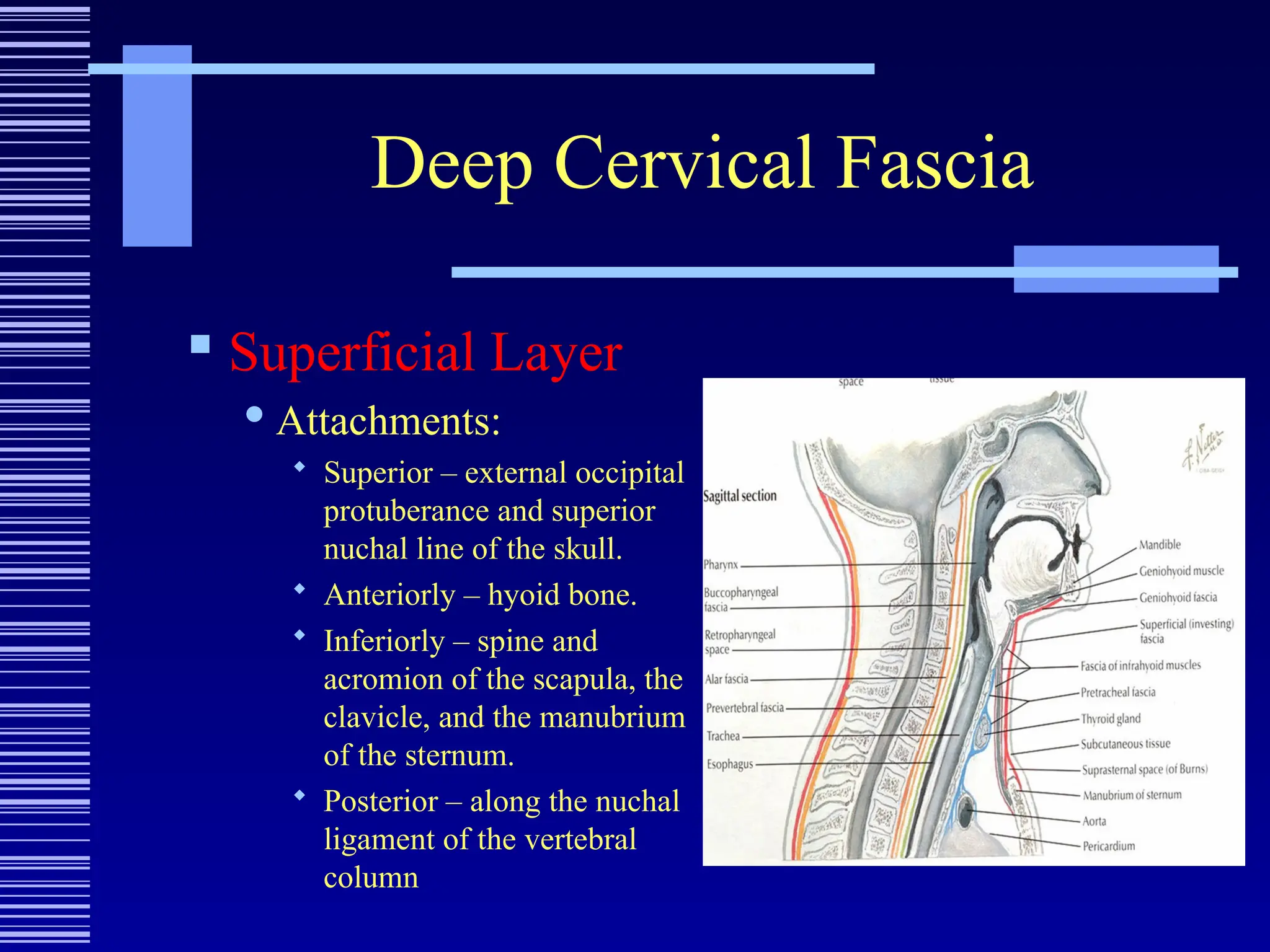
Deep Cervical Fascia
Superficial Layer
Attachments:
Superior – external occipital
protuberance and superior
nuchal line of the skull.
Anteriorly – hyoid bone.
Inferiorly – spine and
acromion of the scapula, the
clavicle, and the manubrium
of the sternum.
Posterior – along the nuchal
ligament of the vertebral
column
7.
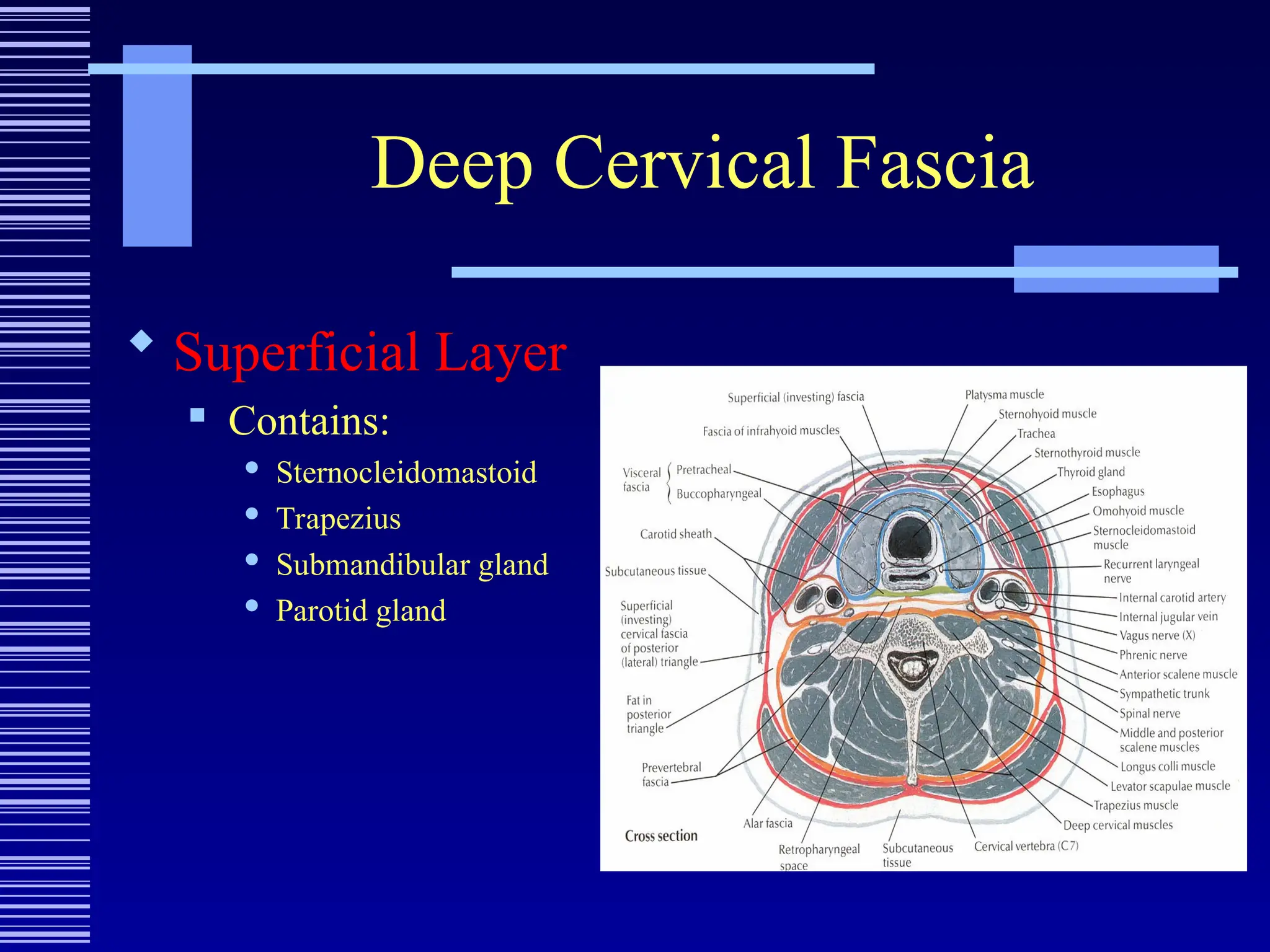
Deep Cervical Fascia
Superficial Layer
Contains:
Sternocleidomastoid
Trapezius
Submandibular gland
Parotid gland
8.
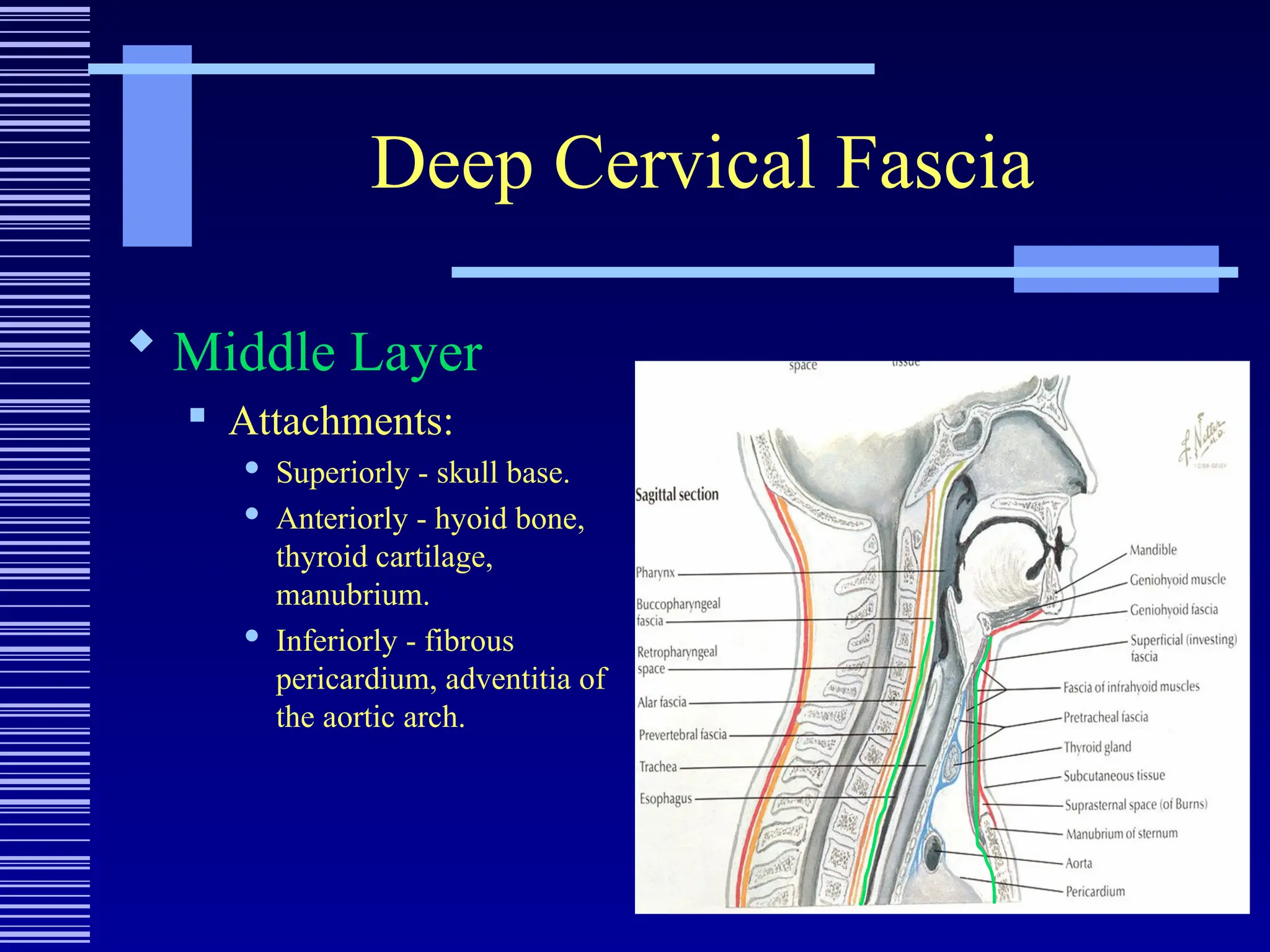
Deep Cervical Fascia
Middle Layer
Attachments:
Superiorly - skull base.
Anteriorly - hyoid bone,
thyroid cartilage,
manubrium.
Inferiorly - fibrous
pericardium, adventitia of
the aortic arch.
9.
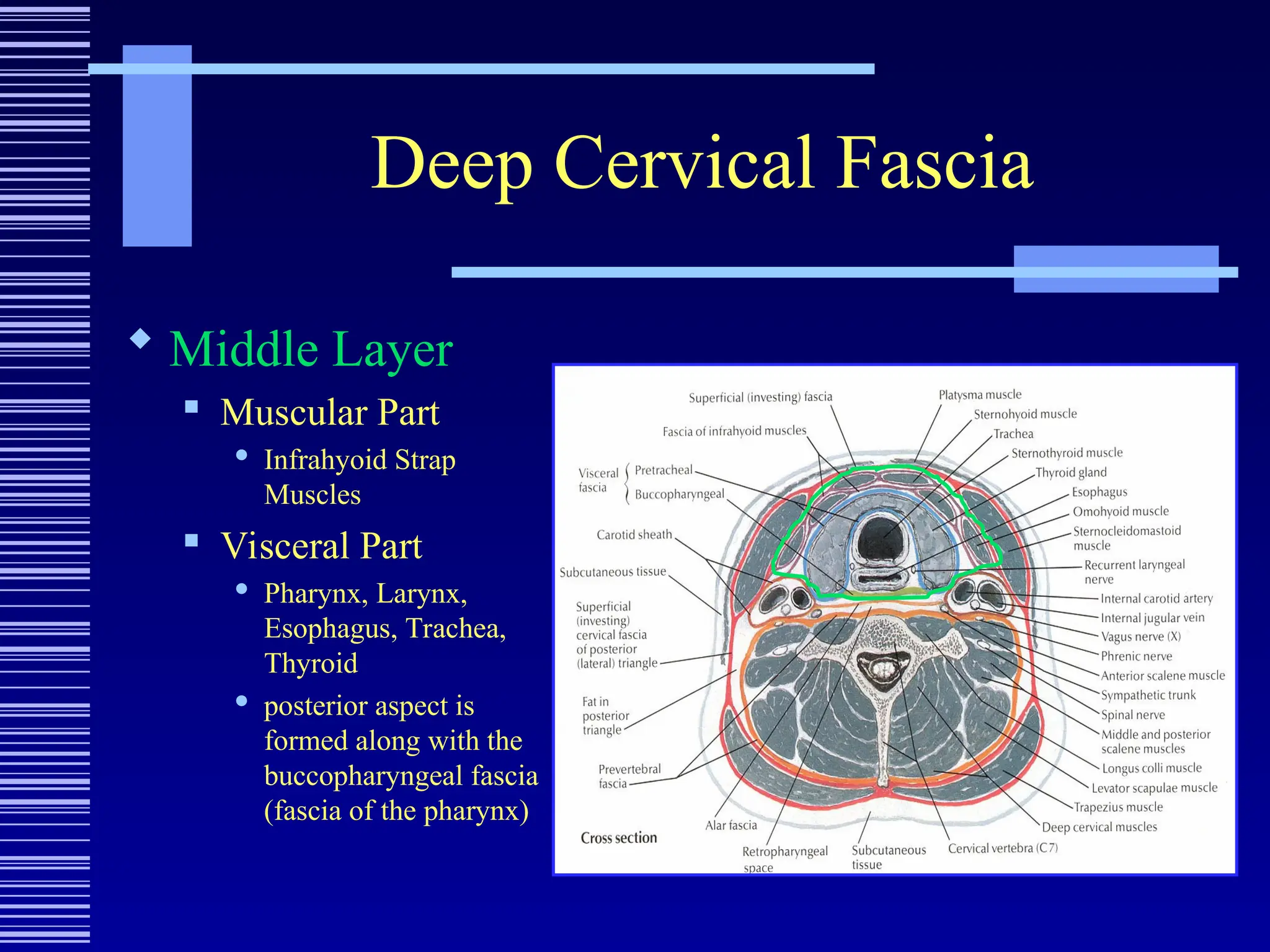
Deep Cervical Fascia
Middle Layer
Muscular Part
Infrahyoid Strap
Muscles
Visceral Part
Pharynx, Larynx,
Esophagus, Trachea,
Thyroid
posterior aspect is
formed along with the
buccopharyngeal fascia
(fascia of the pharynx)
10.
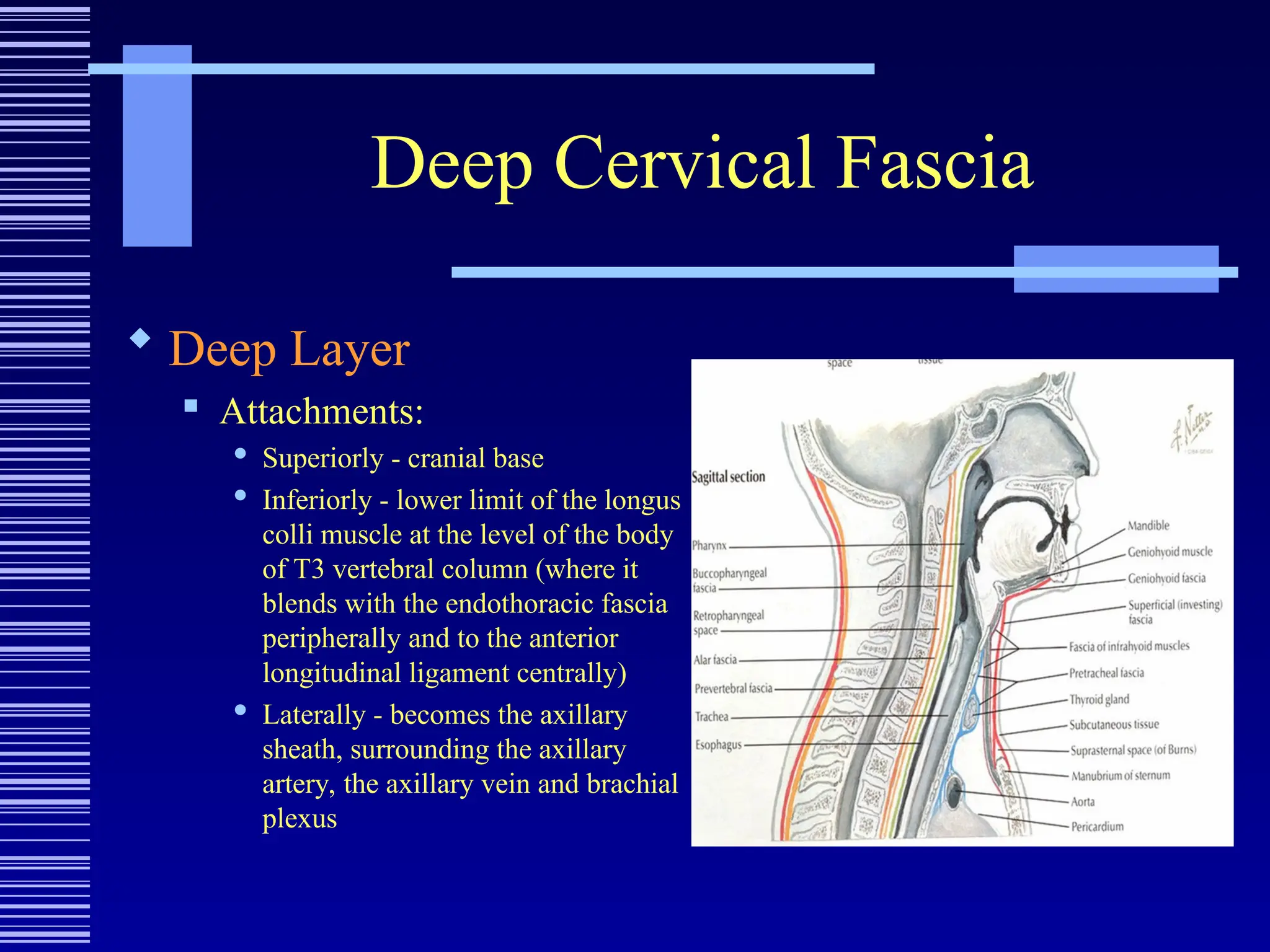
Deep Cervical Fascia
Deep Layer
Attachments:
Superiorly - cranial base
Inferiorly - lower limit of the longus
colli muscle at the level of the body
of T3 vertebral column (where it
blends with the endothoracic fascia
peripherally and to the anterior
longitudinal ligament centrally)
Laterally - becomes the axillary
sheath, surrounding the axillary
artery, the axillary vein and brachial
plexus
11.
