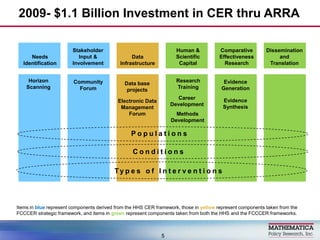
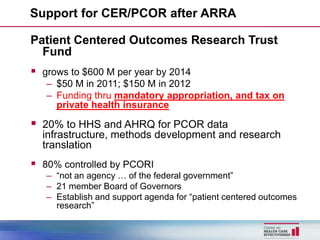
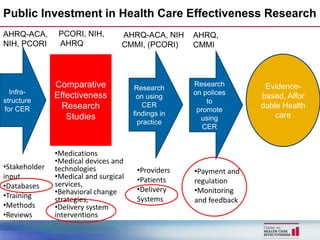
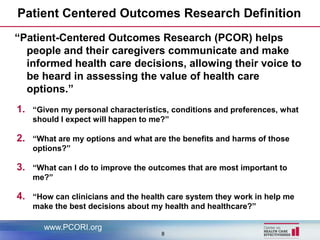
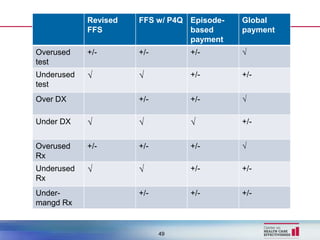

This document discusses accountable care and evidence-based decision making in health care. It provides background on rising health care costs in the US and efforts to promote comparative effectiveness research (CER) and patient-centered outcomes research (PCOR) to address this. It describes the 2009 $1.1 billion ARRA investment in CER and subsequent funding opportunities for PCOR through the Patient-Centered Outcomes Research Trust Fund and the Patient-Centered Outcomes Research Institute (PCORI). The document also discusses challenges of using CER/PCOR findings and the need to incorporate clinical decision-maker perspectives. It analyzes how different payment models like fee-for-service, pay-for-quality programs, episode-based




















![[대한병리학회] 의료 인공지능 101: 병리를 중심으로](https://cdn.slidesharecdn.com/ss_thumbnails/pathology-201106004112-thumbnail.jpg?width=640&height=640&fit=bounds)














































![[Hongsermeier] clinical decision support services amdis final](https://cdn.slidesharecdn.com/ss_thumbnails/hongsermeierclinicaldecisionsupportservicesamdisfinal-131009123754-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Teich] amdis](https://cdn.slidesharecdn.com/ss_thumbnails/teichamdis-131009123653-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




