Contents
Biological approach
Cytokines
Prostaglandin
VitaminD3
PTH
Corticosteroid
Introduction
Biological principles behind accelerated tooth movement
Methods Of Accelerating Tooth Movement
Surgical approach
Interseptal Alveolar Surgery
• Corticotomy
• Micro-osteo-perforation
• Piezocision Technique
3.
Contents
Device-assisted treatment
CyclicalForce Device Effect On Tooth
Movement.
Direct Electric Current Effect On Tooth
Movement.
Photo-biostimulation
Recent Advances
Conclusion
References
5
INTRODUCTION
• Attempts tomodify bone growth, both in terms of amount and direction have been
made since antiquity.
• Initially, orthodontists generally limited their mission to simply move the teeth,
allowing the alveolar bone to remodel naturally, ignoring the alveolar topography.
• However, in the 21st century, orthodontists are forced to widen their horizon of
treatment because more and more adult patients are seeking treatment.
• Limitations in traditional orthodontic techniques and the duration of therapy often
create barriers to the patient’s willingness to accept orthodontic therapy.
6.
6
• A numberof attempts have been made to create different approaches both pre-
clinically and clinically in order to achieve quicker results, but still there are a lot of
uncertainties and unanswered questions towards most of these techniques.
• Most attempts can broadly be categorized into biological, physical, biomechanical,
and surgical approaches.
• Before going into details of these attempts, we need to understand the basics of
orthodontic tooth movements and the factors that initiate inhibition and delayed tooth
movement
7.
7
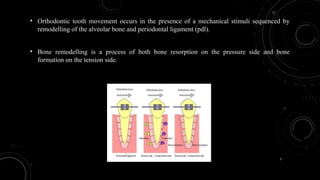
• Orthodontic toothmovement occurs in the presence of a mechanical stimuli sequenced by
remodelling of the alveolar bone and periodontal ligament (pdl).
• Bone remodelling is a process of both bone resorption on the pressure side and bone
formation on the tension side.
8.
8
• The forceapplied on the teeth will cause changes in the microenvironment around
the PDL due to alterations of blood flow, leading to the secretion of different
inflammatory mediators such as cytokines, growth factors, neurotransmitters,
colony-stimulating factors, and arachidonic acid metabolites.
• As a result of these secretions, remodelling of the bone occurs.
10
• Orthodontic appliancesare not intentionally built to activate
or inhibit specific remodelling pathways in specific cells.
• Rather, they are built to generate biomechanical force
systems that produce the desired tooth and jaw movements
needed to establish an ideal occlusion – regardless of the
cellular mediators of the response.
11.
11
• Orthodontists arenow designing innovative appliances and treatments that
optimize skeletal and dental target cell responses that produce controlled, safe
accelerated tooth movement.
• By identifying and harnessing reactions of the target cells one can develop two
different approaches to accelerate the rate of tooth movement:
12.
12
• Directly stimulatethe target cells by artificial, physical, or chemical means to
increase their numbers and their activity.
• Indirectly stimulate the body to recruit and activate more target cells.
In either scenario, identifying the target cells and understanding how they are activated
is crucial.
13.
13
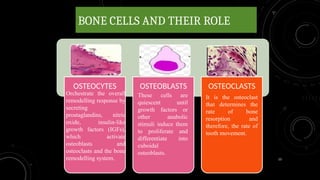
BONE CELLS ANDTHEIR ROLE
OSTEOCYTES OSTEOBLASTS OSTEOCLASTS
Orchestrate the overall
remodelling response by
secreting
prostaglandins, nitric
oxide, insulin-like
growth factors (IGFs),
which activate
osteoblasts and
osteoclasts and the bone
remodelling system.
These cells are
quiescent until
growth factors or
other anabolic
stimuli induce them
to proliferate and
differentiate into
cuboidal
osteoblasts.
It is the osteoclast
that determines the
rate of bone
resorption and
therefore, the rate of
tooth movement.
14.
14
BIOLOGY OF TOOTHMOVEMENT
Bone is the direct
target of
mechanical force
Periodontal ligament
is the direct target of
mechanical force
2 SCHOOLS OF
THOUGHT
15.
15
DIRECT VIEW MODEL
•Compression stress generated in the direction of tooth movement directly
stimulates osteoclasts and tension stress in the opposite direction of tooth
movement directly stimulates osteoblasts.
• Under this assumption, osteocytes may play a significant role by coordinating
osteoclast and osteoblast activity
16.
16
Evidence against thisproposal.
• First, bone does not recognize static forces such as orthodontic forces.
• Second, the lack of movement of implants and ankylosed teeth in response to orthodontic
forces argues against the claim that bone is the target of orthodontic forces.
• Third, in experiments where bone is loaded directly, without interference of the pdl,
compression stresses stimulate bone formation, not bone resorption.
17.
17
INDIRECT VIEW OFTOOTH MOVEMENT
• PDL will exhibit areas of compression and tension in response to the application of
orthodontic forces.
• Distribution of these areas varies depending on the different types of tooth movement,
which in turn are controlled by the magnitude of the force and the moment applied to
the tooth.
18.
18
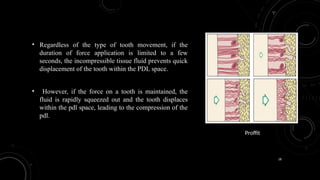
• Regardless ofthe type of tooth movement, if the
duration of force application is limited to a few
seconds, the incompressible tissue fluid prevents quick
displacement of the tooth within the PDL space.
• However, if the force on a tooth is maintained, the
fluid is rapidly squeezed out and the tooth displaces
within the pdl space, leading to the compression of the
pdl.
Proffit
19.
19
• The immediateresult of this displacement is the constriction of blood vessels in the
compression site.
• Depending on the magnitude of pressure and level of blood flow reduction, some of the
cells will go through apoptosis, while some cells will die non-specifically, resulting in
areas of necrosis.
• These sequences of events lead to an aseptic, acute inflammatory response with the
early release of chemokines from local cell
20.
20
Schematic representation ofincrease in permeability of vessels, release of
chemokines, expression of adhesion molecules, and recruitment of
inflammatory and precursor cells during early events of orthodontic tooth
movement
21.
21
RECENT TREND
BIPHASIC THEORY-
•The biphasic theory incorporates the latest evidence on the biology of
tooth movement and proposes an initial phase of catabolism in
response to trauma and inflammation, which in turn activates an
anabolic phase.
• Geographically, these catabolic and anabolic responses can overlap
due to extensive coupling of osteoclast and osteoblast activation
22.