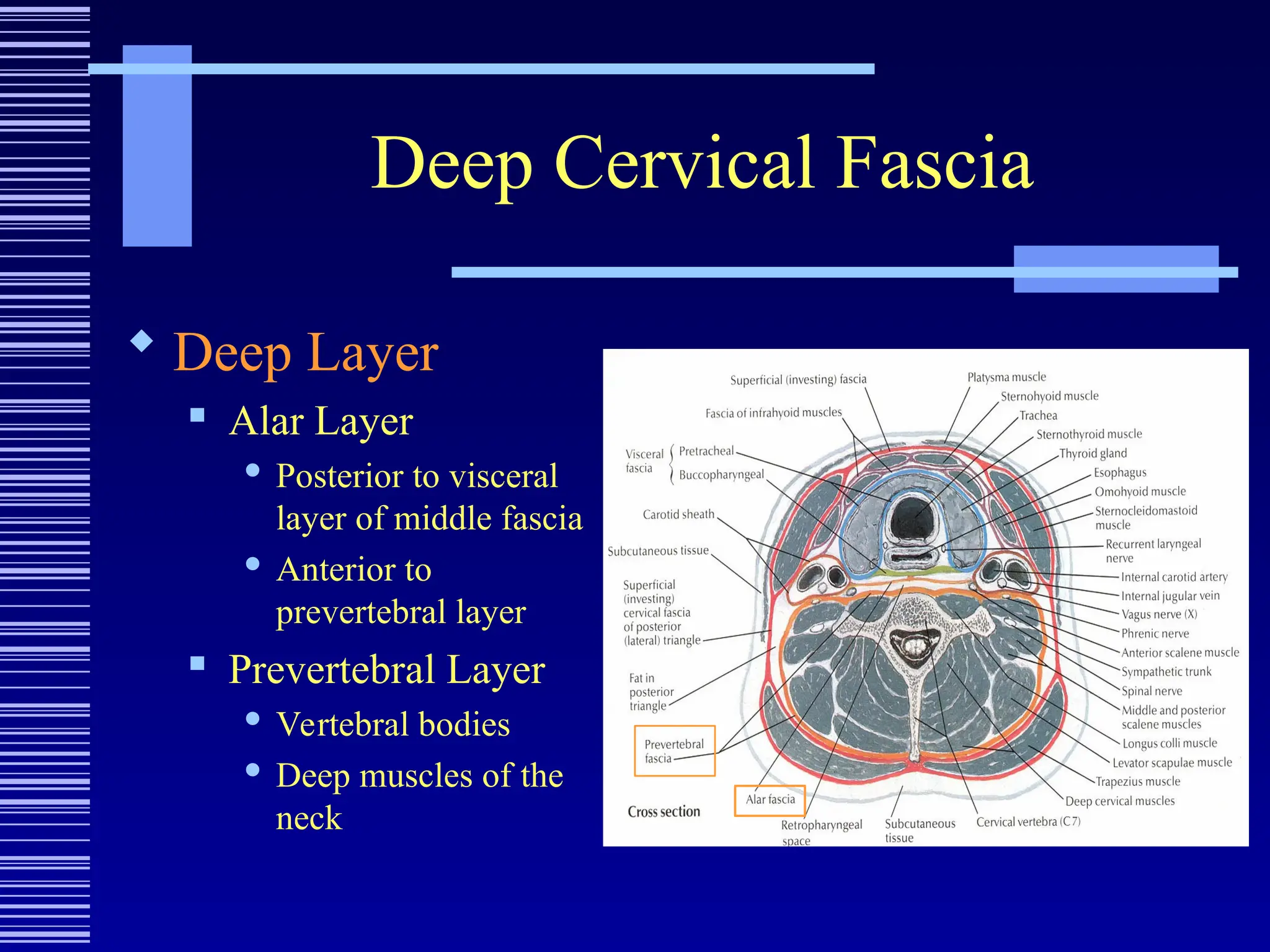
Deep Cervical Fascia
Deep Layer
Alar Layer
Posterior to visceral
layer of middle fascia
Anterior to
prevertebral layer
Prevertebral Layer
Vertebral bodies
Deep muscles of the
neck
12.
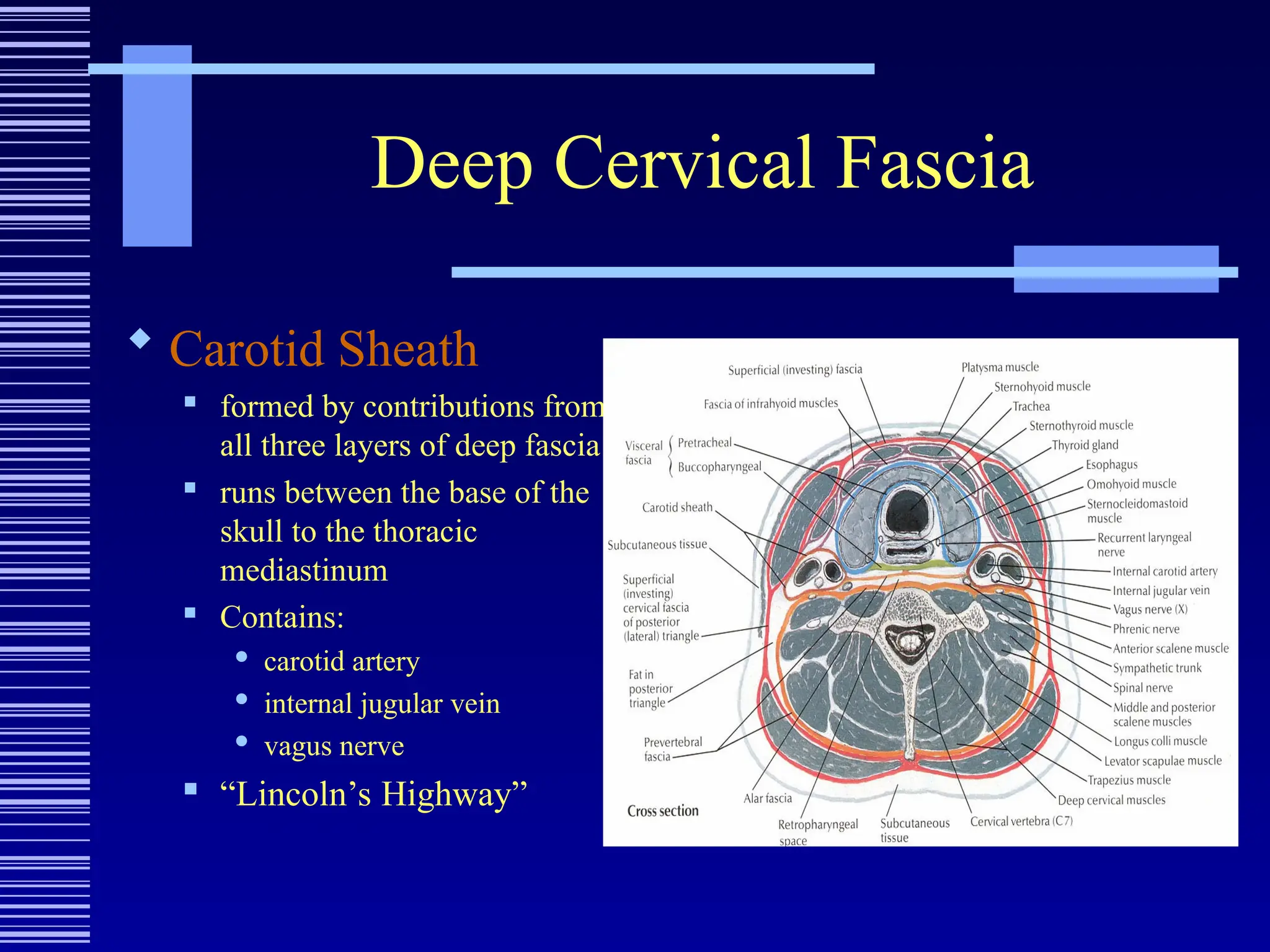
Deep Cervical Fascia
Carotid Sheath
formed by contributions from
all three layers of deep fascia
runs between the base of the
skull to the thoracic
mediastinum
Contains:
carotid artery
internal jugular vein
vagus nerve
“Lincoln’s Highway”
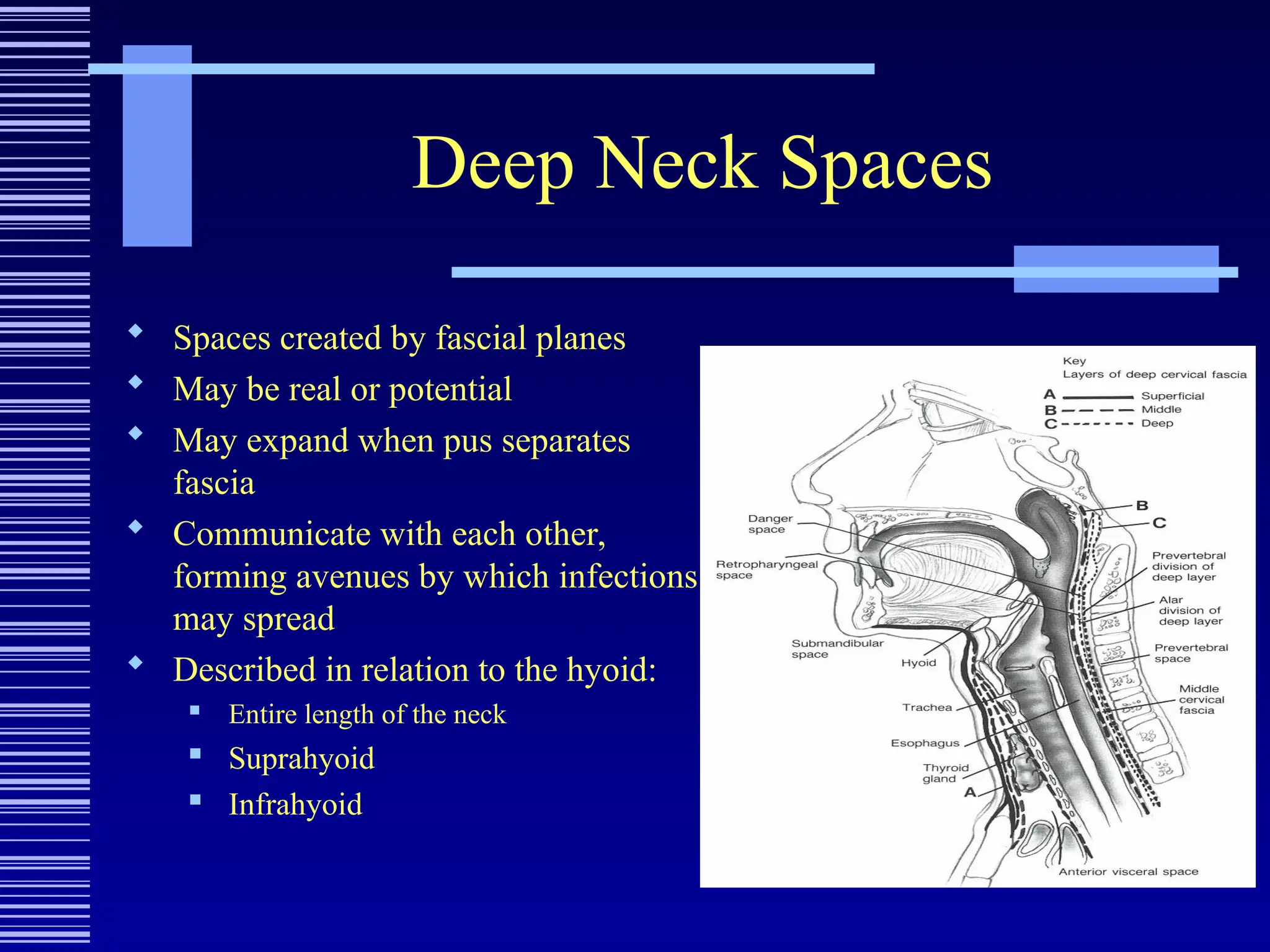
Deep Neck Spaces
Spaces created by fascial planes
May be real or potential
May expand when pus separates
fascia
Communicate with each other,
forming avenues by which infections
may spread
Described in relation to the hyoid:
Entire length of the neck
Suprahyoid
Infrahyoid
15.
Entire Length ofthe Neck
Deep Neck Spaces
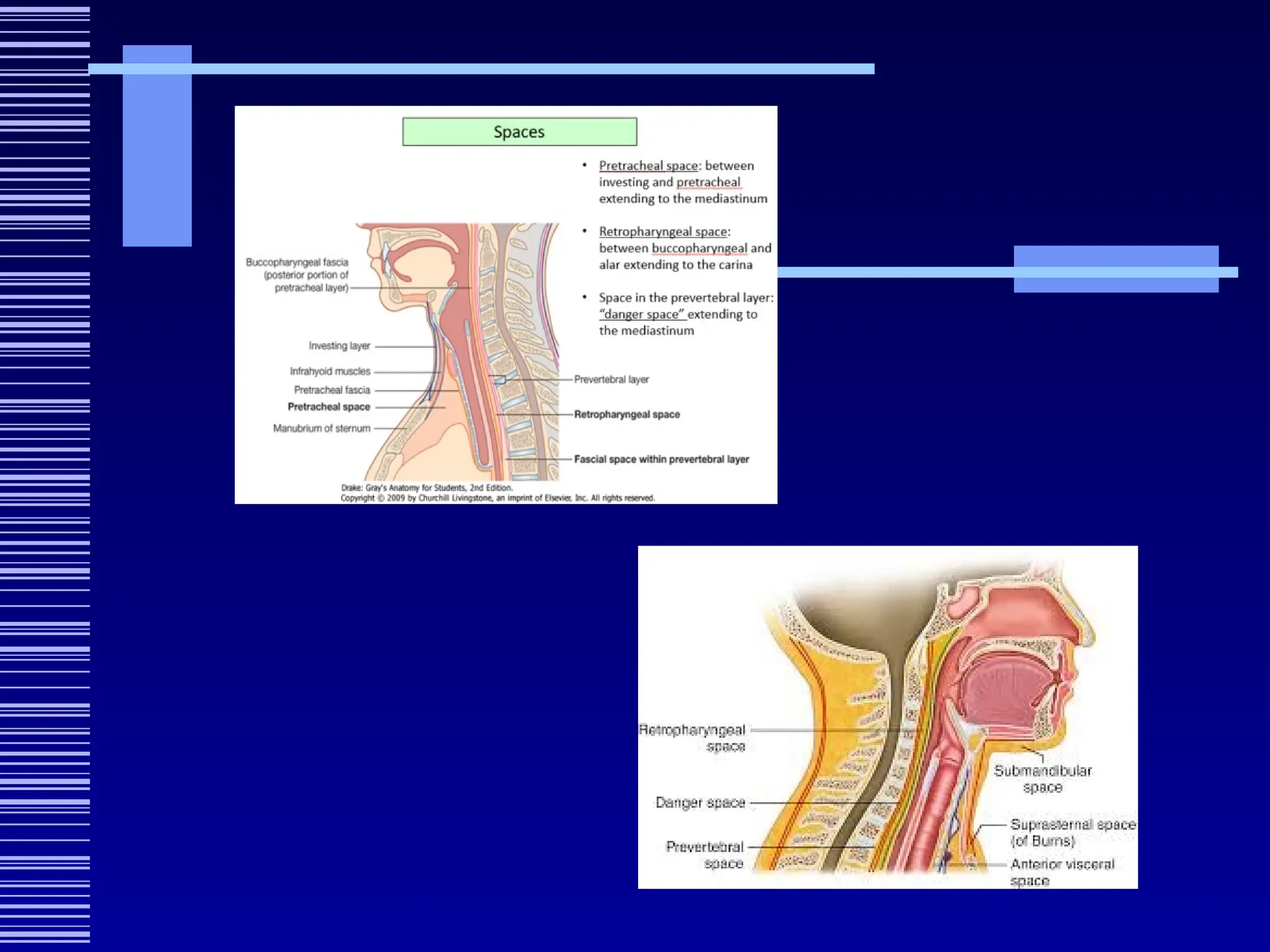
Retropharyngeal Space
Danger Space
Pre/perivertebral Space
Carotid Space (visceral/vascular)
16.
