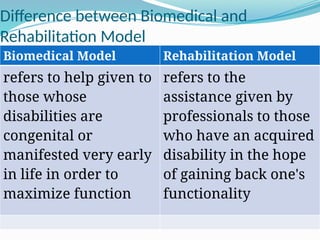
The document outlines various models of disability, including the moral/religious, biomedical, functional/rehabilitation, social, and rights-based models. It discusses each model's perspective on disability and its implications for education and societal attitudes, emphasizing the importance of understanding these frameworks to design effective educational programs for individuals with special needs. The document advocates for a twin track approach that combines the social and rights-based models to ensure holistic support and recognition of individual rights.