22
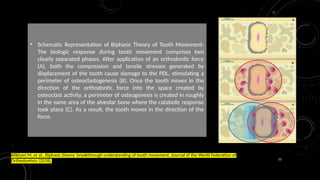
• Schematic Representationof Biphasic Theory of Tooth Movement:
The biologic response during tooth movement comprises two
clearly separated phases. After application of an orthodontic force
(A), both the compression and tensile stresses generated by
displacement of the tooth cause damage to the PDL, stimulating a
perimeter of osteoclastogenesis (B). Once the tooth moves in the
direction of the orthodontic force into the space created by
osteoclast activity, a perimeter of osteogenesis is created in roughly
in the same area of the alveolar bone where the catabolic response
took place (C). As a result, the tooth moves in the direction of the
force.
Alikhani M, et al., Biphasic theory: breakthrough understanding of tooth movement, Journal of the World Federation of
Orthodontists (2018),
23.
23
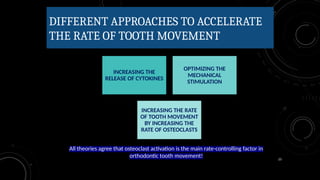
DIFFERENT APPROACHES TOACCELERATE
THE RATE OF TOOTH MOVEMENT
All theories agree that osteoclast activation is the main rate-controlling factor in
orthodontic tooth movement!
INCREASING THE
RELEASE OF CYTOKINES
OPTIMIZING THE
MECHANICAL
STIMULATION
INCREASING THE RATE
OF TOOTH MOVEMENT
BY INCREASING THE
RATE OF OSTEOCLASTS
26
CYTOKINES
• Cytokines familyincludes IL-1, tumor necrosis factors, colony stimulating factors and growth
factors.
• Prominent cytokines that show demonstrated effects on bone remodelling are il-1 iβ, il-6, tnf-
alpha (tnf-α), gm-csf and m-csf.
• These cytokines have been shown to stimulate bone resorption and induce osteoclast
proliferation.
• M-csf is the most potent in stimulating bone-marrow cells to produce osteoclasts.
27.
27
• High concentrationof cytokines such as interleukins IL-1, IL-2, IL-3 IL-6, IL-
8, and tumour necrosis factor alpha (TNF) were found to play a major role in
bone remodelling; moreover, interleukin-1 (IL-1) stimulates osteoclast function
through its receptor on osteoclasts.
• Mechanical stress due to orthodontic treatment increased the production of
prostaglandin pg-E and il-1 beta in the periodontal ligaments
28.
28
• These experimentswere done on cats where one canine was tipped distally by 80 g of
force from hours to days, then immuno-histochemistry and micro-photometry
experiments were done to measure the intensity of PGE and IL-1 beta which was
found to be highest on the tension side.
• Other cytokines which are also involved in the acceleration of tooth movement are
RANKL, which is a membrane-bound protein on the osteoblasts that bind to the rank
on the osteoclasts and causes osteoclastogenesis .
29.
29
• On theother hand, osteoprotegerin (OPG) competes with RANKL in binding to
osteoclast to inhibit osteoclast genesis.
• The process of bone remodelling is a balance between (rankl-rank) system and
opg compound.
31
• Kanzaki etal. (2006), with the help of HVI (hemagglutinating-virus of japan) envelope vector
containing pcDNA-mRANKL, transfected the PDL of male wistar rats with the RANKL gene.
They observed a 30-40% increase in the rate of tooth movement, and a high number of
osteoclasts at day 2 after RANKL gene transfer.
• Iglesias-Linares et al. (2011) used a mixed nonviral system to transfect RANKL to the PDL and
observed a higher number of osteoclasts. Their experiments with local gene transfer in
comparison to corticotomies revealed above 40% and 20% acceleration in tooth movement rate
respectively in comparison with conventional mechanics
32.
32
• Juvenile teethmove faster than adults, which is due to the lower amount of
RANKL/ OPG ratio in the gingival crevicular fluid (GCF) in adult patients
measured by the enzyme-linked immunosorbent assay method.
• Also a correlation was found among rank, opg, and root resorption during
orthodontic teeth movement, and patients with root resorption produced a
large amount of rankl in the compressed site
33.
33
PROSTAGLANDIN
• Prostaglandins (pgs)are inflammatory mediator and a paracrine hormone that acts on
nearby cells; it stimulates bone resorption by increasing directly the number of
osteoclasts.
• Experiments done have shown that injections of exogenous pge2 over an extended
period of time caused acceleration of tooth movements in rats
34.
34
• Chemically producedPGE2 has been studied in human trials with split-mouth
experiments in the first premolar extraction cases.
• In these experiments the rate of distal retraction of canines was 1.6-fold faster than the
control side
35.
35
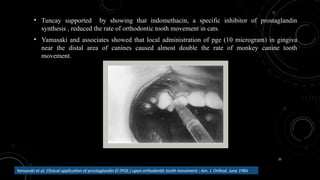
• Tuncay supportedby showing that indomethacin, a specific inhibitor of prostaglandin
synthesis , reduced the rate of orthodontic tooth movement in cats.
• Yamasaki and associates showed that local administration of pge (10 microgram) in gingiva
near the distal area of canines caused almost double the rate of monkey canine tooth
movement.
Yamasaki et al. Clinical application of prostaglandin El (PGE,) upon orthodontic tooth movement ; Am. J. Orthod. June 1984
36.
36
VITAMIN D3
• VitaminD3 (1,25 dihydroxycholecalciferol) is another factor that can affect the
rate of bone remodeling and therefore its possible effect on the rate of tooth
movement has been studied. Vitamin D3 regulates calcium and phosphate serum
levels by promoting their intestinal absorption and reabsorption in the kidneys.
37.
37
• Furthermore, itpromotes bone deposition and inhibits PTH release.
• Based on these mechanisms, one would expect that vitamin d3 should decrease
the rate of tooth movement.
• To the contrary, it has been shown that vitamin d3 can increase the rate of tooth
movement if injected locally.
38.
38
• This effectcan be related to the effect of vitamin D3 on increasing the expression of RANKL
by local cells and therefore activation of osteoclasts.
• Vitamin d metabolite was injected on the pdl of cats for several weeks; it was found that
vitamin d had accelerated tooth movement at 60% more than the control group due to the
increase of osteoclasts on the pressure site as detected histologically
Collins MK, Sinclair PM. The local use of vitamin D to increase the rate of orthodontic tooth movement. Am J Orthod
Dentofacial Orthop. 1988; 94(4):278–84.
39.
39
• Kawakami (1990)reported that a local application of 10-10 mol/L of l,25-(oh)2D3 tends to
prevent mineral apposition at the alveolar bone during OTM.
40.
40
• A comparisonbetween local injection of vitamin D and pges on two different
groups of rats was also investigated (Kale et al. (2004).
• It was found that there is no significant difference in acceleration between the
two groups.
• However, the number of osteoblasts on the pressure side which was injected by
vitamin d was greater than on the pge2 side.
• This indicates that vitamin d may be more effective in bone turnover
41.