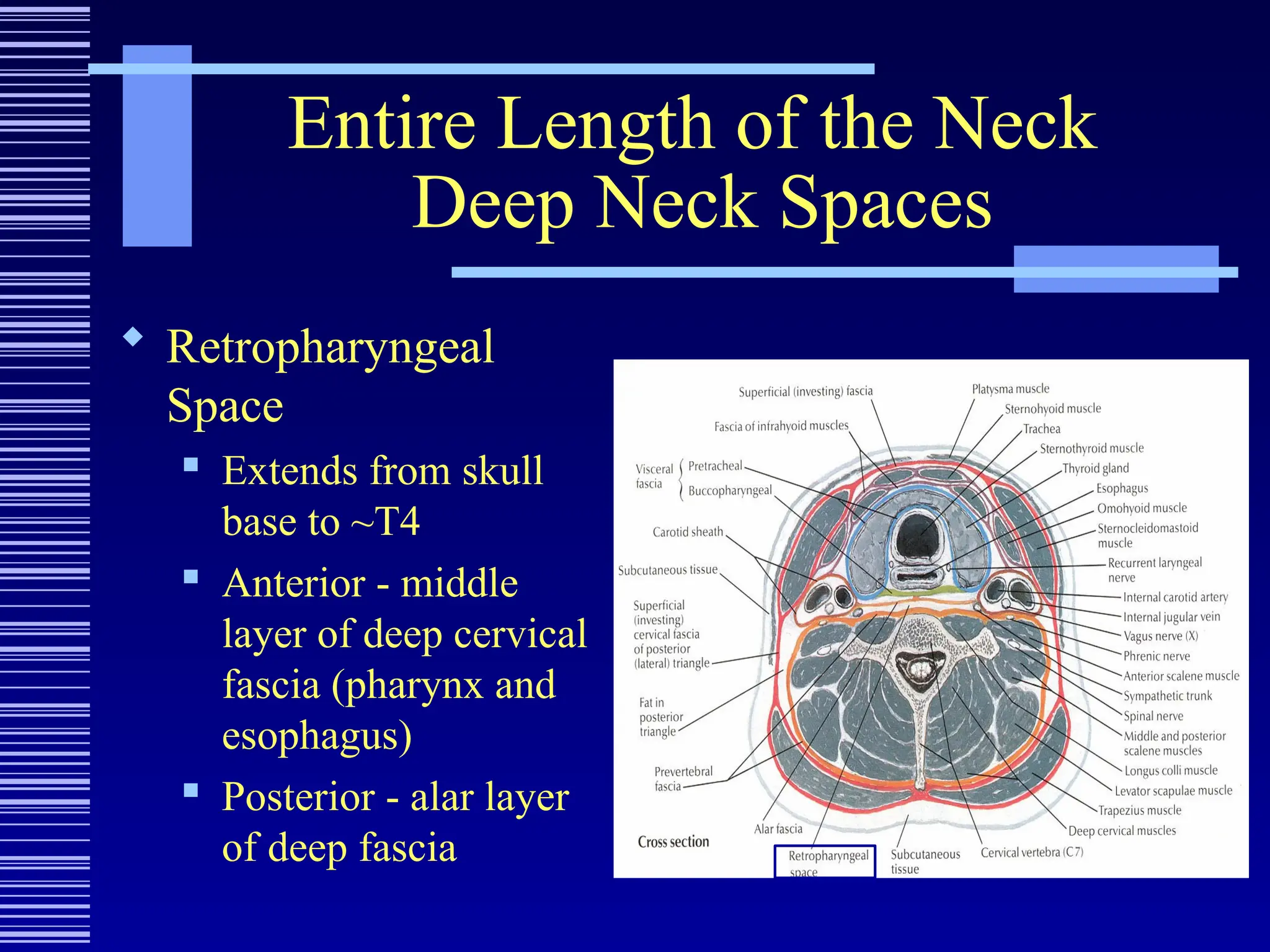
Entire Length ofthe Neck
Deep Neck Spaces
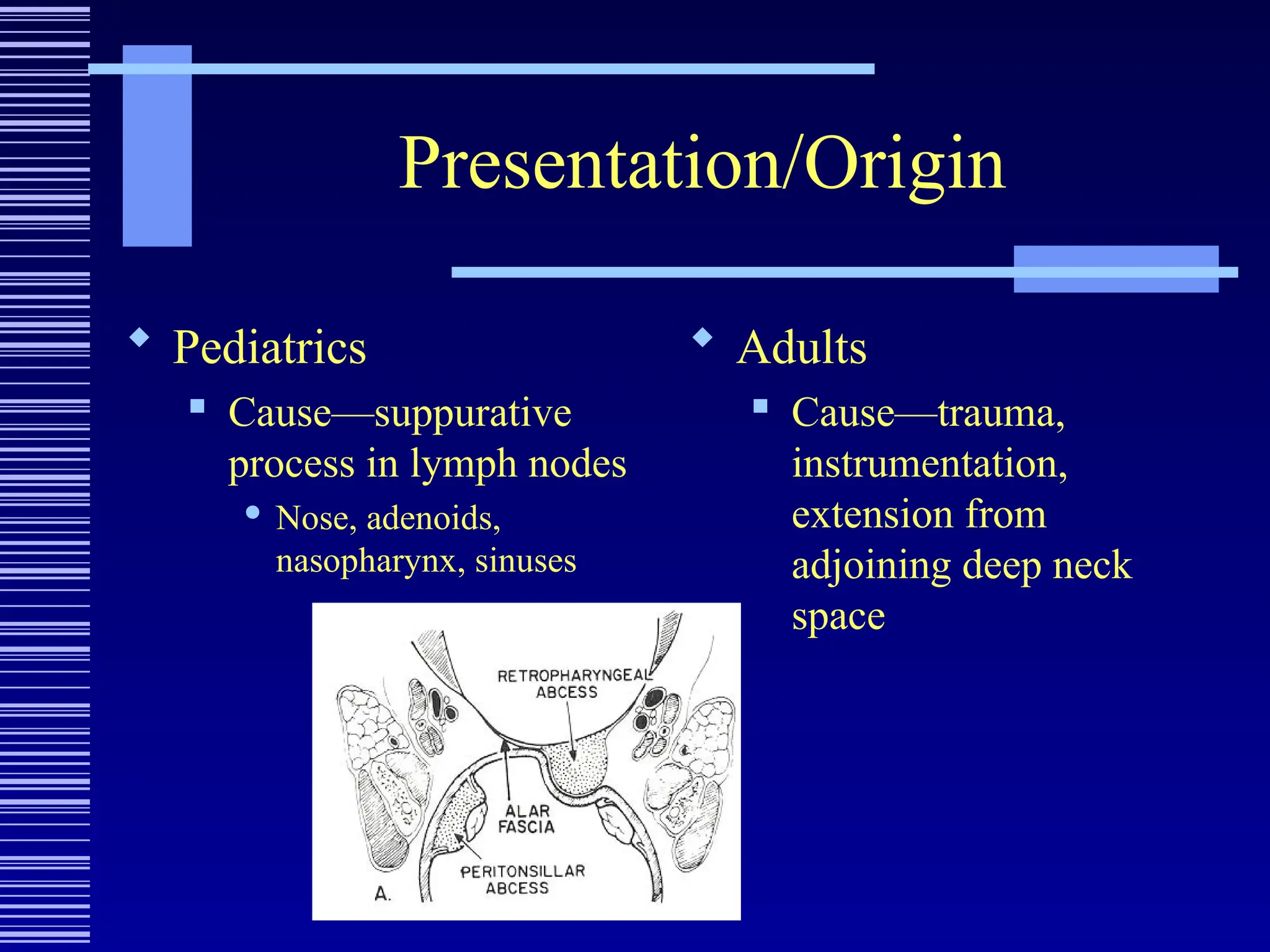
Retropharyngeal
Space
Extends from skull
base to ~T4
Anterior - middle
layer of deep cervical
fascia (pharynx and
esophagus)
Posterior - alar layer
of deep fascia
17.
Entire Length ofthe Neck
Deep Neck Spaces
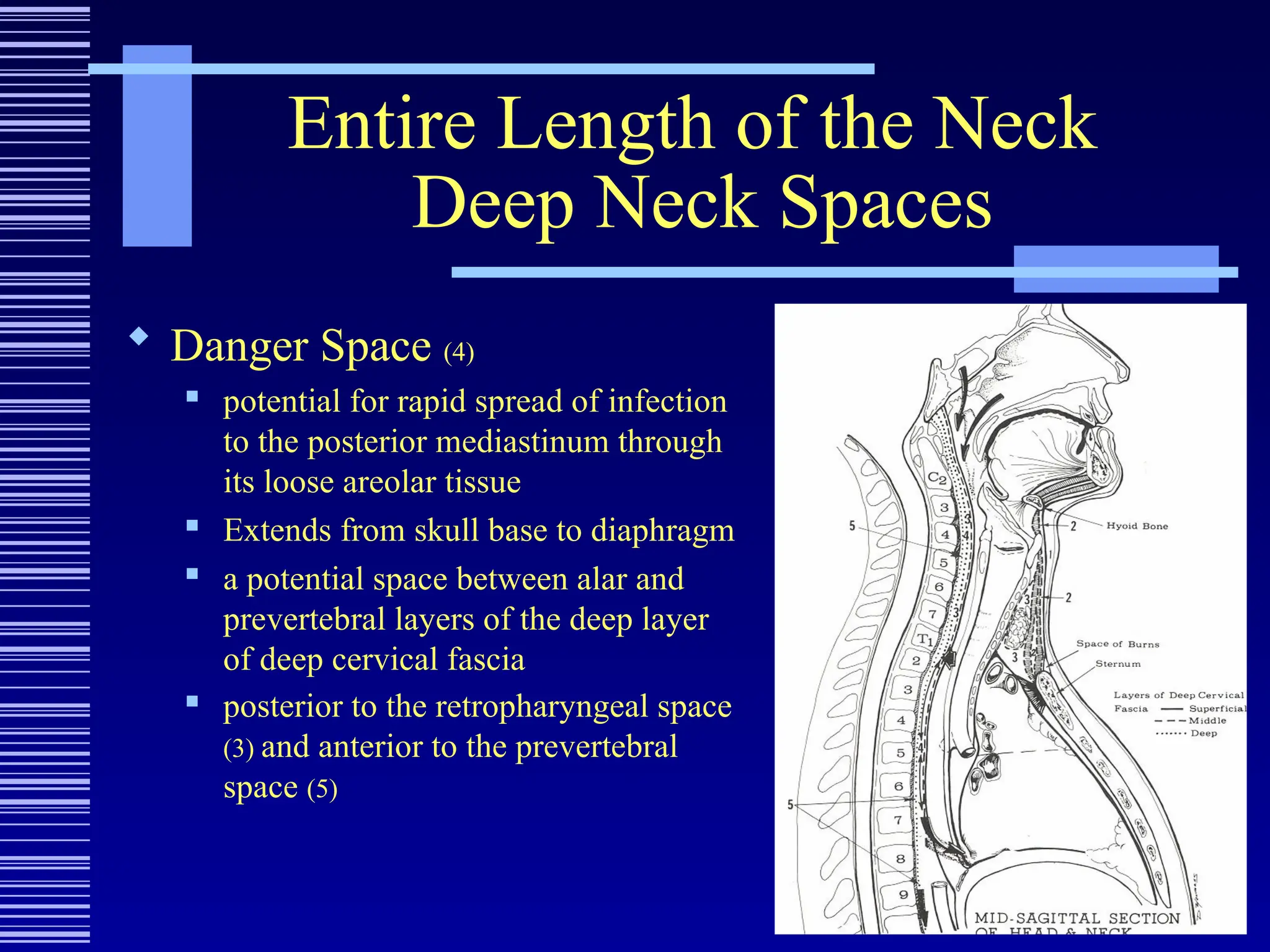
Danger Space (4)
potential for rapid spread of infection
to the posterior mediastinum through
its loose areolar tissue
Extends from skull base to diaphragm
a potential space between alar and
prevertebral layers of the deep layer
of deep cervical fascia
posterior to the retropharyngeal space
(3) and anterior to the prevertebral
space (5)
19.
Entire Length ofthe Neck
Deep Neck Spaces
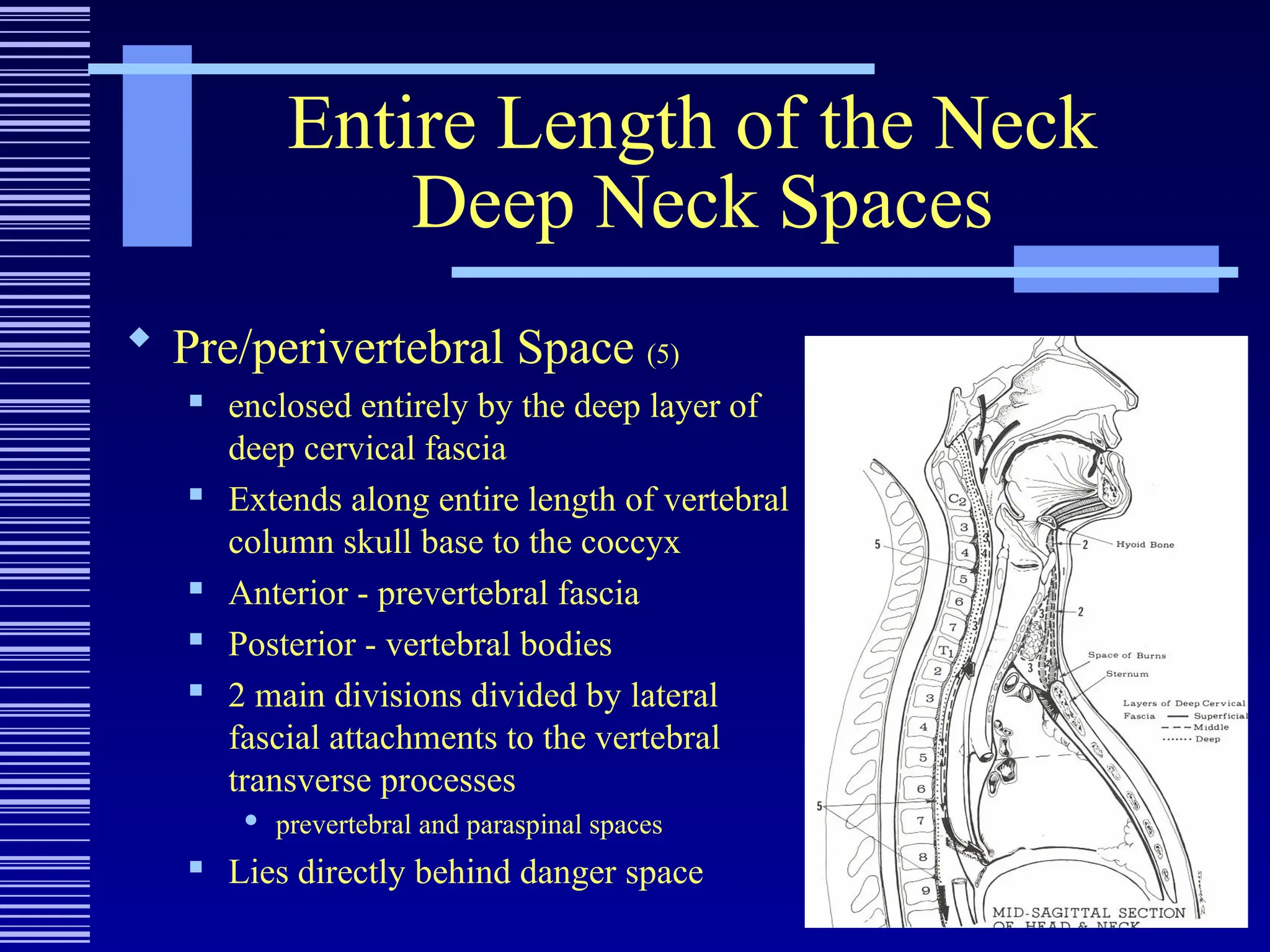
Pre/perivertebral Space (5)
enclosed entirely by the deep layer of
deep cervical fascia
Extends along entire length of vertebral
column skull base to the coccyx
Anterior - prevertebral fascia
Posterior - vertebral bodies
2 main divisions divided by lateral
fascial attachments to the vertebral
transverse processes
prevertebral and paraspinal spaces
Lies directly behind danger space
20.
Entire Length ofthe Neck
Deep Neck Spaces
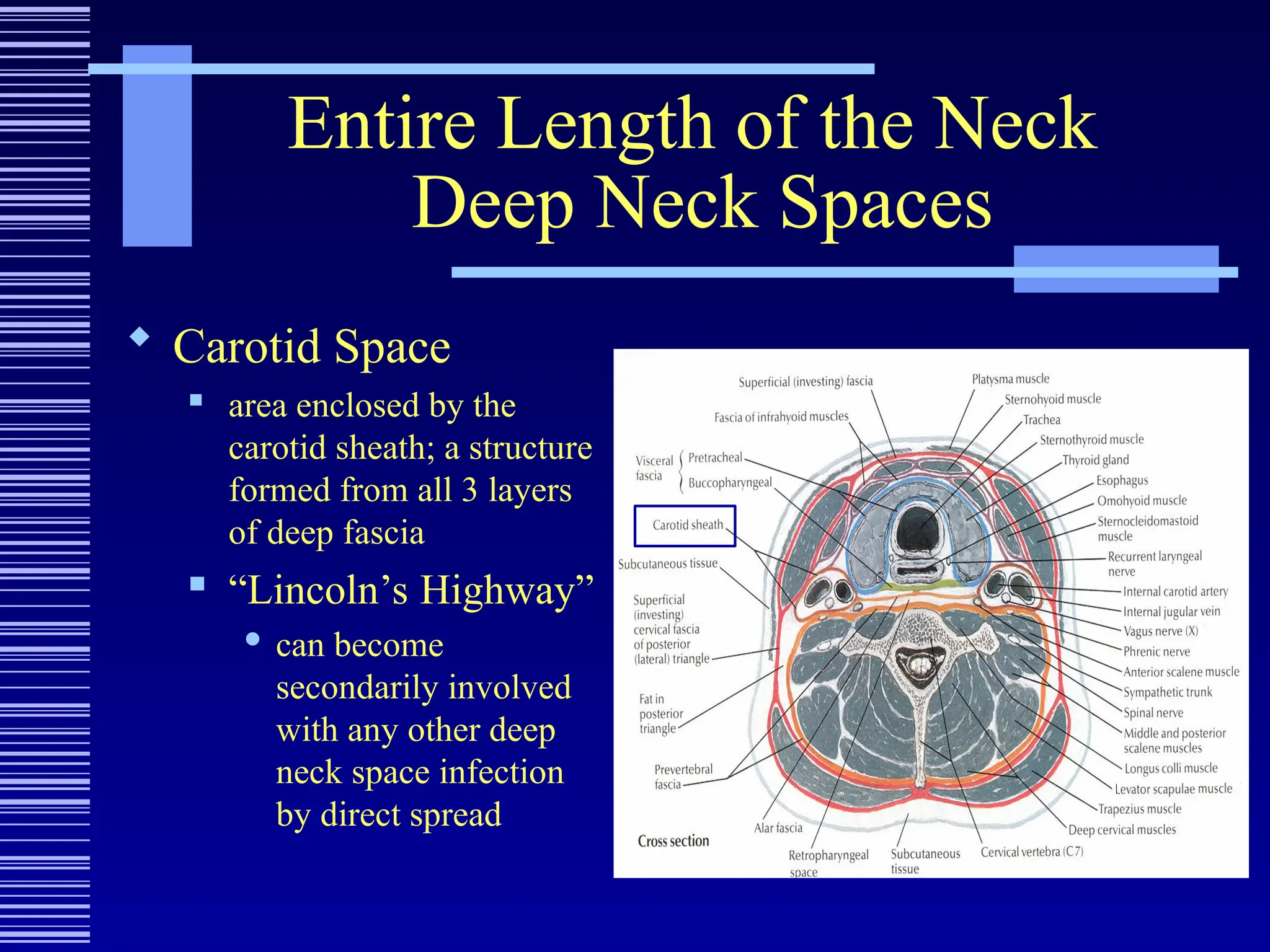
Carotid Space
area enclosed by the
carotid sheath; a structure
formed from all 3 layers
of deep fascia
“Lincoln’s Highway”
can become
secondarily involved
with any other deep
neck space infection
by direct spread
21.
