The document discusses age-related changes in dental tissues, including enamel, dentin, pulp, and cementum, emphasizing the biological processes and factors influencing aging. Various theories of aging are presented, along with methods of dental age estimation and the significance of these changes in dentistry. The impact of aging on tooth structure, including chemical, physical, and morphological alterations, is explored, highlighting the importance of understanding these changes for dental treatment and forensic evaluation.


![MORPHOLOGICAL METHODS
Morphological methods are based on assessment of ex-vivo teeth for age estimation of adults.
The samples of the extracted tooth can be sectioned or unsectioned and observed with the eye or with
microscope .
The first technique was published by Gustafson in 1950 AND noted the following changes:
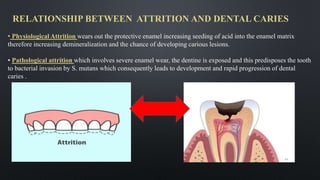
1.Attrition of the incisal or occlusal surfaces due
to mastication [A]
1.Periodontitis [P]—the loss of periodontal attachment
Cementum apposition [C] at the root apex
Transparency of the root [T]
Root resorption [R] amount
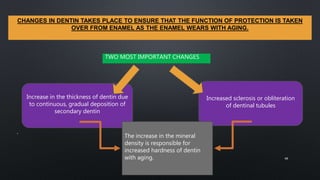
1.Secondary dentin [S]—the amount of coronal secondary
dentine formation
17](https://image.slidesharecdn.com/agechangesintoothaishwarya-210504065810/85/Age-changes-in-tooth-17-320.jpg)












































![Age changes in enamel, dentin and pulp1 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/agechangesinenameldentinandpulp1autosaved-240807163606-82ece9c9-thumbnail.jpg?width=640&height=640&fit=bounds)

