41
• Al-hasani (2011)conducted the first human clinical trial on vitamin D by injecting calcitrol (15,
25, or 40 pg/0.2ml calcitrol diluted with 10% dimethyl sulphide) to 15 patients (17-28 years).
• They observed around 51 % increases in tooth movement with the 25 pg group while the other
two groups exhibited 10% acceleration.
• Radiographic evaluation of the dental and paradental tissues revealed no side effects with
calcitrol injection.
42.
42
• Clinical trialwas carried out on 15 subjects who were referred for bilateral
therapeutic extraction of the first premolars followed by canine retraction in the
maxillary arch.
• Vitamin d3 (15 pg/ml) in a vehicle of local anesthetic solution was injected into the
buccal vestibule immediately distal to the canine to be retracted on the experimental
side; on the contralateral side, only local anesthetic solution as control was injected
into the correspnding site on the 7th, 21st, and 47th days of canine retraction.
43.
43
Abhijith shettya ;anand K. Patil; ameet R.; Prabhdeep K. Sandhu. Local infiltration of vitamin D3 does not
accelerate orthodontic tooth movement in humans. Angle orthodontist 2014
• Localized injections of vitamin D3 produced a significantly decreased
rate and amount of tooth movement after a 60-day experimental period.
44.
44
PARATHYROID HARMONE
• PTHis secreted by the parathyroid glands and increases the concentration of serum
calcium by stimulating bone resorption.
• A significant stimulation of the rate of tooth movement by exogenous pth appears to
occur in a dose-dependent manner, but only when it is continuously applied by either
systemic infusion
45.
45
• PTH hasbeen shown to accelerate orthodontic tooth movement on rats, which
was studied by continuous infusion of PTH (1 to 10 μg/100 g of body
weight/day) implantation in the dorsocervical region, and the molars were
moved 2- to 3-fold faster mesially by orthodontic coil spring
Soma S, Iwamoto M, Higuchi Y, Kurisu K. Effects of continuous infusion of PTH
on experimental tooth movement in rats. J Bone Miner Res. 1999; 14(4):546–54
• Studies have shown that locally injected PTH induces local bone resorption, and
it is more advantageous to give PTH locally rather than systemically
Takano-yamamoto T, rodan GA. A model for investigating the local action of bone-acting agents in vivo:
effects of hpth(1–34) on the secondary spongiosa in the rat. Calcif tissue int. 1990; 47(3):158–63.
46.
46
• The developmentof a slow-release application that keeps the local concentration
of PTH for a long time is very efficient.
• The daily injection of pth dissolved in gel medium allowed a slow release which
caused 1.6-fold faster acceleration of teeth compared to daily injection of PTH
dissolved in saline solution which did not cause any acceleration.
47.
47
CORTICOSTEROIDS
• Corticosteroid effectson tooth movement have also been studied.
• While the antiinflammatory effect of corticosteroids can decrease the rate of tooth
movement in the presence of cytokines such as il-6, they may stimulate
osteoclastogenesis and cause osteoporosis
Angeli A, Dovio A, Sartori ML, Masera RG, Ceoloni B, Prolo P, et al. Interactions between glucocorticoids
and cytokines in the bone microenvironment. Ann N Y Acad Sci. 2002;966:97–107.
48.
48
• The effectof corticosteroids on tooth movement can vary based on
the dosage and whether they are administered before the expression
of cytokines (induction period) or after their presence.
• Treatment with triamcinolone acetonide is associated with increased
tooth movement in rabbits via increased resorptive activity in the
alveolar bone.
Abtahi et al; Effect of Corticosteroids on Orthodontic Tooth Movement in a Rabbit Model; The
Journal of Clinical Pediatric Dentistry Volume 38, Number 3/2014
49.
49
• Tooth movementrate increased in the chronic group. The mechanical load
induced an enlargement of the alveolar wall that was less pronounced in both
medicated groups (acute & chronic).
• In the acute group the drug suppressed bone resorption and formation without
mechanical stimulus.
• Force application resulted in significant increase in the relative extension of
resorption and formation in both drug groups; it was particularly pronounced in
the chronic group.
Kalia S, Melsen B, Verna C: Tissue reaction to orthodontic tooth movement in acute and
chronic corticosteroid treatment; Orthod Craniofacial Res , 2004;
50.
50
LIMITATIONS
• First, allthe chemical factors have systemic effects that raise questions about their
safety during clinical application.
• Second, the majority of the factors have a short half-life; therefore, multiple
applications of the chemical are required.
• Furthermore, the administration of a factor in a manner that allows an even distribution
along the alveolar bone surface in the compression site is still a challenge.
55
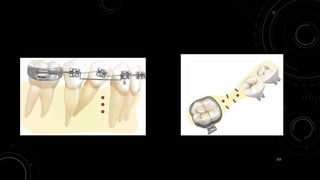
DISTRACTION OF PDL
•In the rapid canine distraction of pdl, the interseptal bone distal to the canine is
undermined surgically at the same time of extraction of the first premolars, thus, this
will reduce the resistance on the pressure site.
• In this concept the compact bone is replaced by the woven bone, and tooth movement
is easier and quicker due to reduced resistance of the bone.
56.
56
• In thistechnique the interseptal bone is undermined 1 to 1.5 mm
in thickness distal to the canine after the extraction of the first
premolar, and the socket is deepened by a round bur to the length
of the canine.
• The objective of these osteotomies is to weaken the interseptal
bone and allow canine to move bodily.
57.
57
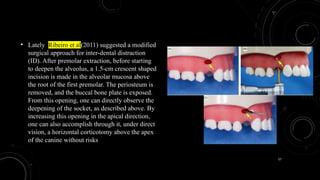
• Lately, Ribeiroet al(2011) suggested a modified
surgical approach for inter-dental distraction
(ID). After premolar extraction, before starting
to deepen the alveolus, a 1.5-cm crescent shaped
incision is made in the alveolar mucosa above
the root of the first premolar. The periosteum is
removed, and the buccal bone plate is exposed.
From this opening, one can directly observe the
deepening of the socket, as described above. By
increasing this opening in the apical direction,
one can also accomplish through it, under direct
vision, a horizontal corticotomy above the apex
of the canine without risks
58.
58
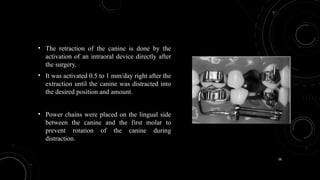
• The retractionof the canine is done by the
activation of an intraoral device directly after
the surgery.
• It was activated 0.5 to 1 mm/day right after the
extraction until the canine was distracted into
the desired position and amount.
• Power chains were placed on the lingual side
between the canine and the first molar to
prevent rotation of the canine during
distraction.
59.
59
• It hasbeen shown that it took 3 weeks to achieve 6 to 7 mm of full retraction of
the canine to the socket of the extracted first premolars
Liou EJ, Huang CS. Rapid canine retraction through distraction of the periodontal ligament.