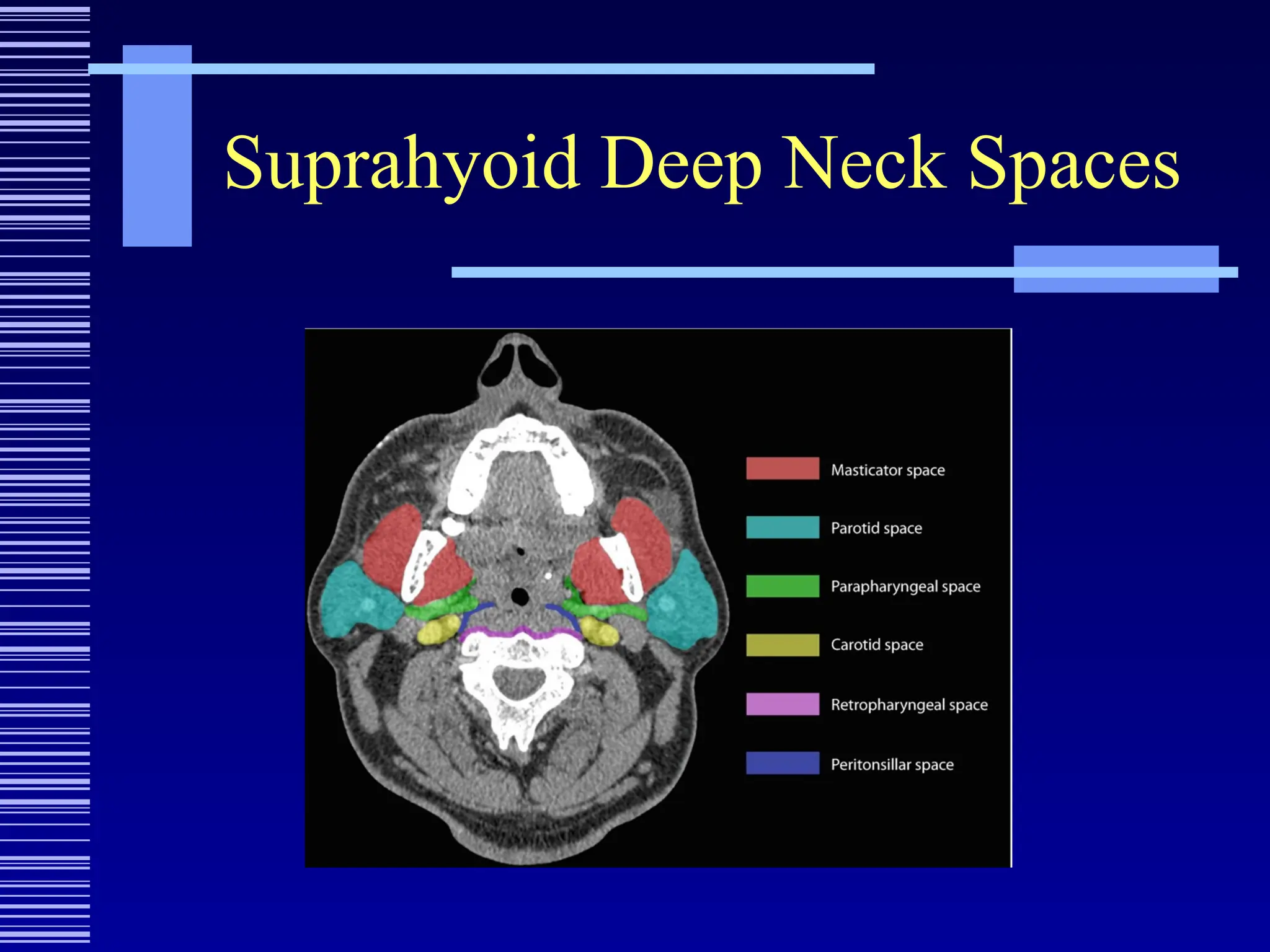
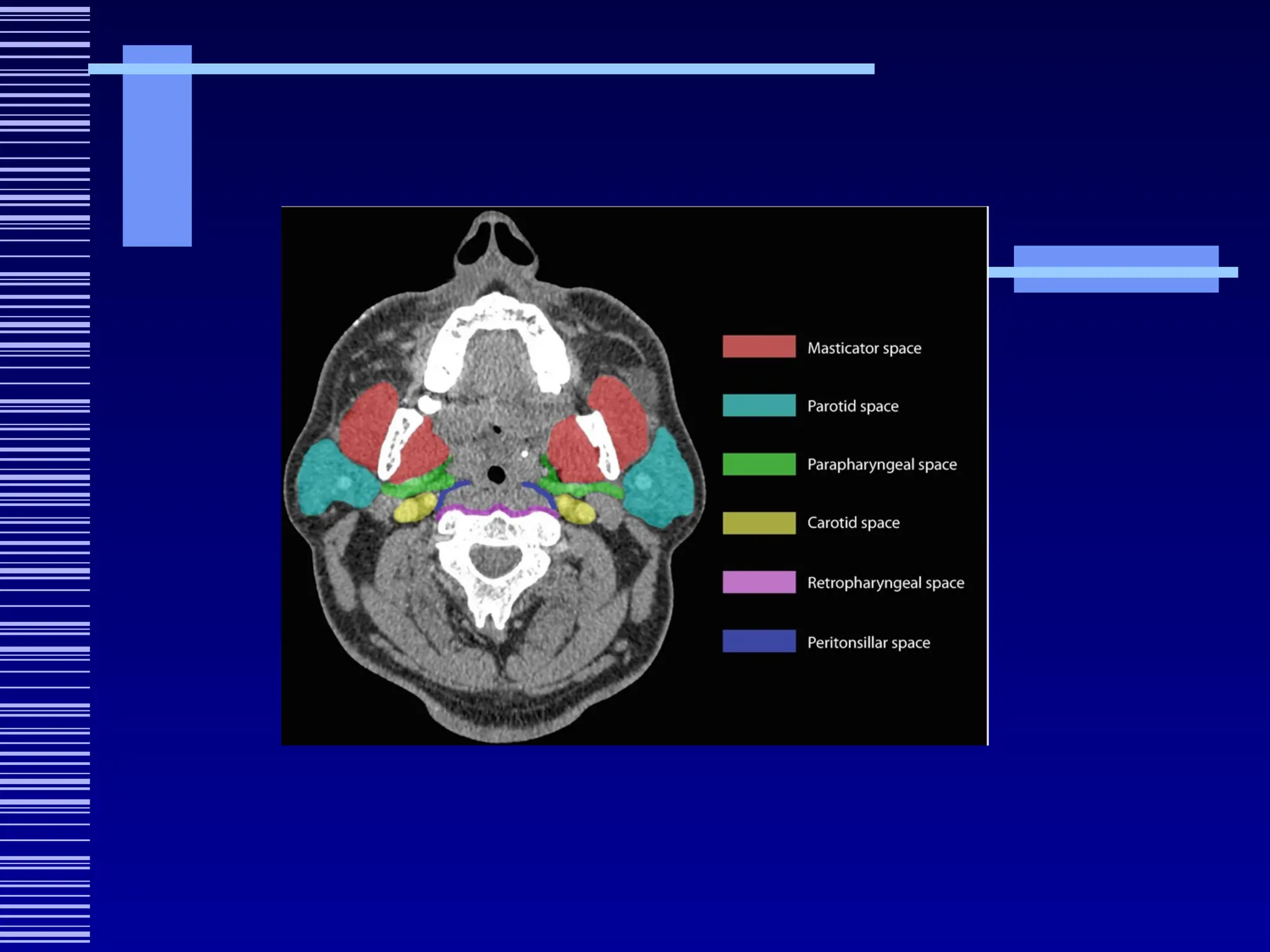
Suprahyoid Deep NeckSpaces
Sublingual Space
Submandibular Space
Peritonsillar Space
Parapharyngeal Space
Pharyngeal Mucosa Space
Masticator Space
Parotid Space
22.
Suprahyoid Deep NeckSpaces
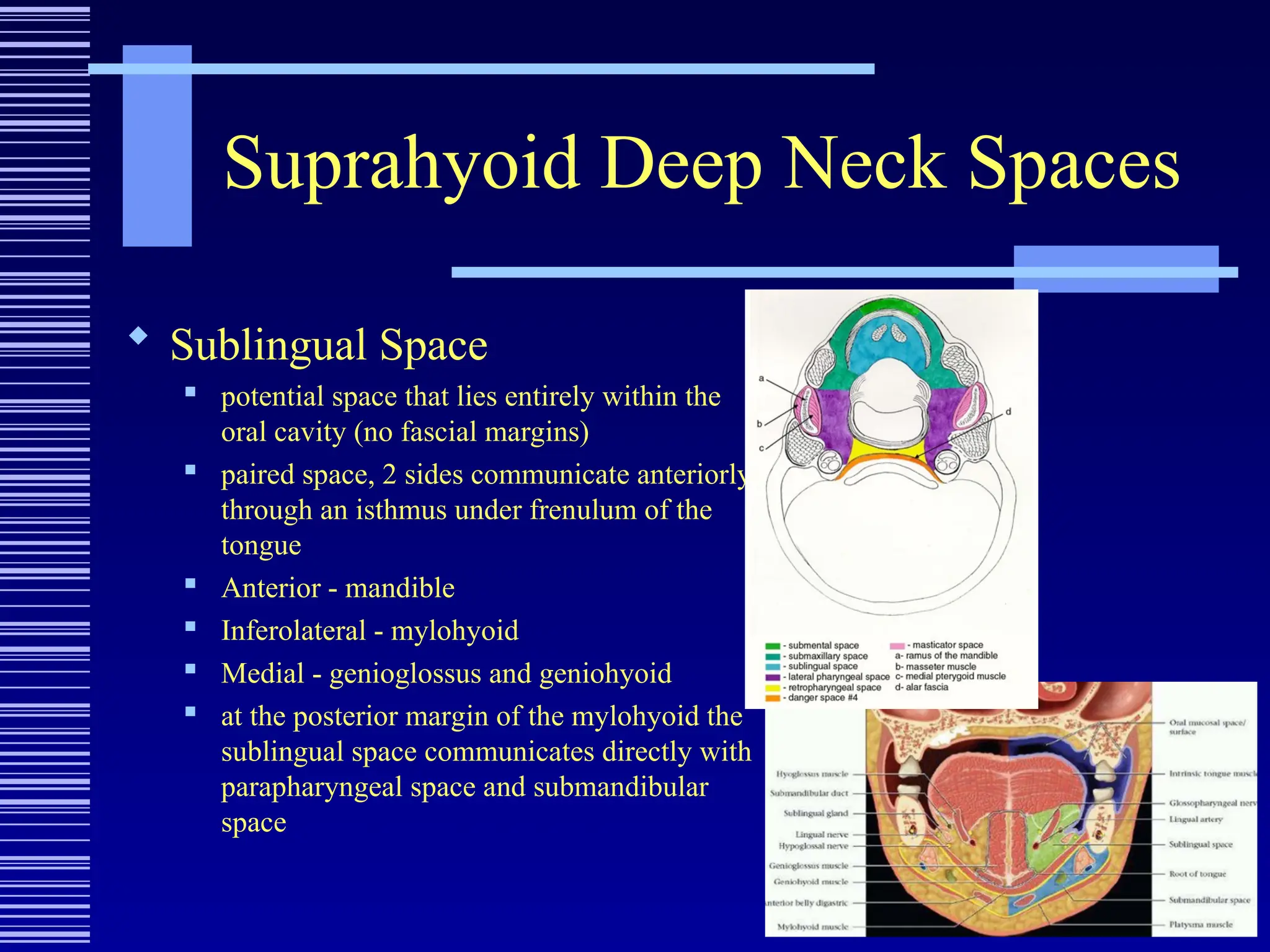
Sublingual Space
potential space that lies entirely within the
oral cavity (no fascial margins)
paired space, 2 sides communicate anteriorly
through an isthmus under frenulum of the
tongue
Anterior - mandible
Inferolateral - mylohyoid
Medial - genioglossus and geniohyoid
at the posterior margin of the mylohyoid the
sublingual space communicates directly with
parapharyngeal space and submandibular
space
23.
Suprahyoid Deep NeckSpaces
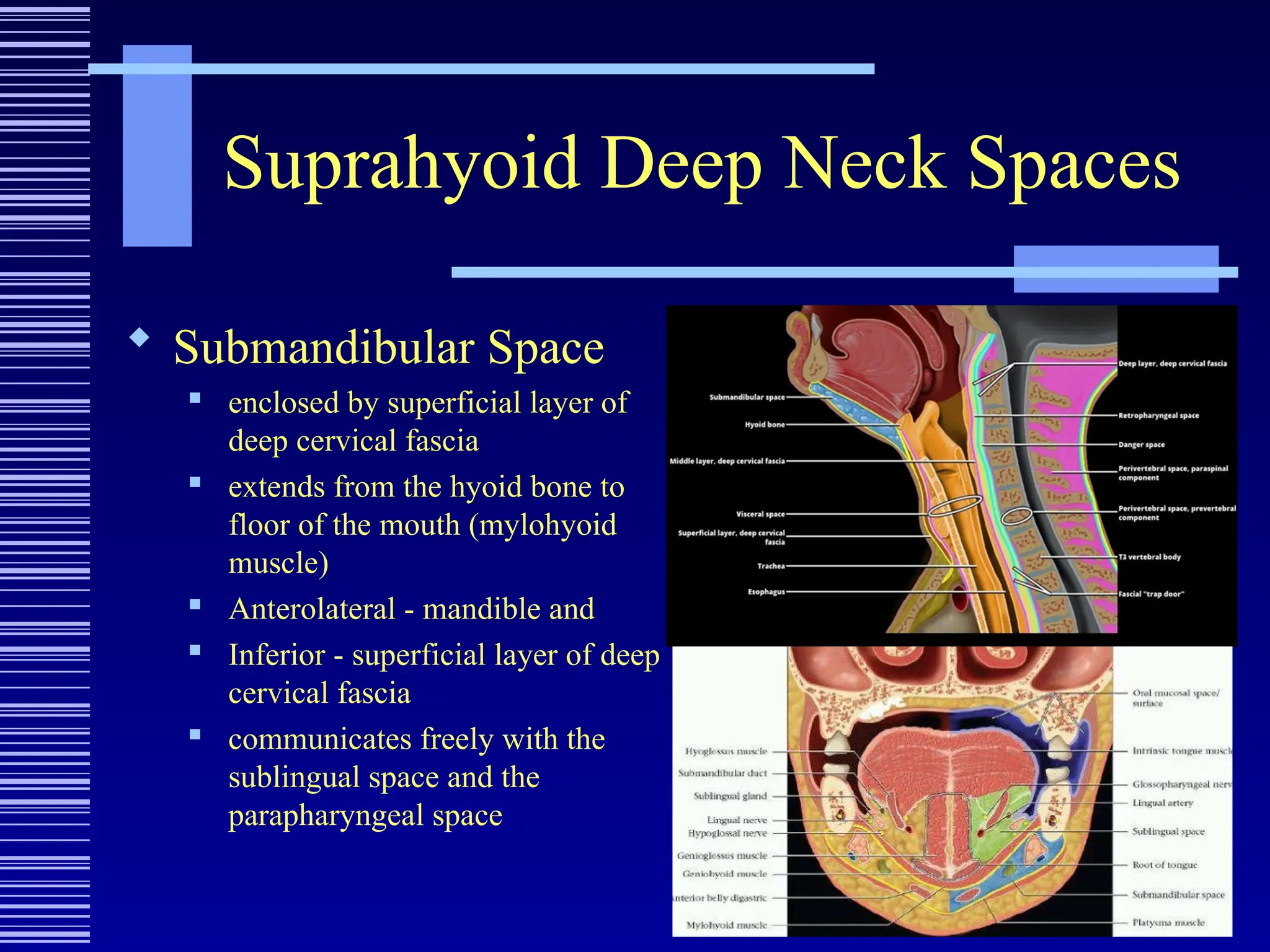
Submandibular Space
enclosed by superficial layer of
deep cervical fascia
extends from the hyoid bone to
floor of the mouth (mylohyoid
muscle)
Anterolateral - mandible and
Inferior - superficial layer of deep
cervical fascia
communicates freely with the
sublingual space and the
parapharyngeal space
24.
