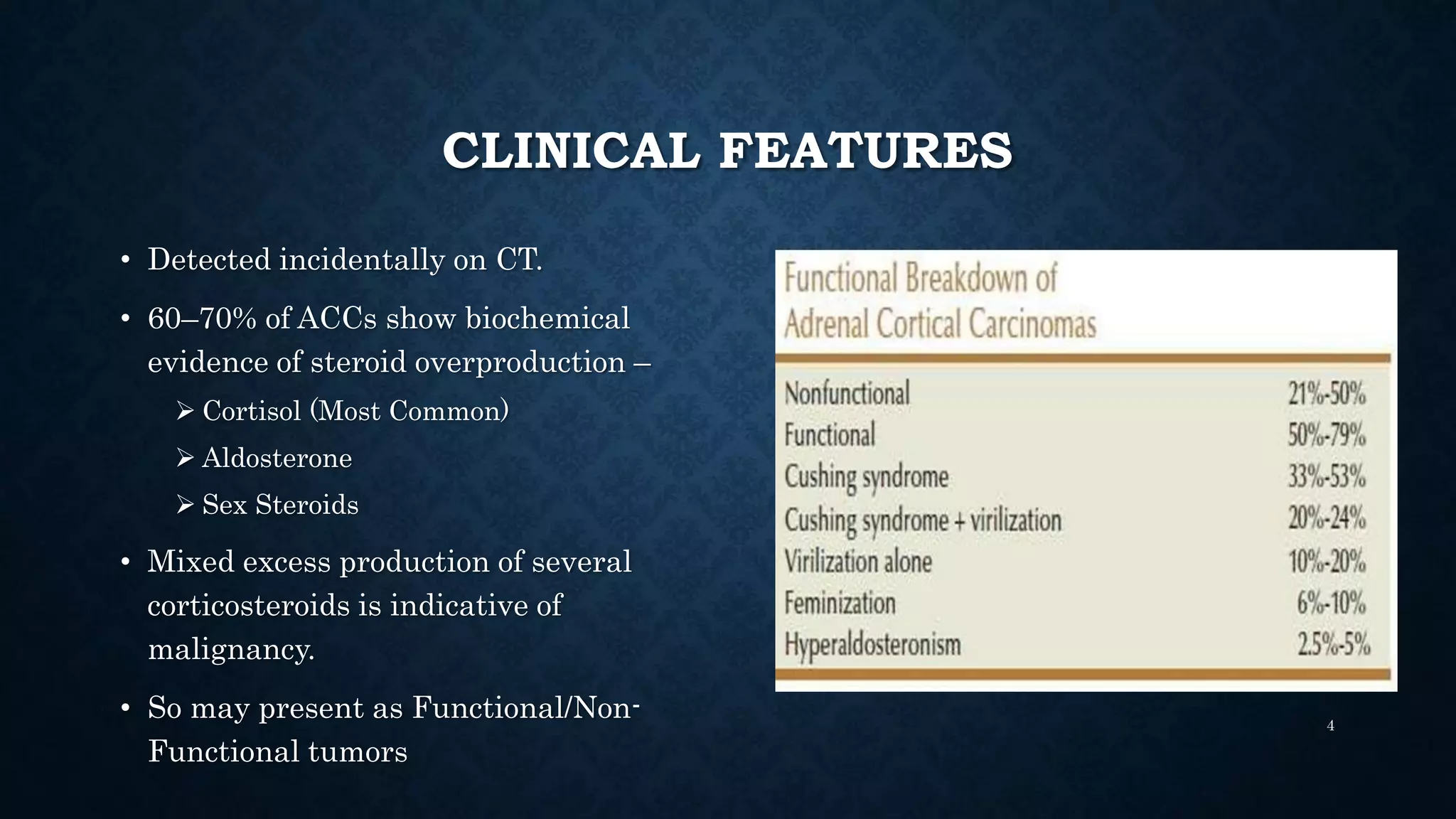
Adrenocortical carcinoma (ACC) is a rare and highly malignant tumor with an annual incidence of 1-2 per million, primarily affecting adults in their fourth to fifth decades and more prevalent in females. Clinical features can include incidental detection on CT scans, hormonal overproduction leading to symptoms of Cushing's syndrome, or non-functional symptoms like abdominal pain and weight loss. Hormonal evaluation, such as the dexamethasone suppression test, is essential for diagnosis and determining the cause of hormonal abnormalities.