Am J Orthod Dentofacial Orthop. 1998; 114(4):372–82.
Pre Op Post Op
60.
60
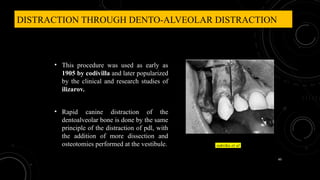
DISTRACTION THROUGH DENTO-ALVEOLARDISTRACTION
• This procedure was used as early as
1905 by codivilla and later popularized
by the clinical and research studies of
ilizarov.
• Rapid canine distraction of the
dentoalveolar bone is done by the same
principle of the distraction of pdl, with
the addition of more dissection and
osteotomies performed at the vestibule. sukrika et al
61.
61
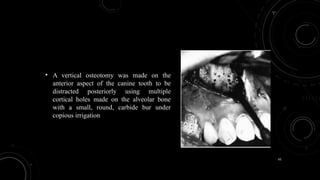
• A verticalosteotomy was made on the
anterior aspect of the canine tooth to be
distracted posteriorly using multiple
cortical holes made on the alveolar bone
with a small, round, carbide bur under
copious irrigation
62.
62
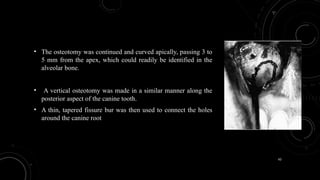
• The osteotomywas continued and curved apically, passing 3 to
5 mm from the apex, which could readily be identified in the
alveolar bone.
• A vertical osteotomy was made in a similar manner along the
posterior aspect of the canine tooth.
• A thin, tapered fissure bur was then used to connect the holes
around the canine root
63.
63
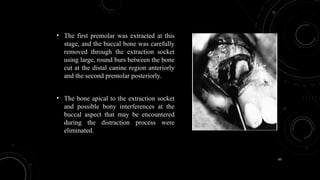
• The firstpremolar was extracted at this
stage, and the buccal bone was carefully
removed through the extraction socket
using large, round burs between the bone
cut at the distal canine region anteriorly
and the second premolar posteriorly.
• The bone apical to the extraction socket
and possible bony interferences at the
buccal aspect that may be encountered
during the distraction process were
eliminated.
64.
64
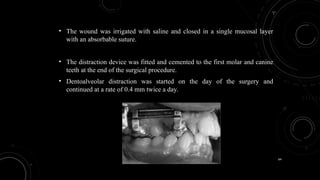
• The woundwas irrigated with saline and closed in a single mucosal layer
with an absorbable suture.
• The distraction device was fitted and cemented to the first molar and canine
teeth at the end of the surgical procedure.
• Dentoalveolar distraction was started on the day of the surgery and
continued at a rate of 0.4 mm twice a day.
65.
65
• In allthe studies done, both techniques accelerated tooth movement with no
evidence of significant root resorption, ankylosis, and root fracture.
• However, there were contradictory results regarding of the electrical vitality
test of the retracted canines. Liou reported 9 out of 26 teeth showed
positive vitality, while sukurica reported that 7 out of 20 showed positive
vitality after the sixth month of retraction.
• So there are still some uncertainties regarding this technique.
66.
66
• The purposeof this study was to test the null hypothesis that duration of orthodontic
treatment can be significantly reduced by accelerating canine retraction using
dentoalveolar distraction.
• The rate of tooth movement and the effects of dad on dento-alveoler and skeletal
structures were evaluated, and these effects were compared with a conventional canine
distalization group
67.
67
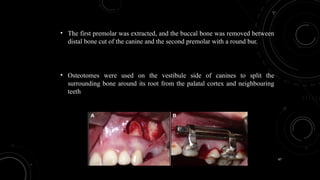
• The firstpremolar was extracted, and the buccal bone was removed between
distal bone cut of the canine and the second premolar with a round bur.
• Osteotomes were used on the vestibule side of canines to split the
surrounding bone around its root from the palatal cortex and neighbouring
teeth
68.
68
• Action wasinitiated after 3 days of latency. The distractor was activated twice per day,
in the morning and in the evening, for a total of about 0.8 mm per day.
69.
69
• No rootresorption was observed in the DAD group.
• Six canines showed widening of the periodontal ligament space at the root apex,
but there was no root resorption in 21 canines.
• No loss of tooth vitality in any maxillary canine was observed in the dad group.
• Moreover, no color change was observed in any teeth before and after dad, and
after 6 months of follow-up.
70.
70
• The meantooth movement (canine retraction) rates were 0.67 +/- 0.14
mm and 0.03 +/- 0.01 mm per day in the DAD group and the DG,
respectively.
• In the dad group, 7.9 +/- 1.49 mm of canine posterior movement was
achieved in 11 days; this is the fastest orthodontic tooth movement in
the literature with no molar anchorage loss.
71.
71
INDICATIONS
• Anterior crowdingwith high anchorage requirement.
• Patients with periodontal problems.
• For alignment of ankylosed teeth.
72.
72
CONTRAINDICATIONS
• Patients withmutilated dentition.
• Dental distraction is not indicated for patients with complex behavioral
problems and known psychological disorders.
• Patients with debilitating diseases.
74
• The pioneerAmerican oral surgeon Hullihan is said to have experimented
with moving teeth after making cuts in alveolar bone in the late 19th century.
• The approach was not widely adopted, as a concern about infections and bone
loss in this pre-antibiotic era
• In the mid-20th century, the german surgeon köle revived the idea that cuts
between teeth could produce faster tooth movement and introduced the term
corticotomy to describe the technique.
75.
75
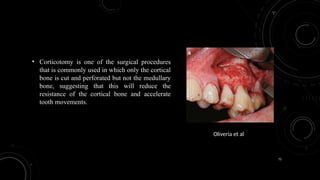
• Corticotomy isone of the surgical procedures
that is commonly used in which only the cortical
bone is cut and perforated but not the medullary
bone, suggesting that this will reduce the
resistance of the cortical bone and accelerate
tooth movements.
Oliveria et al
77
• This techniqueis performed under local anesthesia as a -routine
outpatient procedure.
• A full thickness -mucoperiosteal flap is carefully reflected beyond the
apices of the teeth to -allow adequate decortication
• Selective circumscribing -corticotomy cuts are performed both labially
and -lingually around the teeth to be moved
Selective alveolar
decortication (SAD)
78.
78
DISADVANTAGES
• Risk includesthe possibility of loss of alveolar bone height, which occurs
when corticotomy is done without bone grafting
• Unsightly facial bruising
• Unfavorable changes in the appearance of the gingiva after the extensive
flaps.
• Possibility of gingival stripping
79.
79
Accelerated osteogenic orthodontics
Dr.Thomas wilcko (periodontist) and william wilcko (orthodontist), in 1995 further
modified the corticotomy assisted orthodontic technique with the addition of alveolar
augmentation and named the procedure as periodontally accelerated osteogenic
orthodontics (PAOO) later patented as “wilckodontics”
Dr. Thomas
Dr. William
80.