Suprahyoid Deep NeckSpaces
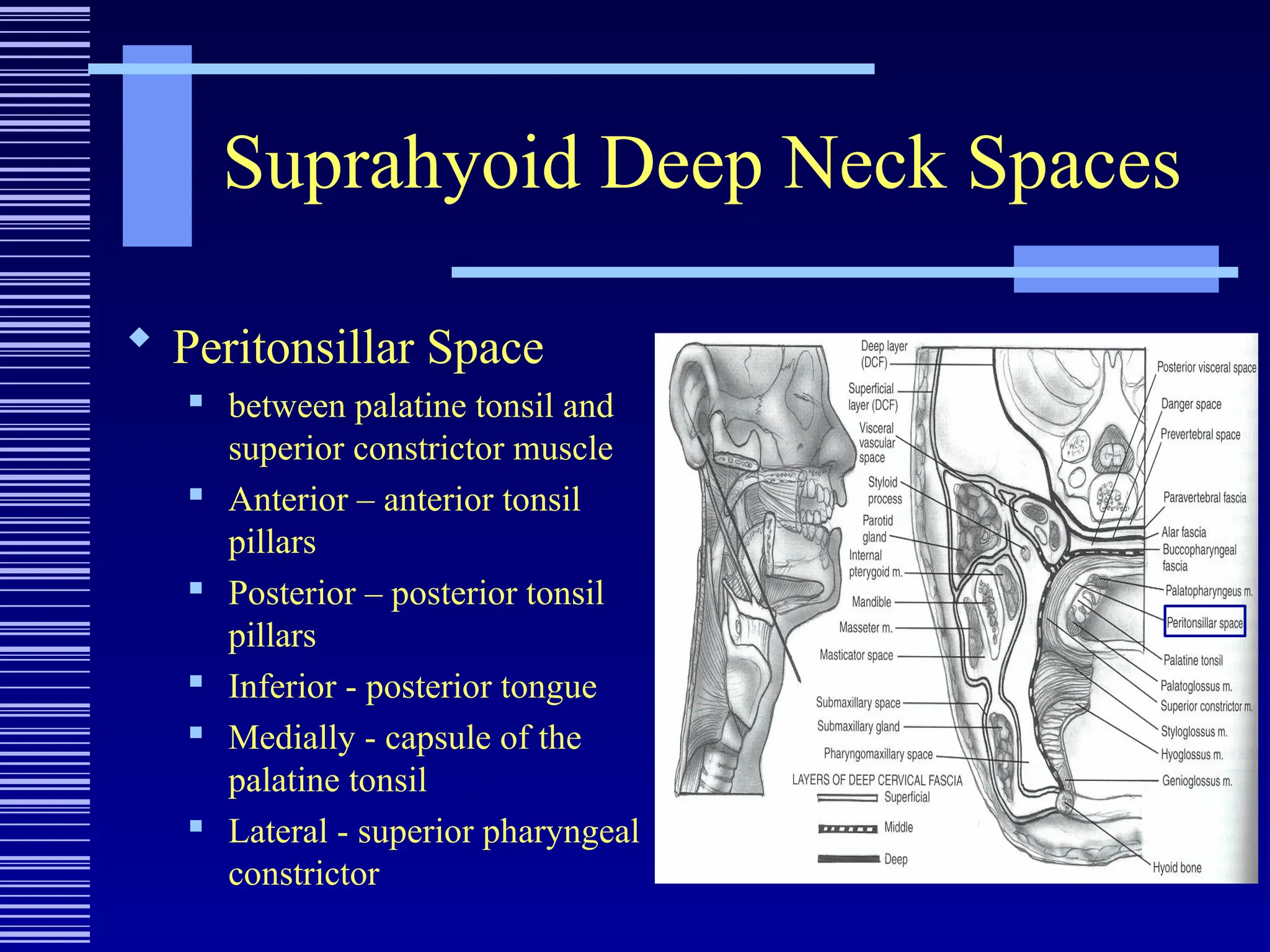
Peritonsillar Space
between palatine tonsil and
superior constrictor muscle
Anterior – anterior tonsil
pillars
Posterior – posterior tonsil
pillars
Inferior - posterior tongue
Medially - capsule of the
palatine tonsil
Lateral - superior pharyngeal
constrictor
Suprahyoid Deep NeckSpaces
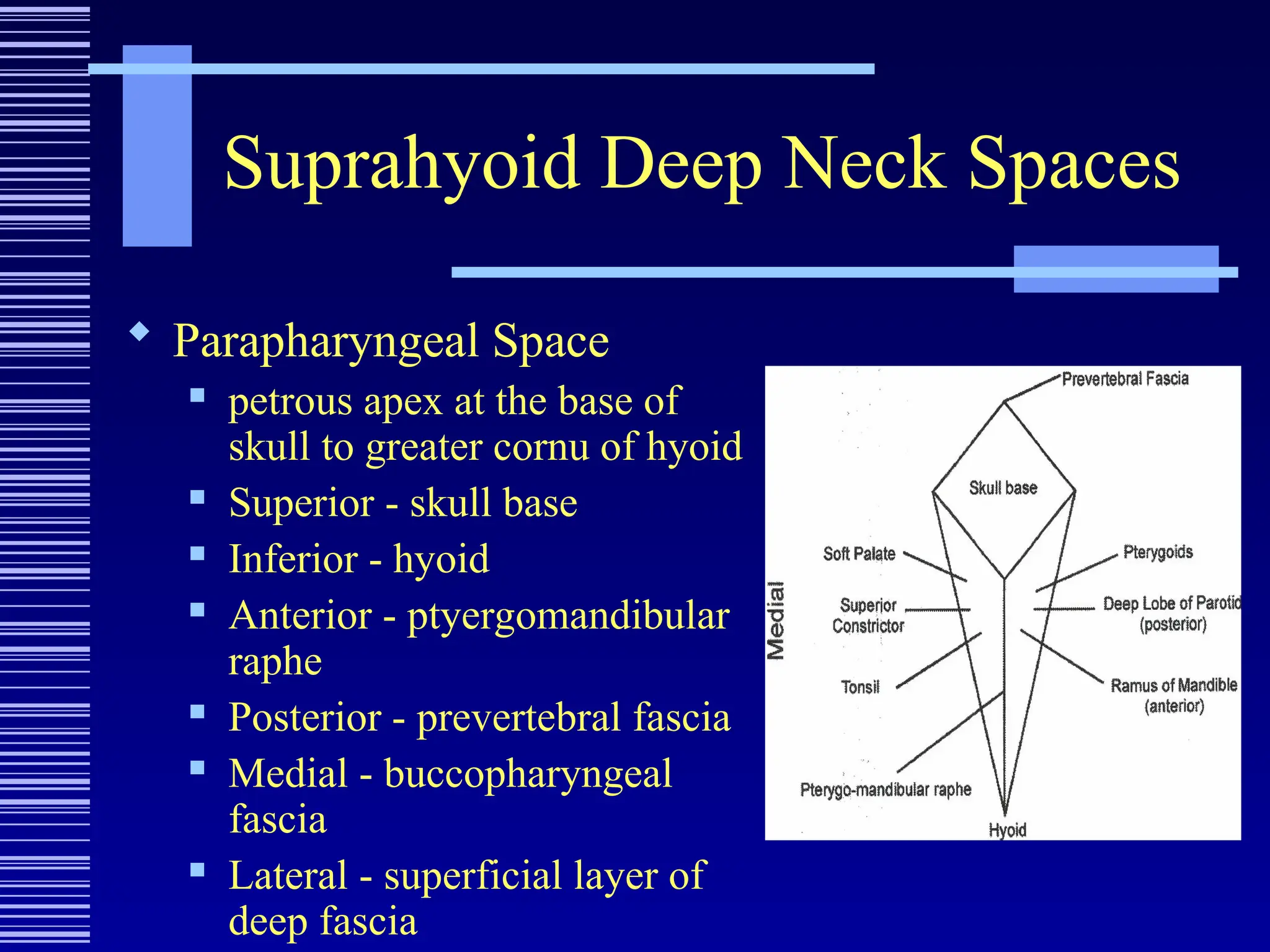
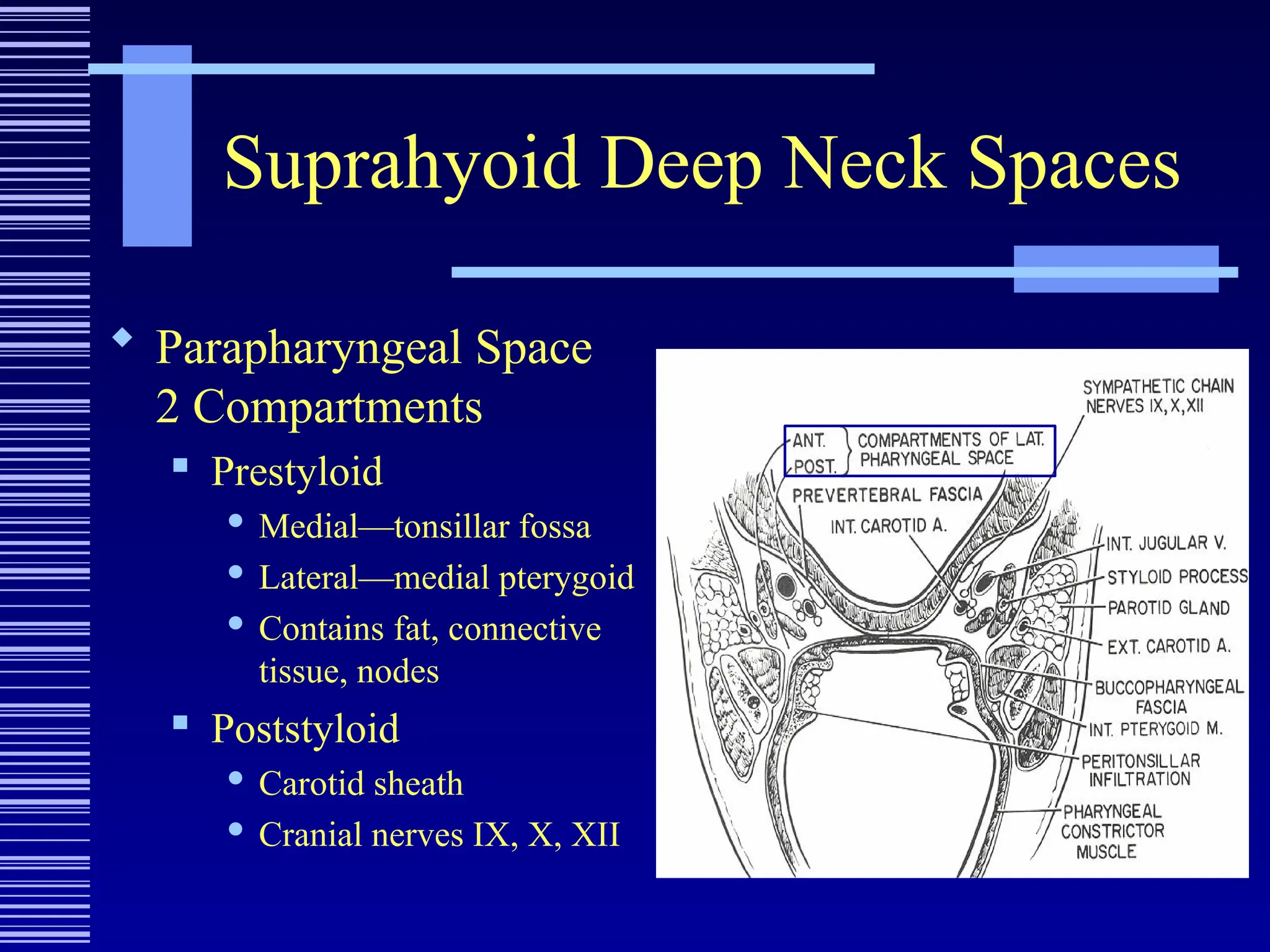
Parapharyngeal Space
petrous apex at the base of
skull to greater cornu of hyoid
Superior - skull base
Inferior - hyoid
Anterior - ptyergomandibular
raphe
Posterior - prevertebral fascia
Medial - buccopharyngeal
fascia
Lateral - superficial layer of
deep fascia
Suprahyoid Deep NeckSpaces
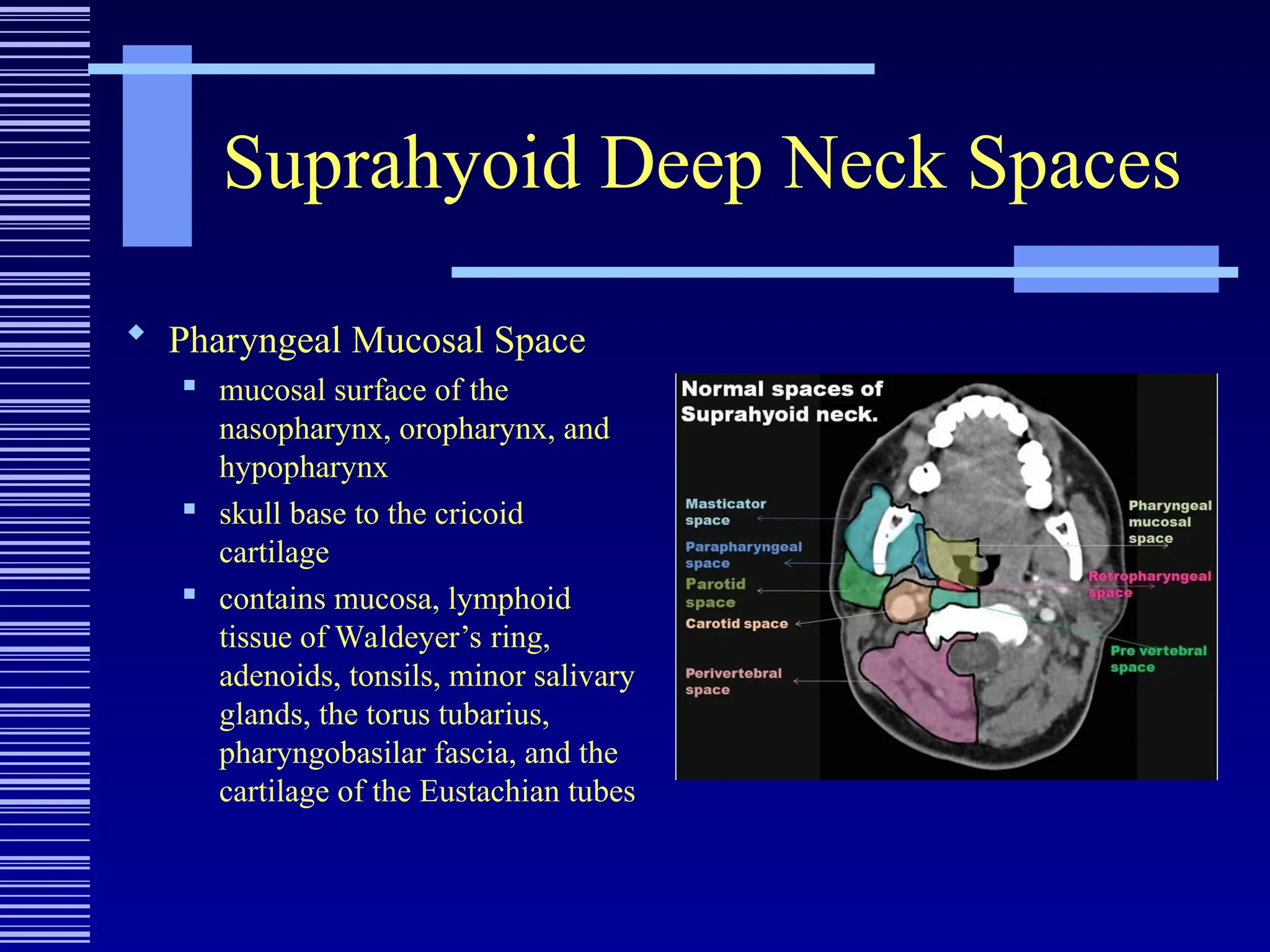
Pharyngeal Mucosal Space
mucosal surface of the
nasopharynx, oropharynx, and
hypopharynx
skull base to the cricoid
cartilage
contains mucosa, lymphoid
tissue of Waldeyer’s ring,
adenoids, tonsils, minor salivary
glands, the torus tubarius,
pharyngobasilar fascia, and the
cartilage of the Eustachian tubes
30.
Suprahyoid Deep NeckSpaces
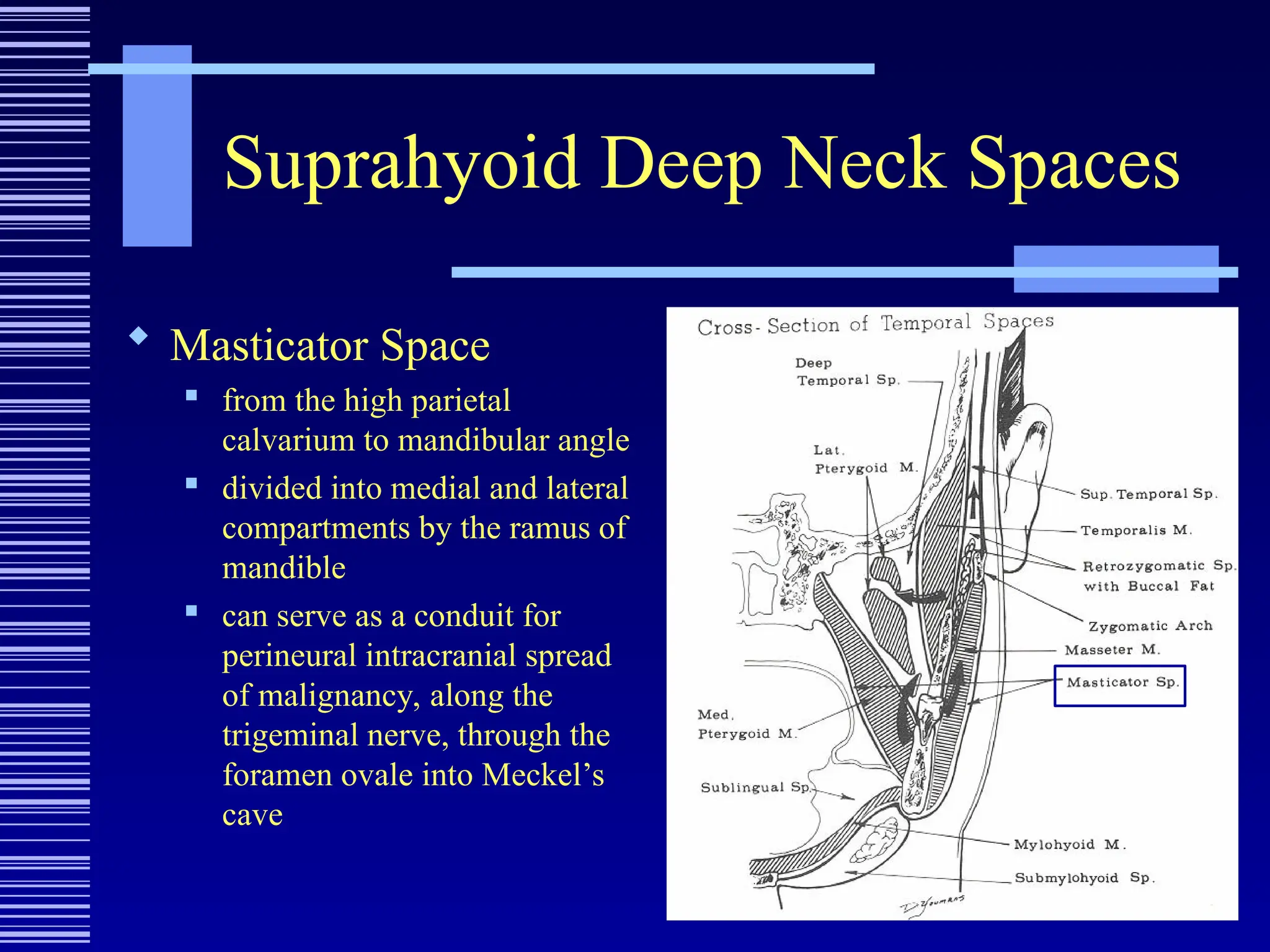
Masticator Space
from the high parietal
calvarium to mandibular angle
divided into medial and lateral
compartments by the ramus of
mandible
can serve as a conduit for
perineural intracranial spread
of malignancy, along the
trigeminal nerve, through the
foramen ovale into Meckel’s
cave
31.
