Downloaded 85 times
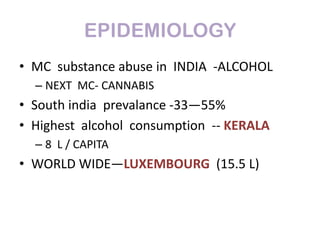
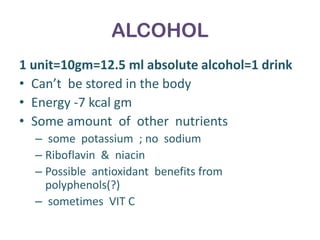
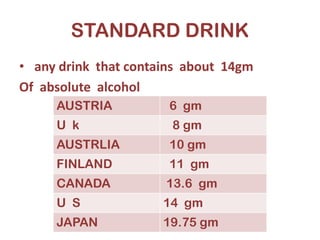
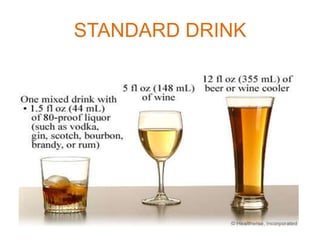



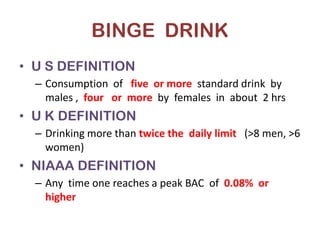
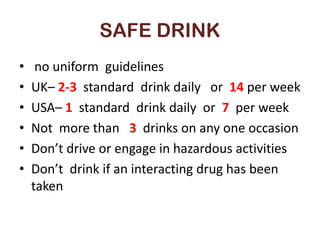
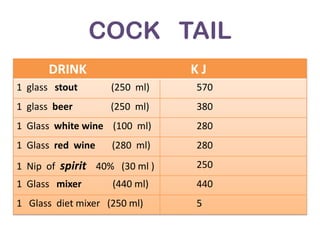
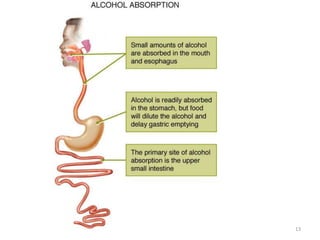
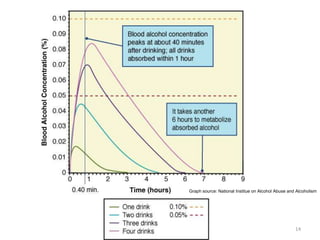
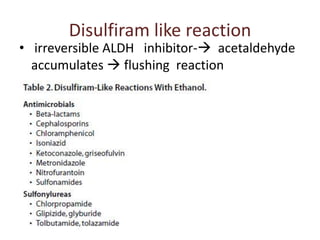
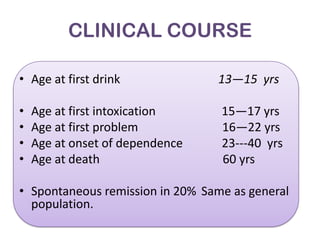



This document provides information on alcohol basics including epidemiology, standard drinks, binge drinking, safe drinking levels, where alcohol comes from, cocktails, factors that influence alcohol absorption, the three pathways of ethanol metabolism, genetic variations in alcohol metabolism, metabolic effects of alcohol, possible hepatotoxic effects of acetaldehyde, drug interactions, diagnosis of alcoholism including questionnaires, the typical clinical course, DSM-IV criteria for alcohol abuse and dependence, and methods for collecting blood and breath samples for alcohol analysis.









































