80
• The techniqueis a combination of selective alveolar decortication in a
linear or punctuate pattern supplemented with bone graft.
• Selective alveolar decortication is performed in the form of line and
cut upto .5mm in depth over all the teeth.
• Then an adequate bone graft is spread over the injured bone.
81.
81
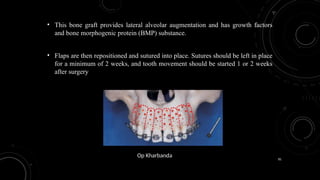
• This bonegraft provides lateral alveolar augmentation and has growth factors
and bone morphogenic protein (BMP) substance.
• Flaps are then repositioned and sutured into place. Sutures should be left in place
for a minimum of 2 weeks, and tooth movement should be started 1 or 2 weeks
after surgery
Op Kharbanda
82.
82
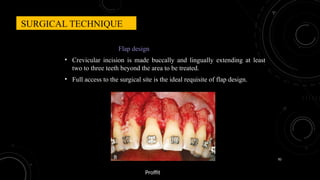
Flap design
• Crevicularincision is made buccally and lingually extending at least
two to three teeth beyond the area to be treated.
• Full access to the surgical site is the ideal requisite of flap design.
SURGICAL TECHNIQUE
Proffit
83.
83
• Gingival collarsare preserved on both palatal and buccal gingiva.
• The ideal design should allow full accessibility to the corticotomy site,
provide full coverage for graft material and enhance aesthetics
wherever required.
84.
84
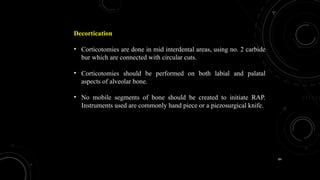
Decortication
• Corticotomies aredone in mid interdental areas, using no. 2 carbide
bur which are connected with circular cuts.
• Corticotomies should be performed on both labial and palatal
aspects of alveolar bone.
• No mobile segments of bone should be created to initiate RAP.
Instruments used are commonly hand piece or a piezosurgical knife.
85.
85
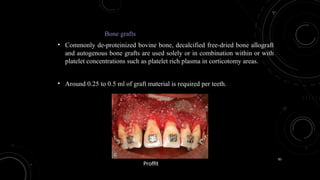
Bone grafts
• Commonlyde-proteinized bovine bone, decalcified free-dried bone allograft
and autogenous bone grafts are used solely or in combination within or with
platelet concentrations such as platelet rich plasma in corticotomy areas.
• Around 0.25 to 0.5 ml of graft material is required per teeth.
Proffit
86.
86
Modifications in grafting
•In certain cases due to thin gingival biotype as well as thin cortical
plate of bone, exposure of root surface can be seen in some cases.
• In such cases use of autogeneous soft grafts such as connective
tissue grafting (gold standard) can be included under full
thickness flap.
• Connective tissue graft can be harvested from palate. Platelet rich
plasma, platelet rich fibrin, and growth factors can also be
included under the flap along with bone grafts to increases the
stability of the graft.
87.
87
Primary closure
• Forpredictable bone augmentation, flap should be closed
without excessive tension.
• Flap is usually sutured at the mid line in the interproximal areas
followed by other areas.
• Suture material of choice is non resorbable sutures. Suture
removal is carried out usually in 7-14 days postoperatively.
88.
88
TECHNIQUE MODIFICATIONS:
• PAOOcan be successfully combined with
gingival augmentation procedures. This is
particularly important to the adult patient who
presents with significant gingival recession. In
these situations, a subepithelial connective
tissue graft is placed over the denuded root
surface in addition to particulate graft
placement. The graft is harvested by removing a
1- to 2-mm thickness of gingival connective
tissue from the elevated palatal flap
89.
89
ADVANTAGE
• Faster toothmovement results in shorter treatment duration and
therefore reduces patient burnout
• Increases the envelope of tooth movement. There is a two- to three-
fold increase in the distance that the teeth can be moved as compared
to traditional orthodontics
• Enhanced post-orthodontic stability due to loss of tissue memory from
high tissue turnover of the periodontium, as well as increased
thickness of the alveolar cortices from the augmentation grafting.
90.
90
DISADVANTAGES
• Invasive procedure.
•Dependent upon patient compliance for timely appliance activation.
• The procedure is technique sensitive, and a lot is dependent upon the
expertise of the surgeon.
• Temporary postoperative oedema.
• Recession and loss of attached gingiva.
• Subcutaneous haematoma of the face.
91.
91
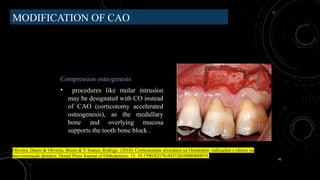
MODIFICATION OF CAO
Compressionosteogenesis
• procedures like molar intrusion
may be designated with CO instead
of CAO (corticotomy accelerated
osteogenesis), as the medullary
bone and overlying mucosa
supports the tooth bone block .
Oliveira, Dauro & Oliveira, Bruno & V Soares, Rodrigo. (2010). Corticotomias alveolares na Ortodontia: indicações e efeitos na
movimentação dentária. Dental Press Journal of Orthodontics. 15. 10.1590/S2176-94512010000400019.
92.
92
• The COconcept is similar to CAO concept, but uses
corticotectomy instead of corticotomy.
• CAO causes movement of teeth in the weakened alveolar
bone but CO causes movement of bone block along with
teeth.
93.
93
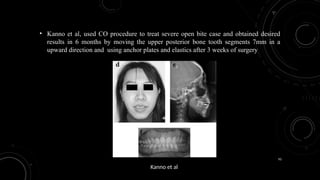
• Kanno etal, used CO procedure to treat severe open bite case and obtained desired
results in 6 months by moving the upper posterior bone tooth segments 7mm in a
upward direction and using anchor plates and elastics after 3 weeks of surgery
Kanno et al
94.
94
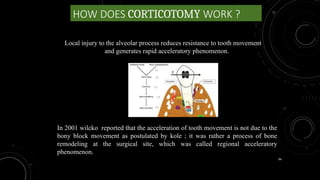
HOW DOES CORTICOTOMYWORK ?
Local injury to the alveolar process reduces resistance to tooth movement
and generates rapid acceleratory phenomenon.
In 2001 wilcko reported that the acceleration of tooth movement is not due to the
bony block movement as postulated by kole ; it was rather a process of bone
remodeling at the surgical site, which was called regional acceleratory
phenomenon.
95.
95
REGIONAL ACCELERATORY PHENOMENON
•The regional acceleratory phenomenon (RAP) is a tissue reaction to a noxious stimulus that
increases the healing capacities of the affected tissues.