Suprahyoid Neck Spaces
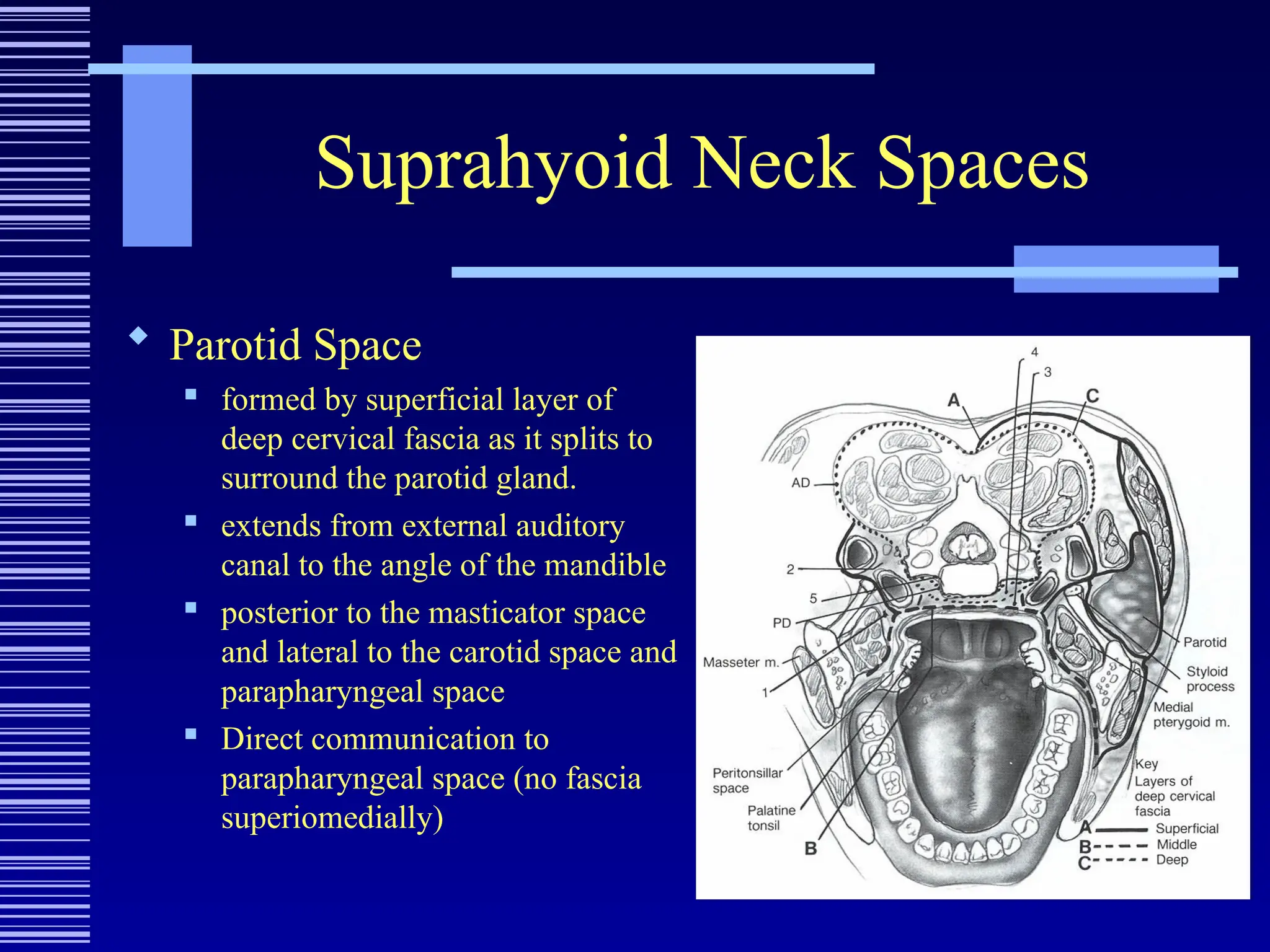
Parotid Space
formed by superficial layer of
deep cervical fascia as it splits to
surround the parotid gland.
extends from external auditory
canal to the angle of the mandible
posterior to the masticator space
and lateral to the carotid space and
parapharyngeal space
Direct communication to
parapharyngeal space (no fascia
superiomedially)
32.
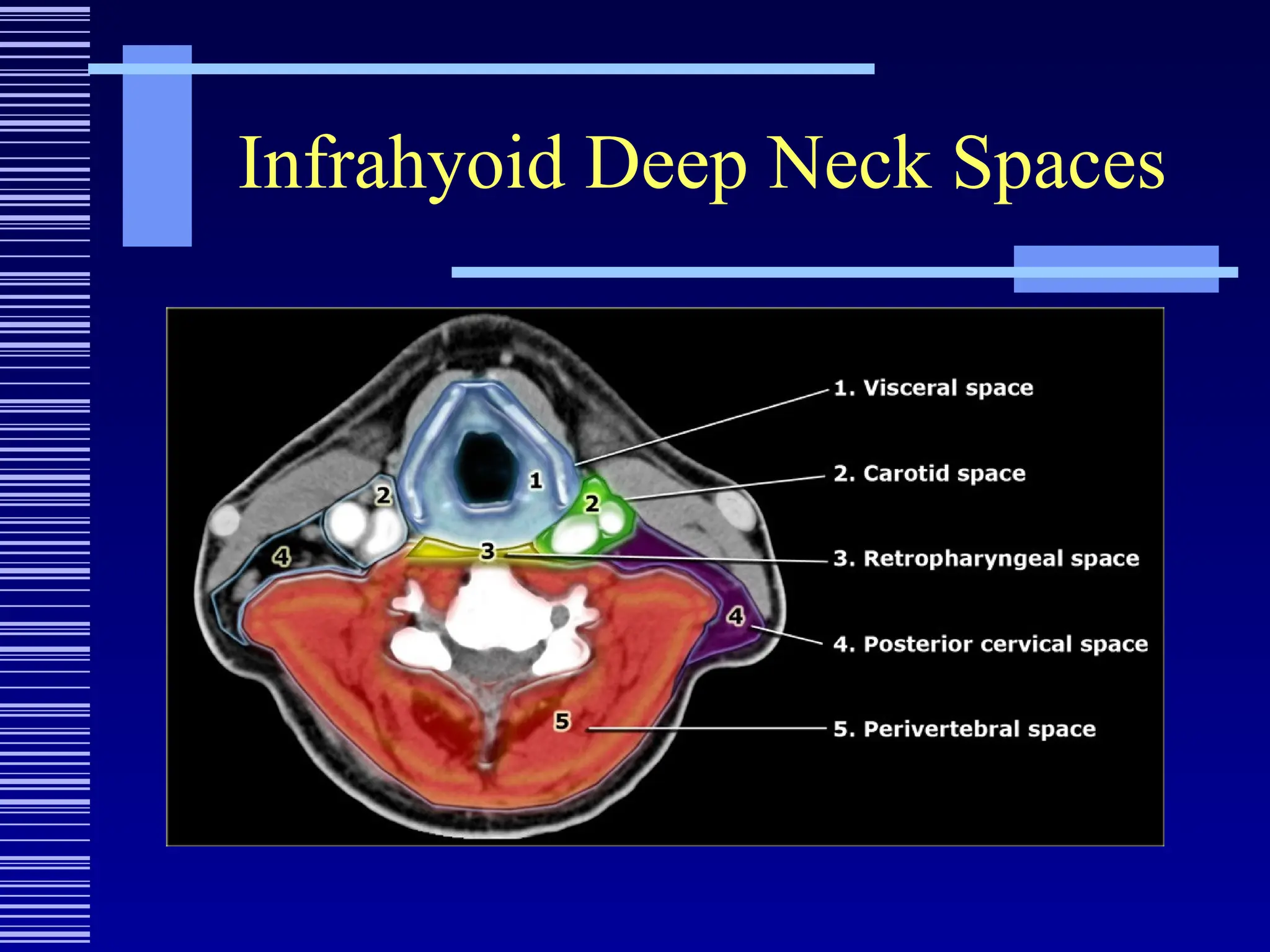
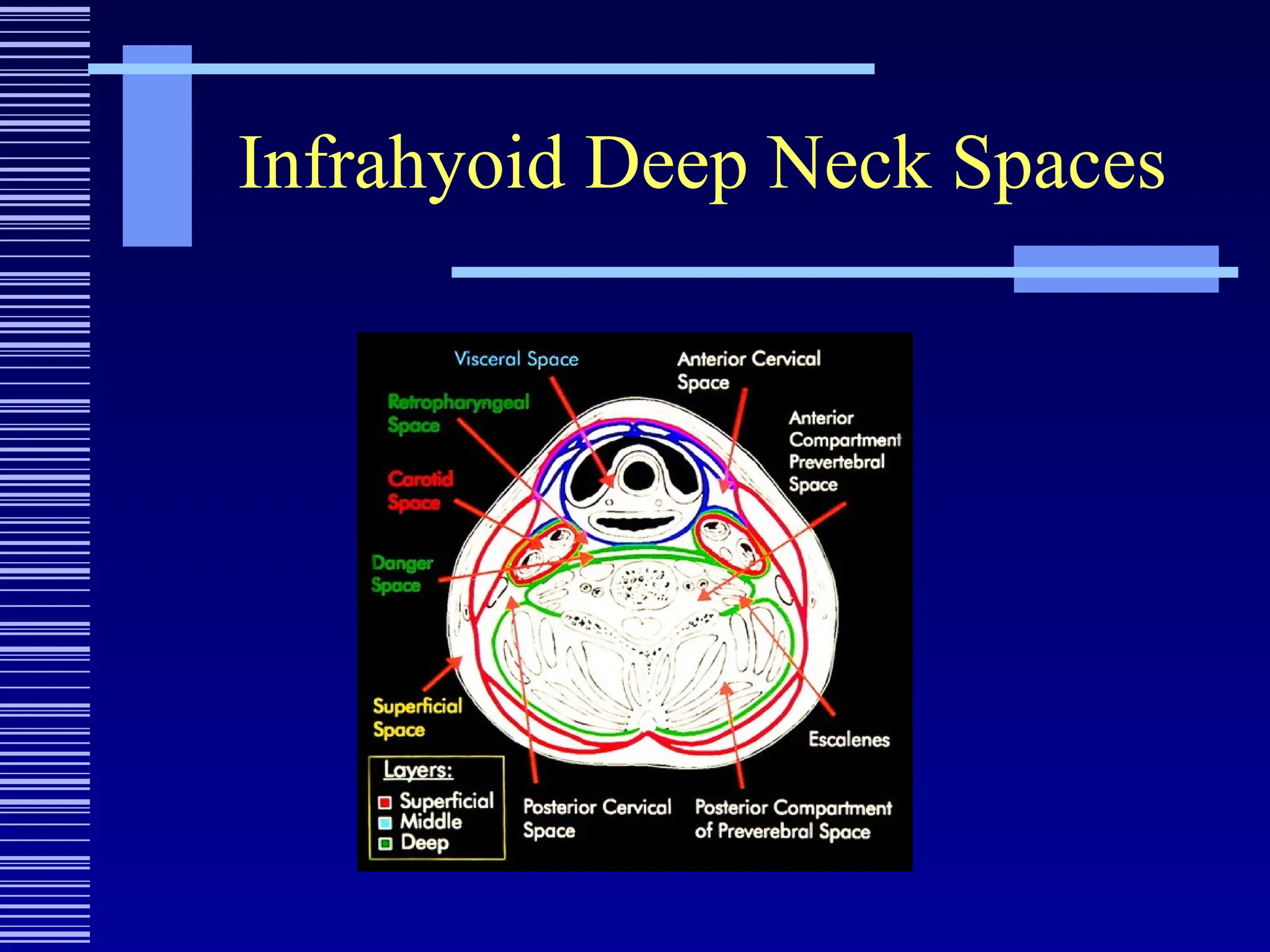
Infrahyoid Deep NeckSpaces
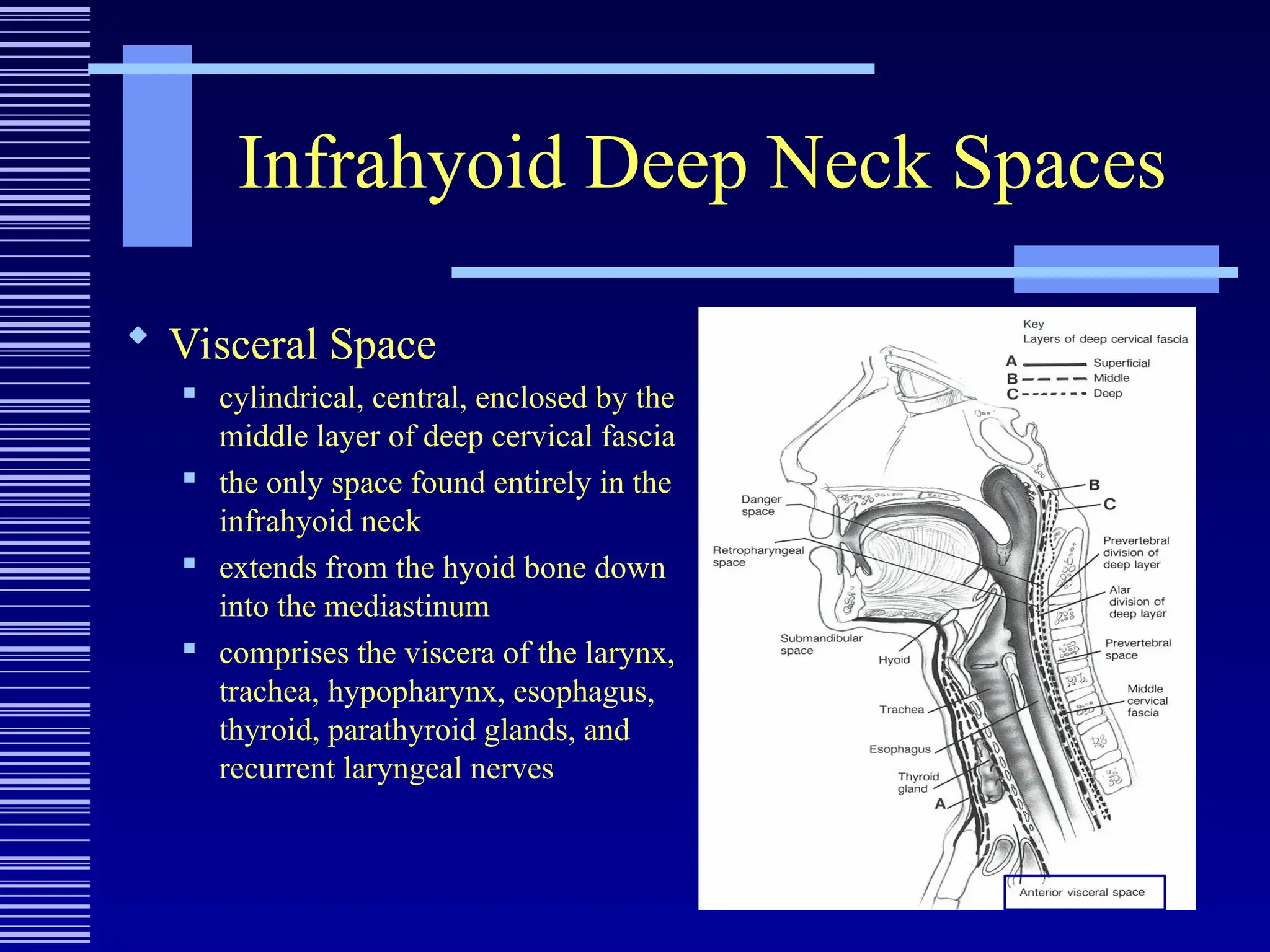
Visceral Space
cylindrical, central, enclosed by the
middle layer of deep cervical fascia
the only space found entirely in the
infrahyoid neck
extends from the hyoid bone down
into the mediastinum
comprises the viscera of the larynx,
trachea, hypopharynx, esophagus,
thyroid, parathyroid glands, and
recurrent laryngeal nerves
Presentation/Origin
Danger Space
Presentation and exam nearly identical to
retropharyngeal space infection
Cause—extension from retropharyngeal,
prevertebral or parapharyngeal space
41.
