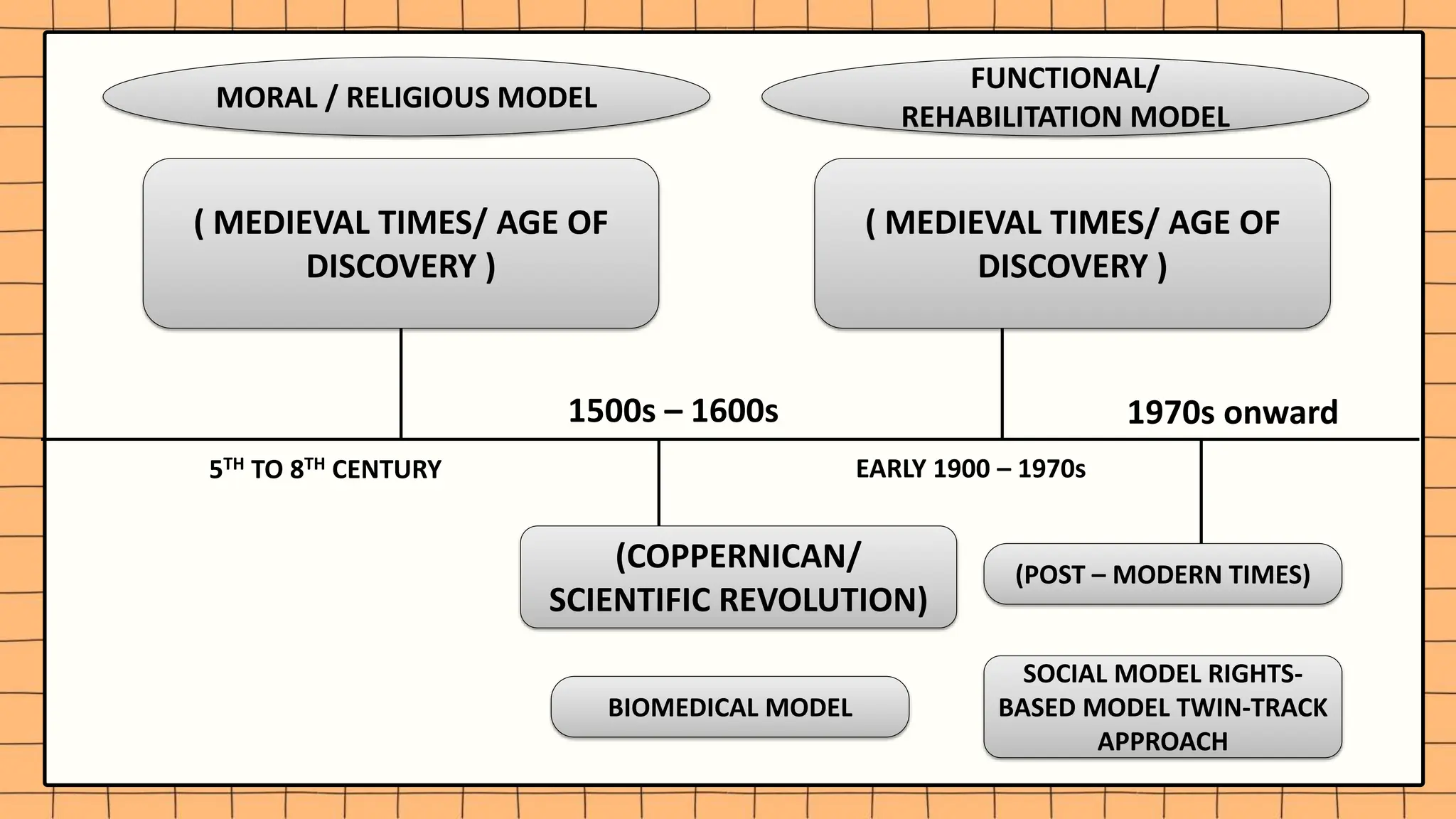
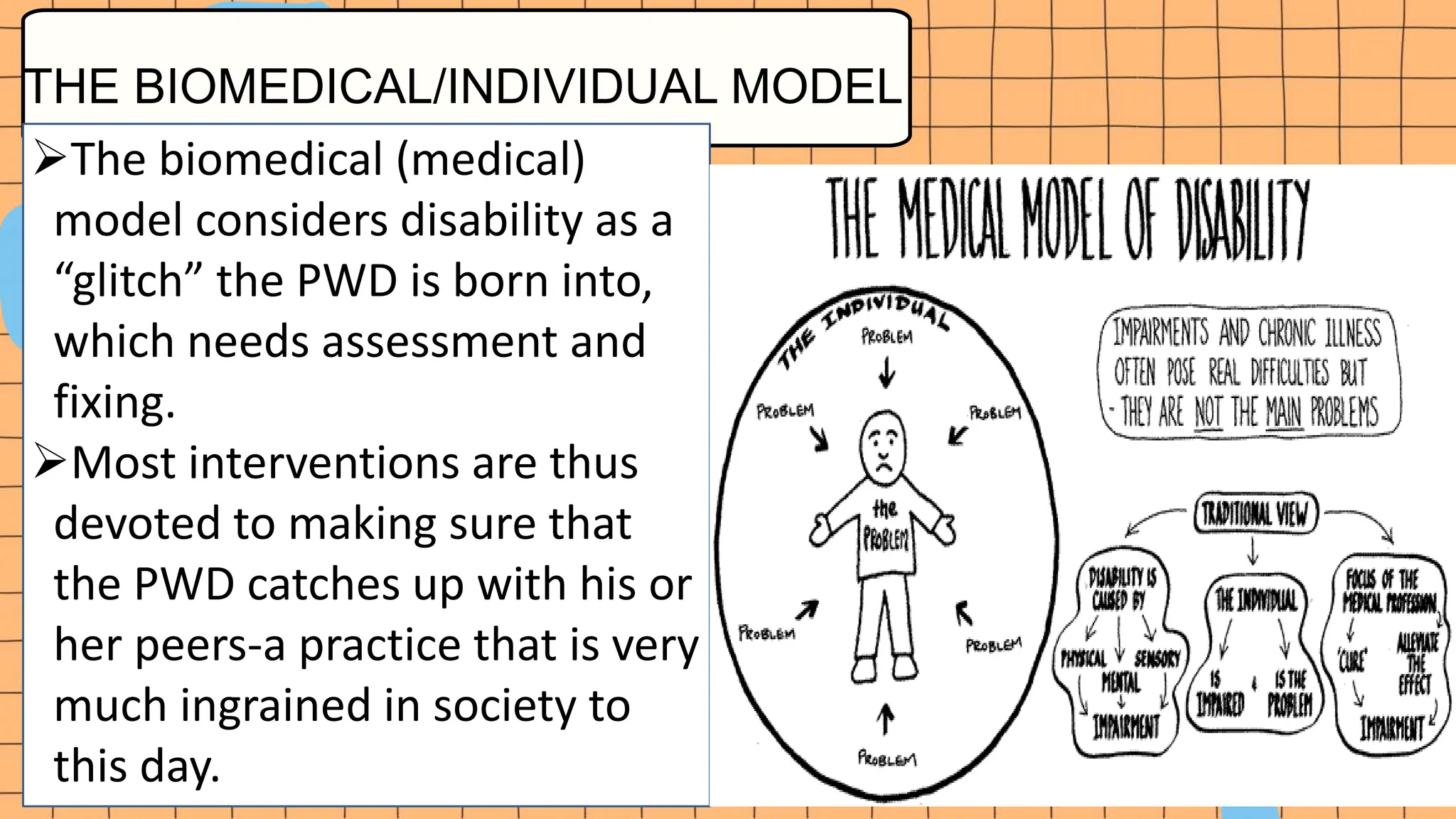
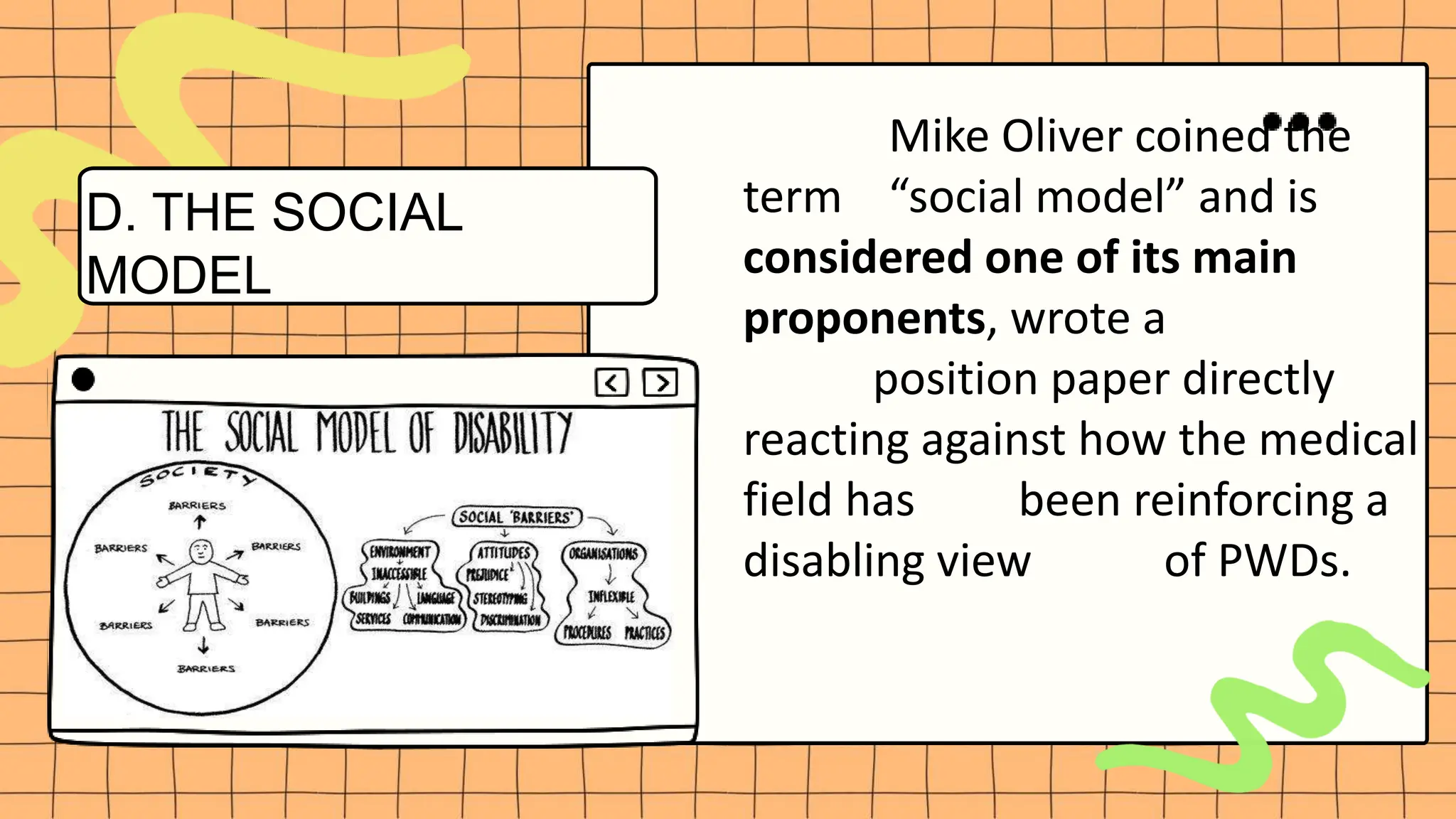
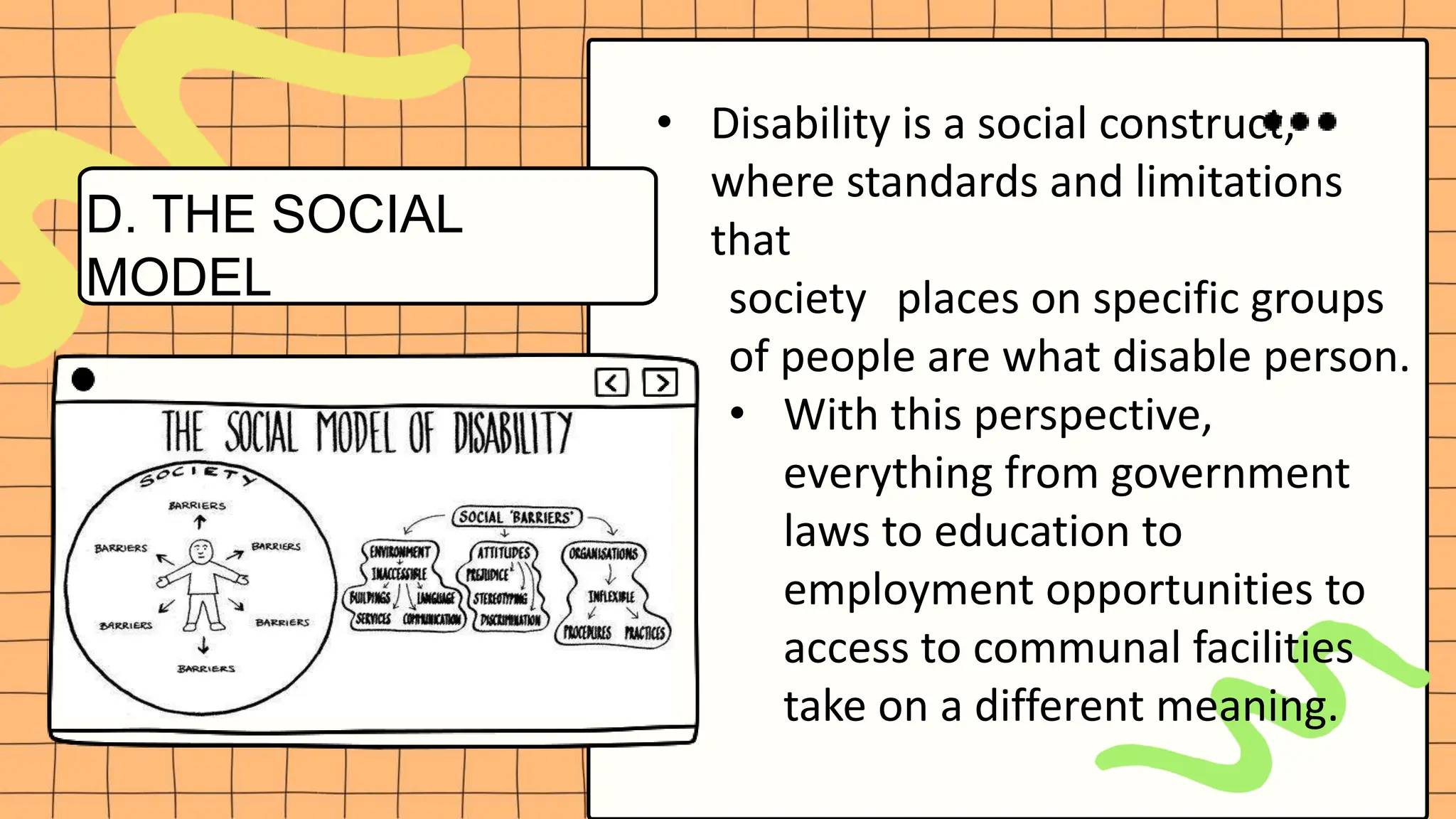
The document discusses various models of disability that have been used throughout history to understand and explain disability. It begins with the moral/religious model used during medieval times which viewed disability as either a blessing or curse from God. It then discusses the biomedical/individual model which sees disability as a medical defect within an individual. The functional/rehabilitation model focuses on rehabilitation to maximize an individual's functioning. The social model frames disability as a social construct caused by societal barriers rather than individual impairments. The rights-based model emphasizes human dignity and rights. Currently, a twin-track approach combining the social and rights-based models is promoted to allow for inclusion while also providing disability-specific support.