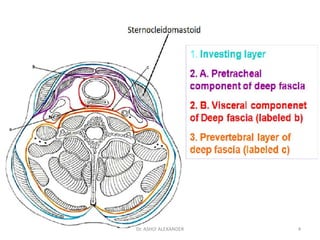
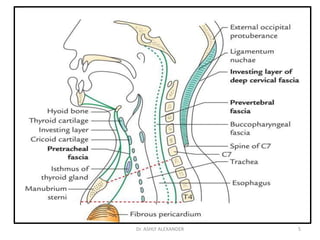
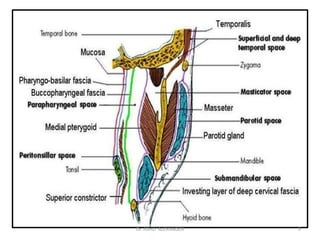
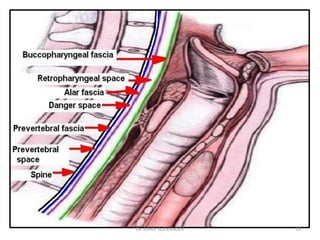
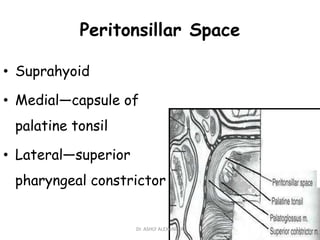
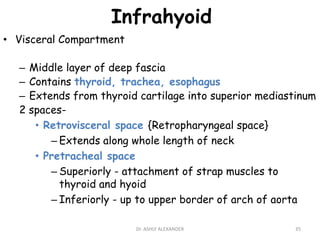
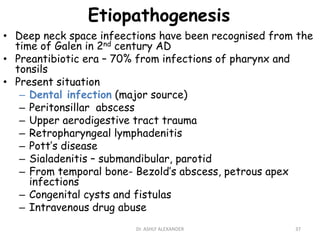
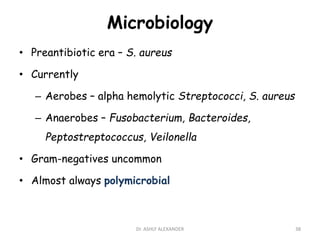
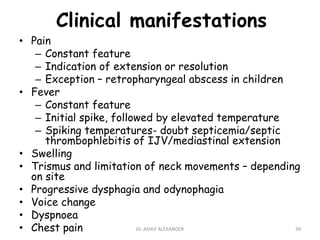
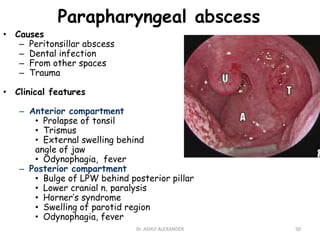
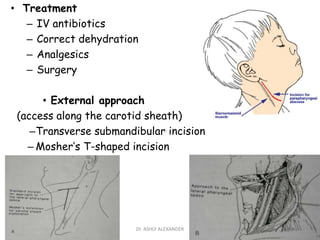
This document discusses deep neck space infections. It begins by describing the anatomy of the cervical fascia and its three layers - superficial, middle, and deep. It then outlines the various deep neck spaces, including those along the entire length of the neck (retropharyngeal, danger, prevertebral, carotid sheath), those above the hyoid bone (submandibular, parapharyngeal), and those below the hyoid bone (retrovisceral, pretracheal). Specific deep neck infections like Ludwig's angina and parapharyngeal abscess are then reviewed in terms of their causes, clinical features, treatment and complications.

























![space infection in oral [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/amithspaceinfectioncopyautosaved-250313174545-e960cdc7-thumbnail.jpg?width=640&height=640&fit=bounds)

