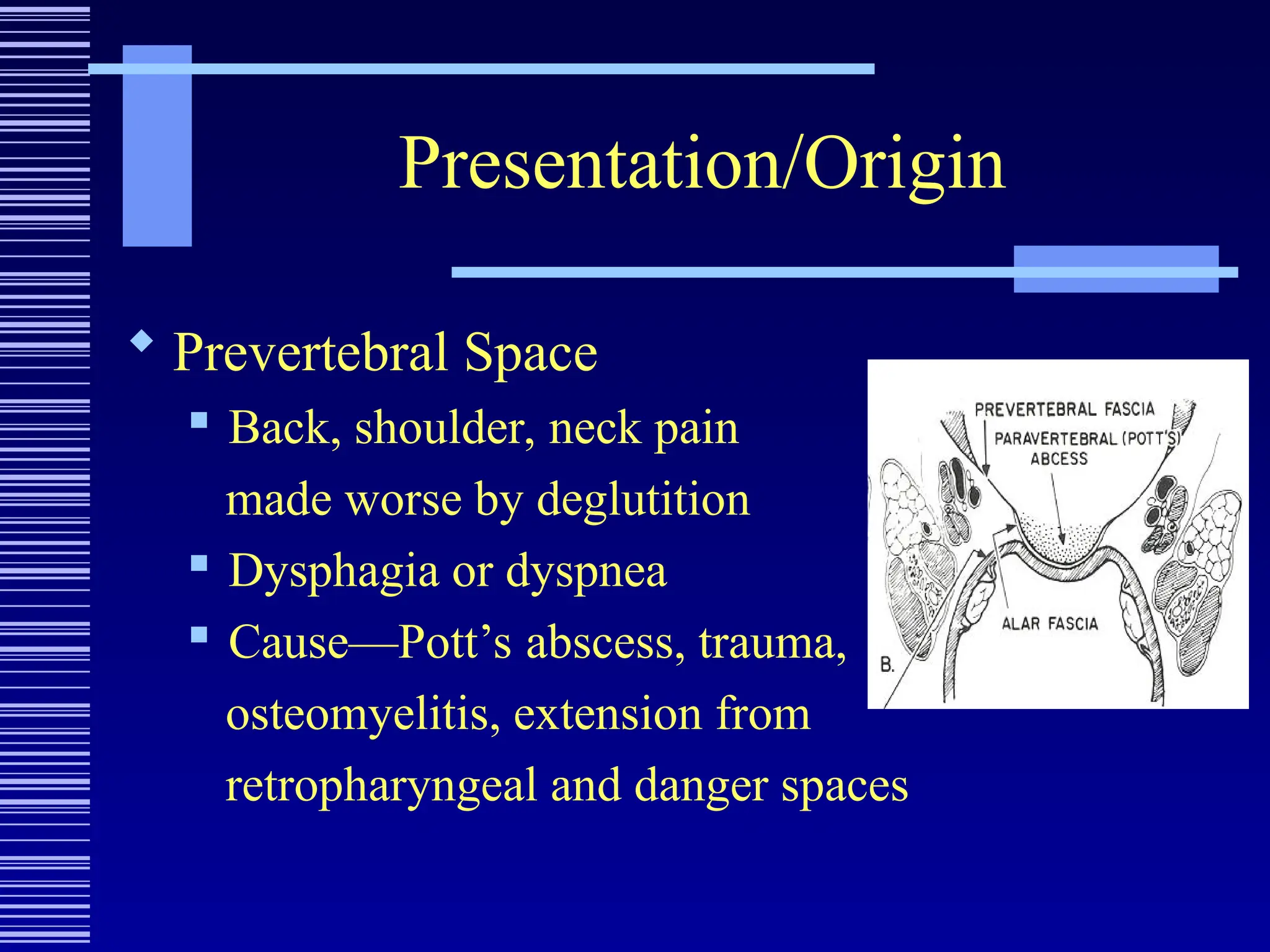
Presentation/Origin
Prevertebral Space
Back, shoulder, neck pain
made worse by deglutition
Dysphagia or dyspnea
Cause—Pott’s abscess, trauma,
osteomyelitis, extension from
retropharyngeal and danger spaces
42.
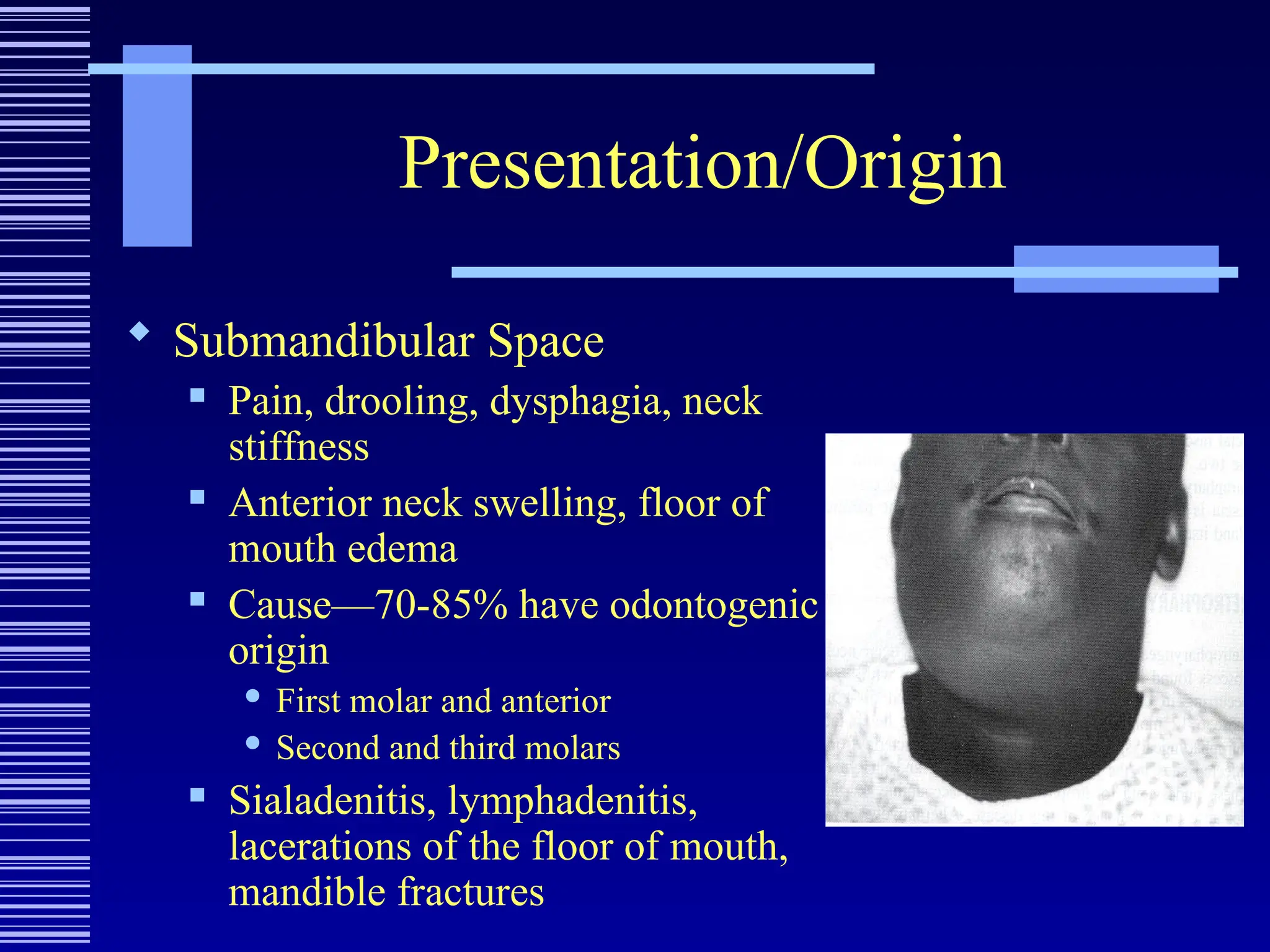
Presentation/Origin
Submandibular Space
Pain, drooling, dysphagia, neck
stiffness
Anterior neck swelling, floor of
mouth edema
Cause—70-85% have odontogenic
origin
First molar and anterior
Second and third molars
Sialadenitis, lymphadenitis,
lacerations of the floor of mouth,
mandible fractures
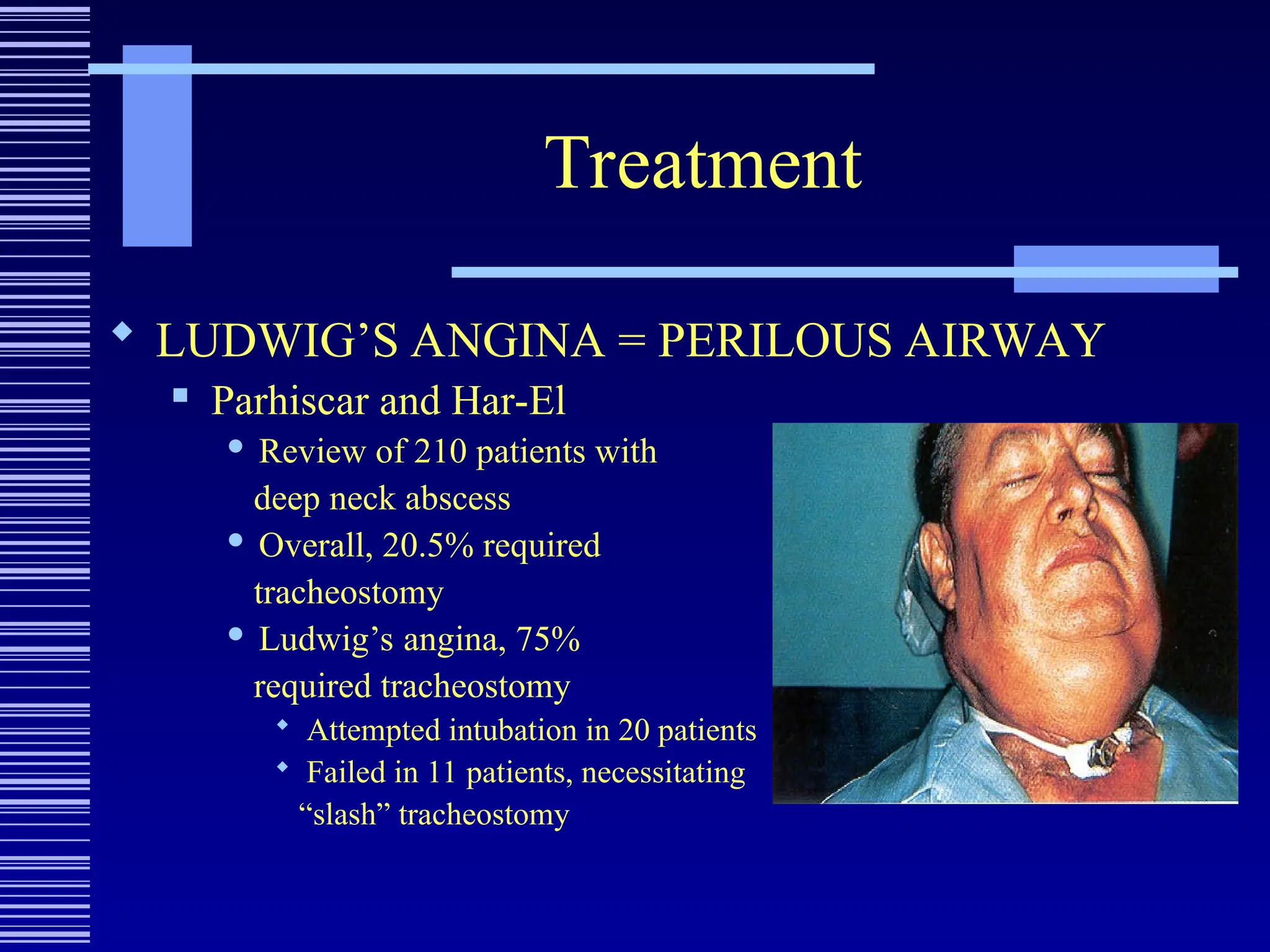
43.
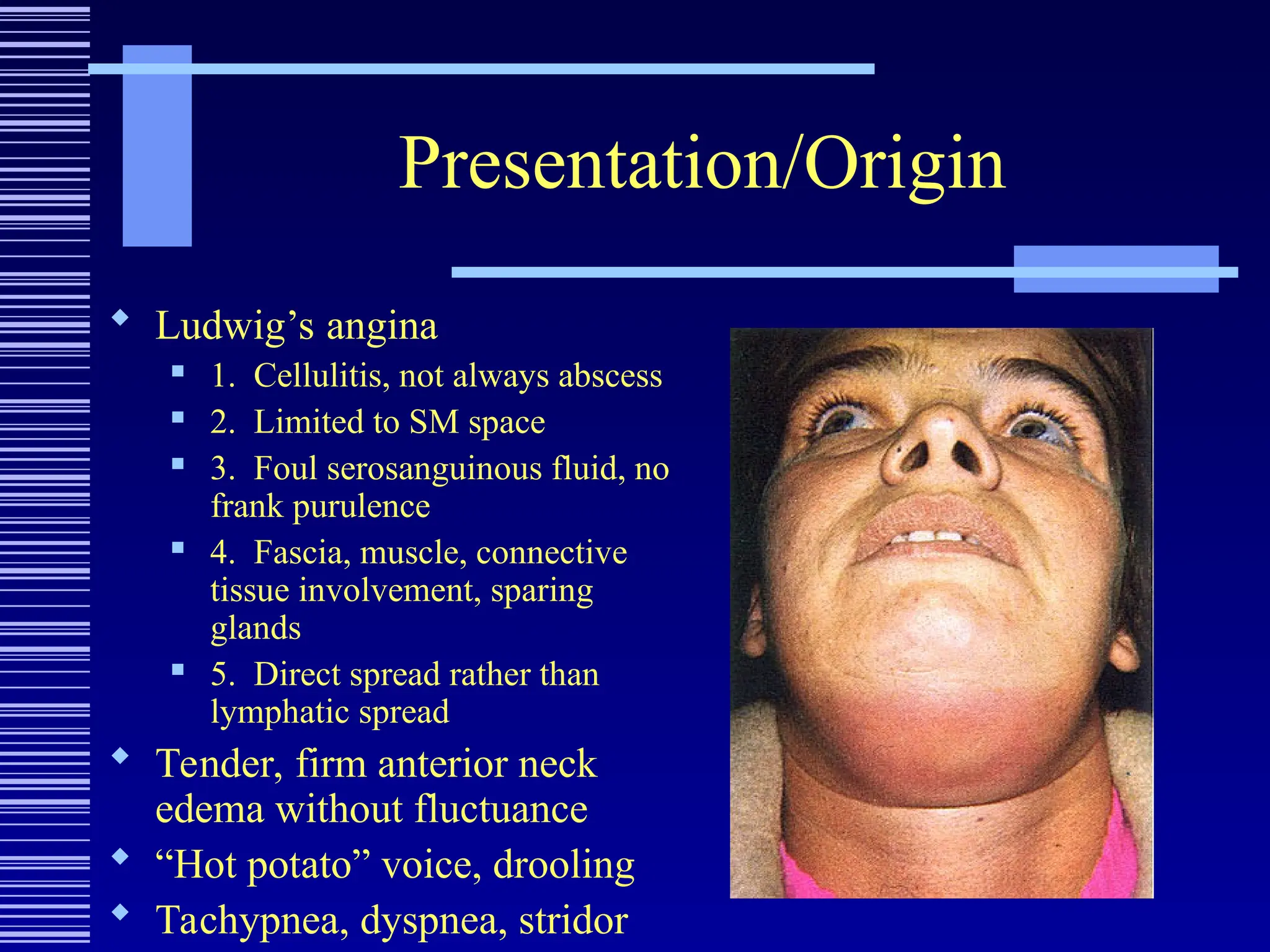
Presentation/Origin
Ludwig’s angina
1. Cellulitis, not always abscess
2. Limited to SM space
3. Foul serosanguinous fluid, no
frank purulence
4. Fascia, muscle, connective
tissue involvement, sparing
glands
5. Direct spread rather than
lymphatic spread
Tender, firm anterior neck
edema without fluctuance
“Hot potato” voice, drooling
Tachypnea, dyspnea, stridor
44.
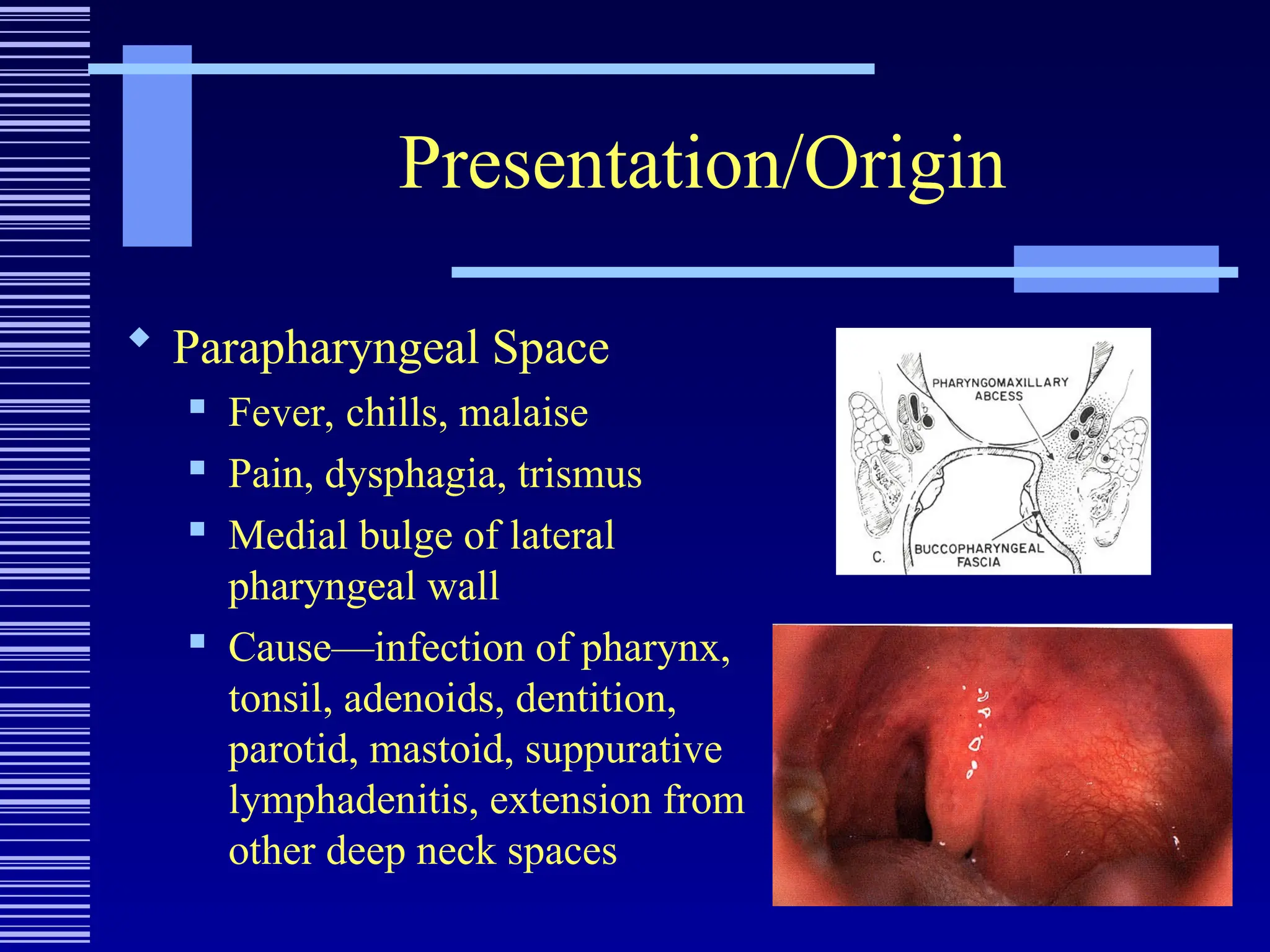
Presentation/Origin
Parapharyngeal Space
Fever, chills, malaise
Pain, dysphagia, trismus
Medial bulge of lateral
pharyngeal wall
Cause—infection of pharynx,
tonsil, adenoids, dentition,
parotid, mastoid, suppurative
lymphadenitis, extension from
other deep neck spaces
45.