• It is typical not only of hard tissues such as bone and cartilage, but also of soft tissues.
• At the tissue level, the RAP is characterized by the production of woven bone, with the
typical unorganized pattern, that will be reorganized into lamellar bone at a later stage.
96.
96
• Herald frostcollectively mentioned the events in physiologic healing and called it as
“the regional acceleratory phenomenon”.
• He was the first to find that surgical wounding of osseous tissues resulted in tissue
stimuli adjacent to the site of the injury, which results in faster than normal regional
regeneration and remodeling process.
• Rap causes bone to heal 2-10 times faster. Following surgical injury in human long
bone, RAP begins within a few hours, maximum action is usually reached in 1-2
months and usually may take 2-4 months to complete.
97.
97
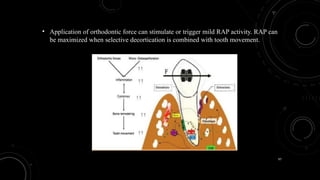
• Application oforthodontic force can stimulate or trigger mild RAP activity. RAP can
be maximized when selective decortication is combined with tooth movement.
99
• Dibart in2009 was among the first to apply the piezocision technique which starts
with primary incision placed on the buccal gingiva followed by incisions by piezo
surgical knife to the buccal cortex and initiate the regional acceleratory phenomenon
without involving palatal or lingual cortex.
• Piezocision can also be combined with invisalign® in selected cases to produce
outcomes that are less time consuming as well as satisfies patient’s desire of aesthetic
appliance
100.
100
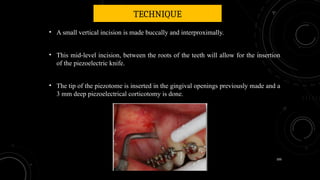
TECHNIQUE
• A smallvertical incision is made buccally and interproximally.
• This mid-level incision, between the roots of the teeth will allow for the insertion
of the piezoelectric knife.
• The tip of the piezotome is inserted in the gingival openings previously made and a
3 mm deep piezoelectrical corticotomy is done.
101.
101
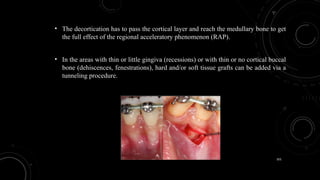
• The decorticationhas to pass the cortical layer and reach the medullary bone to get
the full effect of the regional acceleratory phenomenon (RAP).
• In the areas with thin or little gingiva (recessions) or with thin or no cortical buccal
bone (dehiscences, fenestrations), hard and/or soft tissue grafts can be added via a
tunneling procedure.
102.
102
• The patientis seen every one or two weeks after surgery by the orthodontist in order to
change aligners or activate wires and take advantage of the temporary demineralization
phase created by piezocision™.
• This results in faster tooth movement and early completion of treatment.
• After the 5th or 6th month of treatment, the tooth movement appears to slow down
103.
103
Modified corticotomy/Peizocision avoidsreflecting a flap, using
thin micro-incisions through the facial tissue. A piezoelectric
knife is used to penetrate the cortical bone and extend into the
medullary bone between the teeth.
If a bone graft is desired, a tunnel under the soft tissue is
established, and the graft slurry is placed into the area with a
syringe.
Finished Case Ten months later.
104.
104
CLINICAL APPLICATIONS
• Generalized:if the correction of the malocclusion requires moving all of the teeth in
both maxilla and mandible at the same time.
• Localized: if the malocclusion affects only one part of the dentition or one arch (i.E. An
anterior crowding case with a perfect posterior occlusion, single tooth extrusions
intrusions, etc.)
• Sequential: if the correction of the malocclusion requires a “staged” approach, where
selected areas or segment of the arch are being demineralized at different times during
orthodontic treatment to help achieve specific results.
105.
105
INDICATIONS
1. Class Imalocclusions with moderate to severe crowding (extraction and non extraction)
2. Selected class II malocclusions (end-on)
3. Selected class III malocclusions (dental)
4. Correction of deep bite, correction of open bite
5. Distalization of molars
6. Rapid adult orthodontic treatment
7. Orthodontic treatment with clear aligners,
8. Rapid intrusion and extrusion of teeth
106.
106
CONTRA-INDICATIONS:
1. Medically compromisedpatients
2. Patients taking drugs modifying normal bone physiology (i.E. Biphosphonates)
3. Bone pathology
4. Ankylosed teeth
5. Non-compliant patients
6. Patient and/or operator having a pacemaker or any other active implant.
Potential problems: root injury, infection, mucogingival defects
107.
107
MODIFIED TECHNIQUE
• Toreduce the risk of root damage, Jorge et al in 2013, suggested a method, called MIRO
(Minimally Invasive Rapid Orthodontic procedure) by using metal wire as a guide to
placement of the incisions, and subsequently the corticotomies. He placed metal guides in
between each tooth, perpendicular to the main arch wire, and took digital radiographs, to
ensure that the metal guides did not project over the tooth roots. Once this was confirmed,
incisions and piezoelectric corticotomy was done using the pins as a guide. Clinical results of
a MIRO, maintains the advantages of speedy orthodontics described by Chung et al., but is a
much less traumatic, as it is flapless, reducing both trauma and convalescence. MIRO also
enhances accuracy by relying on radiographic surgical guides that help to make a precise
corticotomy avoiding damage to vital structures and teeth.
108.
108
The radiographic metalguides between each tooth were
positioned and digital radiographies were taken to assure that
the metal pin did not project over the tooth roots
The metal pin allows an accurate mucoperiosteal
incision 2 mm below the papilla. Vertical
corticotomies were performed using an ultrasonic
microsaw OT7.
110
• To furtherreduce the invasive nature of
surgical irritation of bone, a device called
Propel, was introduced by Propel
Orthodontics .
• They called this process as Alveocentesis,
which literally translates to puncturing bone.
• This device comes as ready-to-use sterile
disposable device.
111.
111
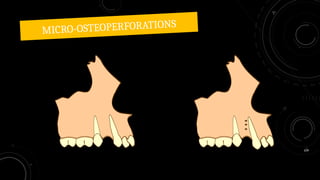
• It hasthe advantage that it does not require periodontal surgery and can be
implemented by orthodontists.
• In this method, special screws supplied by the company are placed through the
gingiva into interproximal alveolar bone and then removed.
• It is said that three such perforations in each interproximal area between teeth are
enough to generate a regional acceleration of bone remodeling and thereby produce
faster tooth movement.
112.
112
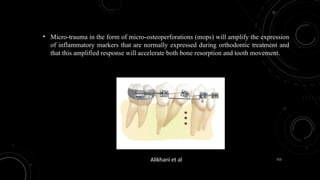
• Micro-trauma inthe form of micro-osteoperforations (mops) will amplify the expression
of inflammatory markers that are normally expressed during orthodontic treatment and
that this amplified response will accelerate both bone resorption and tooth movement.
