Downloaded 159 times
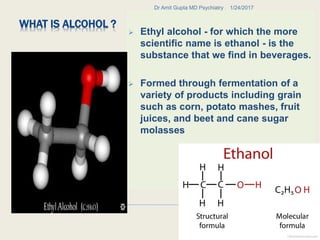

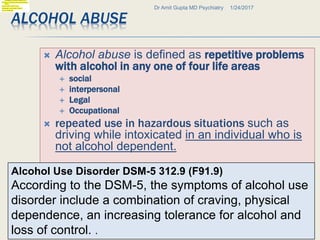
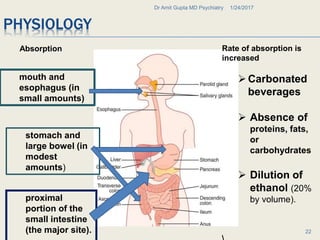
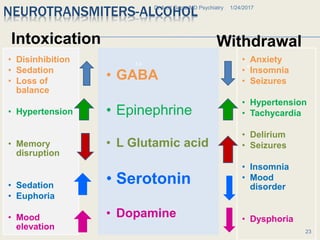
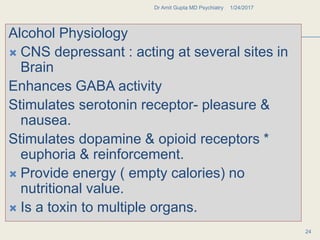
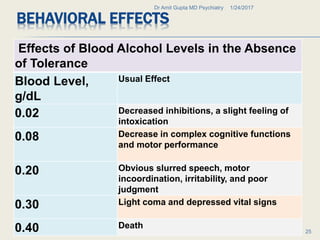
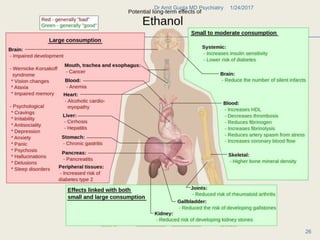
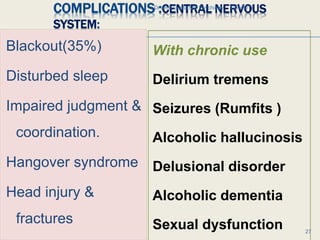
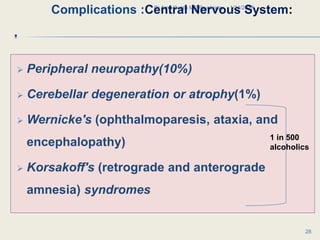
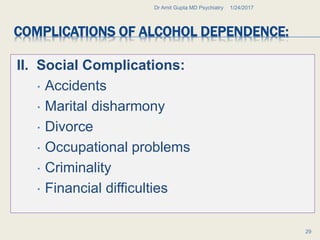


Alcohol abuse has a long history dating back to ancient civilizations. It is formed through fermentation and acts as a central nervous system depressant. Chronic heavy drinking can lead to alcohol use disorder and alcohol dependence. Withdrawal from heavy long-term use can cause serious complications like delirium tremens and seizures. Alcohol abuse is associated with social problems like accidents, violence, and financial issues. It can also damage multiple organ systems and lead to medical conditions like liver disease and neurological impairments.






















































