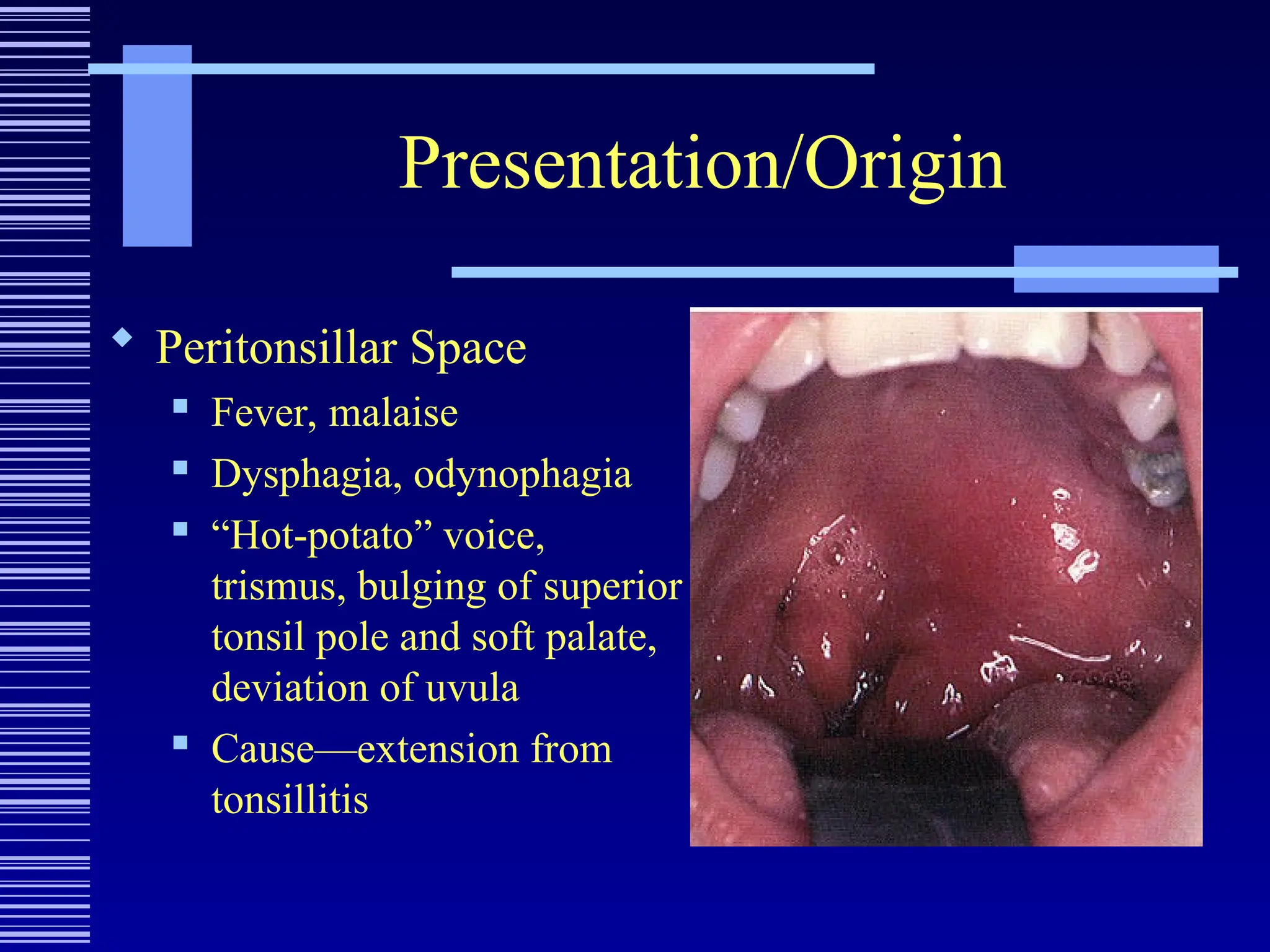
Presentation/Origin
Peritonsillar Space
Fever, malaise
Dysphagia, odynophagia
“Hot-potato” voice,
trismus, bulging of superior
tonsil pole and soft palate,
deviation of uvula
Cause—extension from
tonsillitis
46.
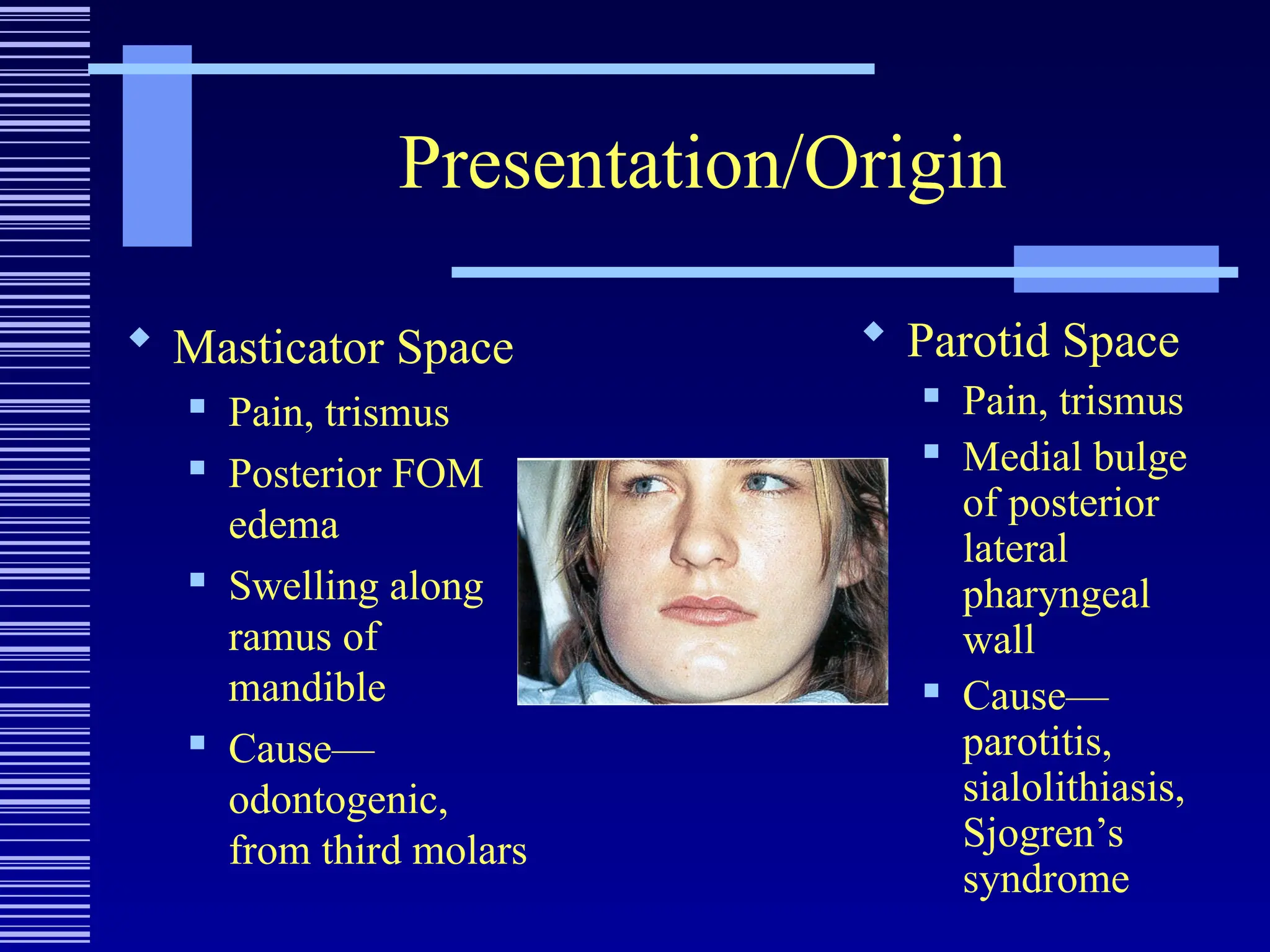
Presentation/Origin
Masticator Space
Pain, trismus
Posterior FOM
edema
Swelling along
ramus of
mandible
Cause—
odontogenic,
from third molars
Parotid Space
Pain, trismus
Medial bulge
of posterior
lateral
pharyngeal
wall
Cause—
parotitis,
sialolithiasis,
Sjogren’s
syndrome
47.
Presentation/Origin
Visceral Space
Hoarseness, dyspnea, dysphagia, odynophagia
Erythema, edema of hypopharynx, may extend to
include glottis and supraglottis
Anterior neck edema, pain, erythema, crepitus
Cause—foreign body, instrumentation, extension
of infection in thyroid
48.
Microbiology
Preantibiotic era—S.aureus
Currently—aerobic Strep species and non-strep
anaerobes
Gram-negatives uncommon
Almost always polymicrobial
Remember resistance
49.
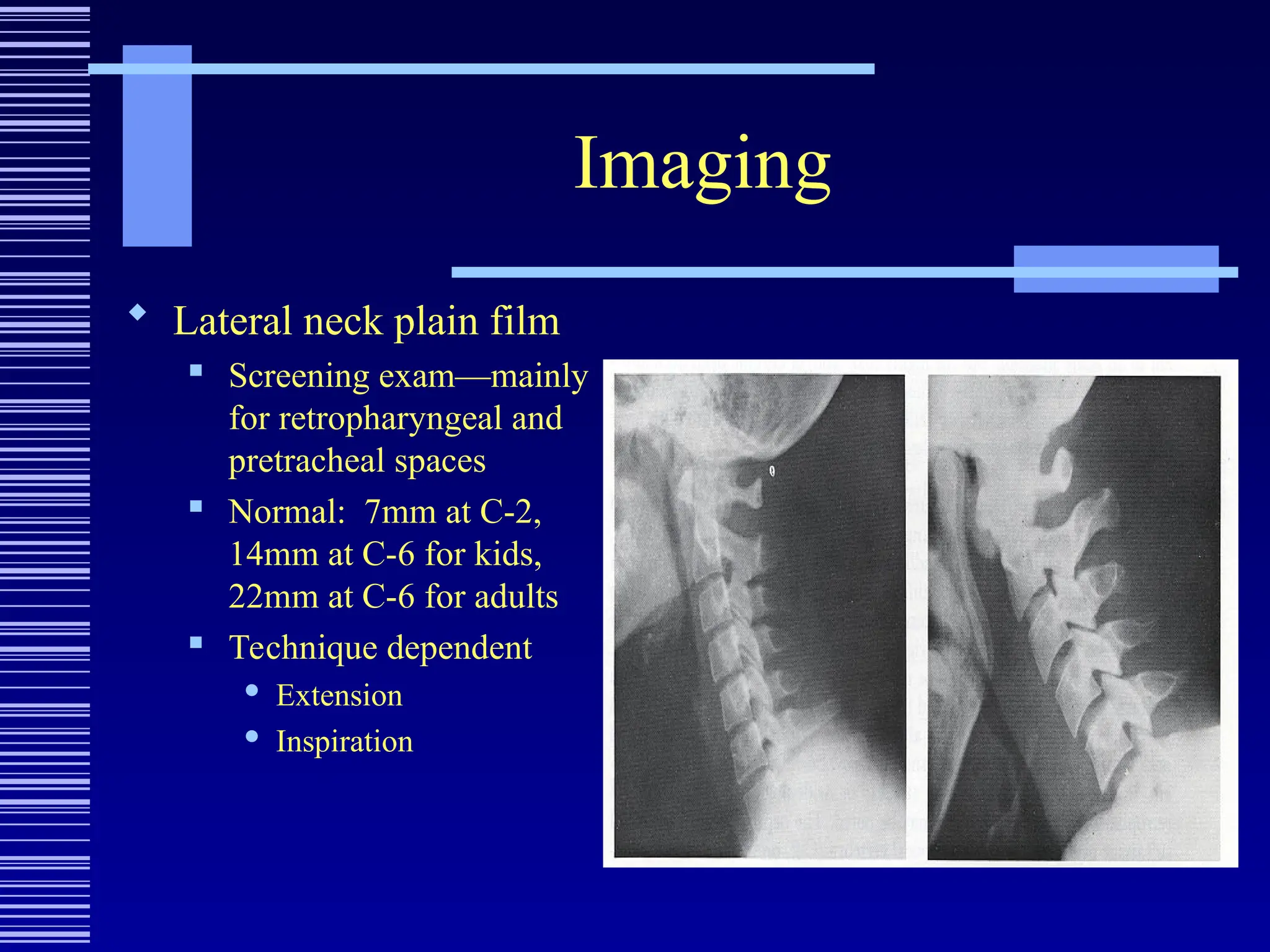
Imaging
Lateral neckplain film
Screening exam—mainly
for retropharyngeal and
pretracheal spaces
Normal: 7mm at C-2,
14mm at C-6 for kids,
22mm at C-6 for adults
Technique dependent
Extension
Inspiration
Complications
Internal JugularVein Thrombosis
Lemierre’s syndrome
F/C, prostration, swelling and pain along SCM
Bacteremia, septic embolization, dural sinus
thrombosis
IV drug abusers
Treatment
IV antibiotic therapy
Anticoagulation?
Ligation and excision
61.
Complications
Carotid ArteryRupture
Mortality of 20-40%
Sentinel bleeds from ear, nose, mouth
Majority from internal carotid, less from external
carotid, and fewest from common carotid
Treatment
Proximal and distal control
Ligation
Patching or grafting?
62.
Complications
Mediastinitis
Mortalityof 40%
Increasing dyspnea, chest pain
CXR = widened mediastinum
Treatment
EARLY RECOGNITION AND INTERVENTION
Aggressive IV antibiotic therapy
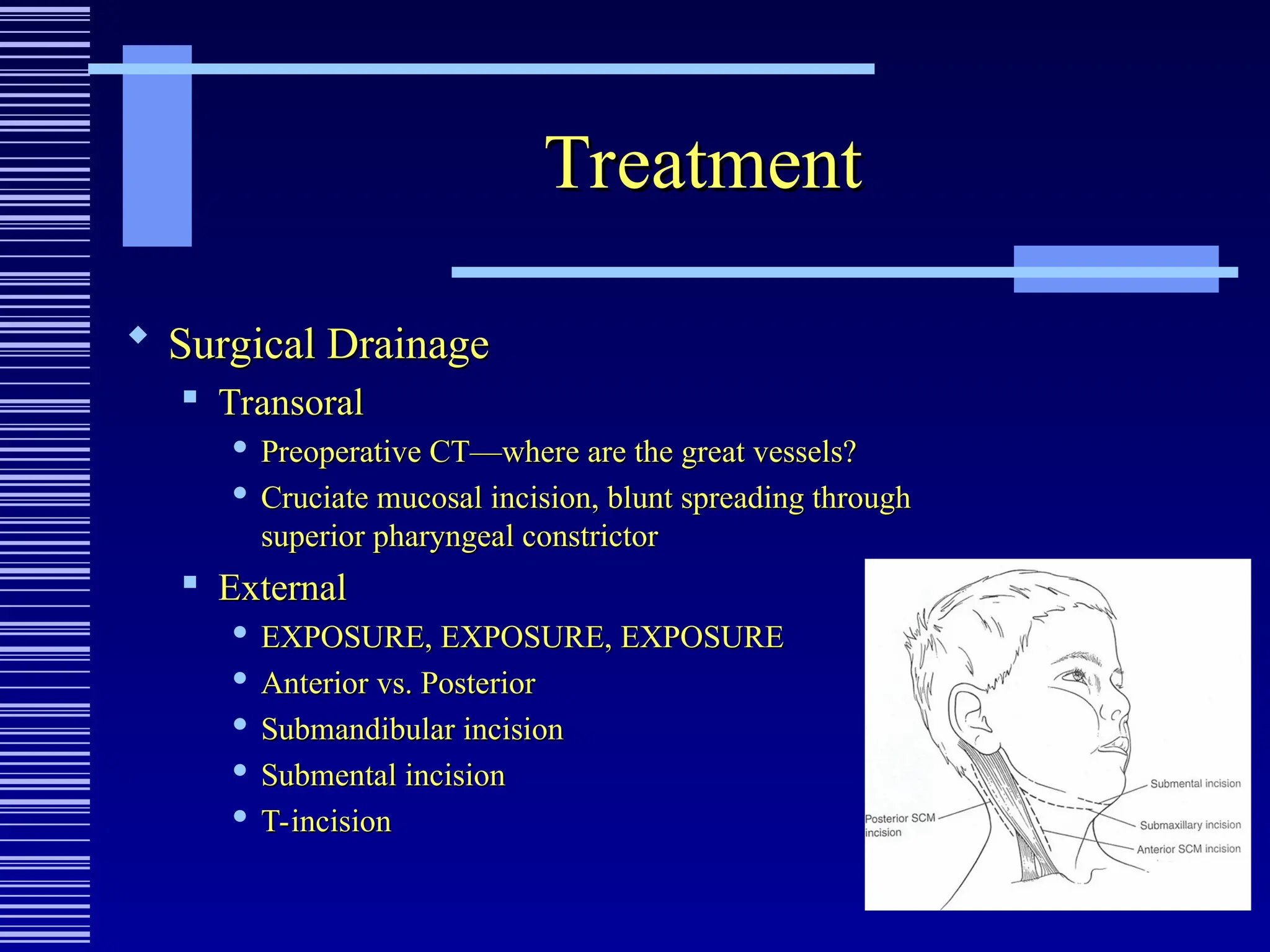
Surgical drainage
Transcervical approach
Chest tube vs. thoracotomy
63.
Special Consideration
RecurrentDeep Neck Space Infection
THINK CONGENITAL ABNORMALITY
Imaging should help make the diagnosis
Nusbaum, et al: 12 cases of recurrent deep neck
infection
Most Common: second branchial cleft cyst
Others: first, third, fourth branchial cleft cysts,
lymphangiomas, thyroglossal duct cysts, cervical
thymic cyst
#12 In 1929, Mosher called this fascia the Lincoln Highway of the neck because all three layers of deep cervical fascia contribute to the carotid sheath. This mental imagery was indicative of an important national event of his time, namely the creation of the first transcontinental paved highway in the United States that ran coast-to-coast from Times Square in New York City west to Lincoln Park in San Francisco.