Alikhani et al
113.
113
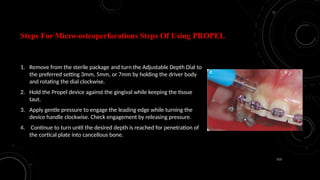
Steps For Micro-osteoperforationsSteps Of Using PROPEL
1. Remove from the sterile package and turn the Adjustable Depth Dial to
the preferred setting 3mm, 5mm, or 7mm by holding the driver body
and rotating the dial clockwise.
2. Hold the Propel device against the gingival while keeping the tissue
taut.
3. Apply gentle pressure to engage the leading edge while turning the
device handle clockwise. Check engagement by releasing pressure.
4. Continue to turn until the desired depth is reached for penetration of
the cortical plate into cancellous bone.
114.
114
5. The LEDDepth Stop indicator will illuminate when
desired depth is reached.
6. Rotate the device counter-clockwise to remove.
1-3 micro-osteoperforations are to be done depending on
proximity of anatomical structures. Perforations can be made
buccal or lingual in linear or triangular patterns
115.
115
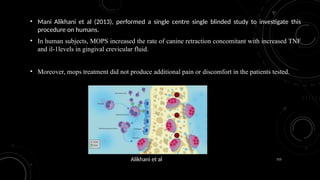
• Mani Alikhaniet al (2013), performed a single centre single blinded study to investigate this
procedure on humans.
• In human subjects, MOPS increased the rate of canine retraction concomitant with increased TNF
and il-1levels in gingival crevicular fluid.
• Moreover, mops treatment did not produce additional pain or discomfort in the patients tested.
Alikhani et al
116.
116
• Rate oftooth movement was compared in 3 groups:
1. Control that only received orthodontic force (O)
2. O + 1mop group, that in addition to orthodontic force
received 1 mop between canine and second premolar.
3. O + 4 mop group that in addition to orthodontic force
receive 4 mops in the same position.
117.
117
• At differenttime points after canine retraction, the rate of tooth movement and
levels of inflammatory marker il1-α were evaluated as described before.
• In response to mops, il1-α activity in the gingival crevicular fluid increased 5 fold
when compared with o group, 24 hours after mops procedure and coil activation,
and 3.5 fold after 28 days.
118.
118
• Mops wereable to increase the rate of more than 2 folds , while no significant difference
between o group and o + 1 mop group was observed.
119.
119
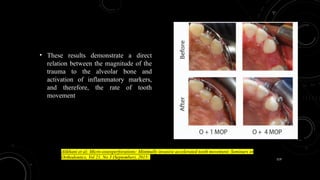
• These resultsdemonstrate a direct
relation between the magnitude of the
trauma to the alveolar bone and
activation of inflammatory markers,
and therefore, the rate of tooth
movement
Alikhani et al; Micro-osteoperforations: Minimally invasive accelerated tooth movement; Seminars in
Orthodontics, Vol 21, No 3 (September), 2015:
120.
120
Goals For MOPsDuring Orthodontic Treatment
• With the proper mechanical design, the incorporation of the catabolic effects of MOPs in each
stage of treatment has the following goals:
1. Accelerate the movement of target teeth
2. Facilitate the desired type of tooth movement
3. Development of biological anchorage
4. Decrease the possibility of root resorption
122
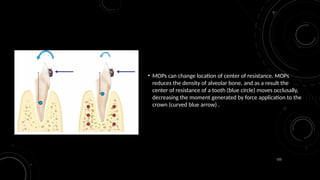
• MOPs canchange location of center of resistance. MOPs
reduces the density of alveolar bone, and as a result the
center of resistance of a tooth (blue circle) moves occlusally,
decreasing the moment generated by force application to the
crown (curved blue arrow) .
123.
123
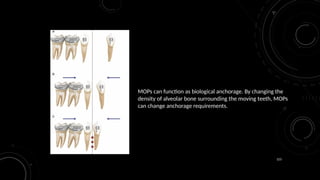
MOPs can functionas biological anchorage. By changing the
density of alveolar bone surrounding the moving teeth, MOPs
can change anchorage requirements.
124.
124
MOPs can preventroot resorption
during movement through dense
alveolar bone. Application of MOPs
stimulates recruitment and
activation of greater number of
osteoclasts from both PDL and bone
side, which shortens the duration of
necrosis, and of their presence in
the area.
126
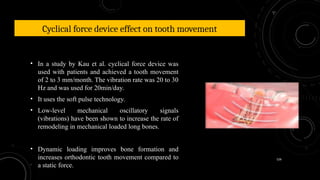
Cyclical force deviceeffect on tooth movement
• In a study by Kau et al. cyclical force device was
used with patients and achieved a tooth movement
of 2 to 3 mm/month. The vibration rate was 20 to 30
Hz and was used for 20min/day.
• It uses the soft pulse technology.
• Low-level mechanical oscillatory signals
(vibrations) have been shown to increase the rate of
remodeling in mechanical loaded long bones.
• Dynamic loading improves bone formation and
increases orthodontic tooth movement compared to
a static force.
127.
127
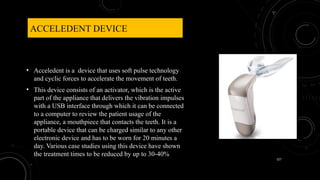
ACCELEDENT DEVICE
• Acceledentis a device that uses soft pulse technology
and cyclic forces to accelerate the movement of teeth.
• This device consists of an activator, which is the active
part of the appliance that delivers the vibration impulses
with a USB interface through which it can be connected
to a computer to review the patient usage of the
appliance, a mouthpiece that contacts the teeth. It is a
portable device that can be charged similar to any other
electronic device and has to be worn for 20 minutes a
day. Various case studies using this device have shown
the treatment times to be reduced by up to 30-40%
128.
128
• The rationaleis that this stimulates cell differentiation and maturation so that the
bone remodeling necessary for tooth movement occurs more quickly.
Significant difference in the rate of tooth movement with standard orthodontic
treatment alone (control group) compared with standard orthodontic treatment
plus the vibration applied for 20 minutes per day (vibration group) by the
acceledent® device
129.
129
• The applicationof cyclic loading (vibration) of 0.25 N (25 grams) at the
frequency of 30 hz, as an adjunct to treatment with a fixed orthodontic appliance,
significantly increases the rate of orthodontic tooth movement.
• There was no difference between the acceledent and control groups with respect
to age, ethnicity, or weight.
• The most common adverse side effect was loosening of tads.
Dubravko Pavlin, Ravikumar Anthony , Vishnu Raj , MS, Peter T. Gakunga; Cyclic Loading (Vibration)
Accelerates Tooth Movement in Orthodontic Patients: A Double-Blind, Randomized Controlled Trial,
Semin Orth 2015
131
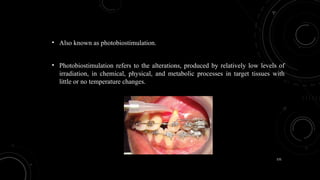
• Also knownas photobiostimulation.
