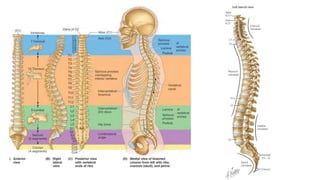
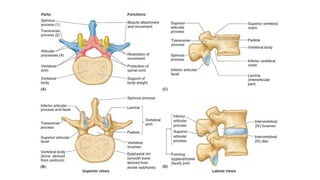
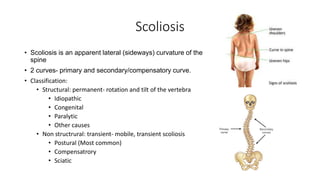
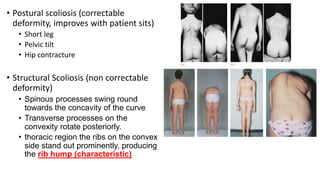





1) Scoliosis is a lateral curvature of the spine that can be structural, caused by conditions like idiopathic scoliosis, or non-structural/postural. Structural scoliosis involves rotation and tilting of vertebrae. 2) The normal spine has four curvatures - thoracic and sacral kyphosis which are primary, and cervical and lumbar lordosis which are secondary. Lordosis bends backward and kyphosis bends forward. 3) Disc prolapse occurs when the nucleus pulposus herniates through weak spots in the annulus fibrosus, potentially compressing spinal nerves. Advanced aging decreases nutrition to discs.