• Photobiostimulation refers to the alterations, produced by relatively low levels of
irradiation, in chemical, physical, and metabolic processes in target tissues with
little or no temperature changes.
132.
132
• Photobiomodulation orlow level laser therapy (LLLT) is one of the
most promising approaches today.
• Laser has a biostimulatory effect on bone regeneration, which has
been shown in the midpalatal suture during rapid palatal expansion
and also stimulates bone regeneration after bone fractures and
extraction site
133.
133
• Two photobiostimulationmodalities:
• Low-level Light Emitting Lasers (Lllt)
• Light Emitting Diodes (Led)
• Both types of applications utilize a near-infrared wavelength of
approximately 600-1000 nm, with a range of 730-850 nm being viewed as
most appropriate for photobiostimulatory effects.
• The relatively narrow wavelength range allows for greater absorption by
target tissues
134.
134
• Photobiostimulation isnot associated with any harmful effects on the
periodontium and teeth.
• The apparent increase in tooth movement can be significant in the clinic provided
that more rigorous research, in both animal models and humans, is conducted to
improve the consistency and predictability of laser and led therapy usage
135.
135
• Although fewconflicting results were obtained that may be explained by the difference
in laser parameters used in each study regarding its type, application method, wavelength,
dose of irradiation, and exposure time as these parameters relate directly to laser clinical
results
Huang H, Williams RC, Kyrkanides S. Accelerated orthodontic tooth movement: molecular mechanisms. Am
J Orthod Dentofacial Orthop. 2014;146:620–632.
136.
136
Recent systematicreviews stated that there is a lack of evidence regarding LLLT’s
effectiveness in accelerating orthodontic tooth movement, so there is a need for well-
designed RCTs to determine the best protocols of laser parameters and present clear
recommendations about its effects
137.
137
LLLT dosefrom an 830-nm wavelength ga-al-as semiconductor laser
device with energy of 2 j/point used.
The laser group needed less mean time (81 +/- 15 days) to complete
leveling and alignment than did the control group (109 +/- 14 days)
138.
138
BIOLUX ORTHOPULSE
• Orthopulseis device that uses low levels of
light energy to stimulate the bone
surrounding the roots and facilitates tooth
movement which may reduce treatment
time for braces or clear aligners.
139.
139
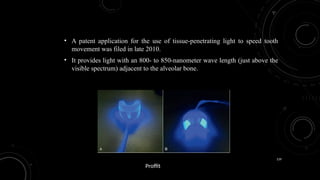
• A patentapplication for the use of tissue-penetrating light to speed tooth
movement was filed in late 2010.
• It provides light with an 800- to 850-nanometer wave length (just above the
visible spectrum) adjacent to the alveolar bone.
Proffit
140.
140
• Light inthis spectrum does penetrate soft tissue, and the idea is that it “infuses light energy
directly into the bone tissue”.
• This is said to excite intracellular enzymes and increase cellular activity in the PDL and bone,
increasing the rate of bone remodeling and tooth movement—but there has been no
demonstration of how that would work, and little in the way of evidence of faster tooth
movement.
• At present, as with vibrating devices, the major focus for Biolux is on improving the
performance of removable aligners, with no data as of 2017 to document its effectiveness.
142
PULSED ELECTROMAGNETIC FIELDS
•The PEMF affects the activity of cyclic adenosine monophosphate (camp) and cyclic
guanosine monophosphate (cgmp) by altering the cell membrane permeability.
• Darendeliler et al. In their study on guinea pigs observed increased rate of orthodontic
tooth movement in the presence of electromagnetic field, i.E., Either static or pulsed.
143.
143
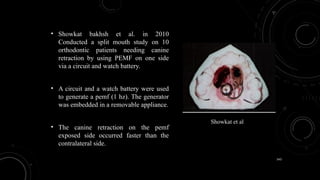
• Showkat bakhshet al. in 2010
Conducted a split mouth study on 10
orthodontic patients needing canine
retraction by using PEMF on one side
via a circuit and watch battery.
• A circuit and a watch battery were used
to generate a pemf (1 hz). The generator
was embedded in a removable appliance.
• The canine retraction on the pemf
exposed side occurred faster than the
contralateral side.
Showkat et al
144.
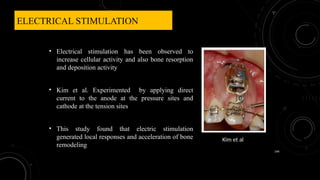
ELECTRICAL STIMULATION
• Electricalstimulation has been observed to
increase cellular activity and also bone resorption
and deposition activity
• Kim et al. Experimented by applying direct
current to the anode at the pressure sites and
cathode at the tension sites
• This study found that electric stimulation
generated local responses and acceleration of bone
remodeling
144
Kim et al
145.
145
EFFECT OF ELECTRICALSTIMULATION ON
ORTHODONTIC TOOTH MOVEMENT: A SYSTEMATIC
REVIEW
• Data was searched on this study by using pubmed, medline, excerpta medica
database(embase),research gate, and google scholar from january, 1950 until june 2019
• The capacity of electrical stimulation to enhance the rate of tooth movement has been
contemplated in several rcts.
146.
146
• The outcomesfrom all the RCT permits to conclude that electric stimulation combined
with induced tooth movement favors tissue response which is effective for increasing the
rate and amount of orthodontic tooth movement.
Agrawal et al; Effect of Electrical Stimulation on Orthodontic Tooth Movement: A Systematic
Review; IJO 2020 VOL. 30 NO. 3
147.
147
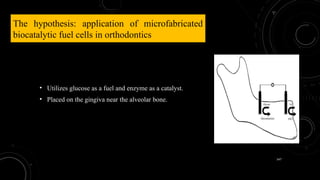
The hypothesis: applicationof microfabricated
biocatalytic fuel cells in orthodontics
• Utilizes glucose as a fuel and enzyme as a catalyst.
• Placed on the gingiva near the alveolar bone.
148.
148
• A combinedforce–electric treatment may provide a powerful and practical technique for
enhancing the velocity of orthodontic tooth movement, regardless the type of the
orthodontic appliance.
• Disadvantages:
• Short life span
• Poor power density
J. Kolahi et al; Microfabricated biocatalytic fuel cells: A new approach to accelerating the orthodontic
tooth movement; Medical Hypotheses (2009) 340–341
149.
149
LOW-INTENSITY PULSED ULTRASOUND(LIPUS)
• It is a clinically established, widely used and FDA approved intervention for
accelerating bone growth during healing of fractures, non-unions and other osseous
defects.
• Lipus is a form of physical energy that can be delivered into living tissues as acoustic
intensity waves
Andrade JR I, Sousa ABS, Silva GG. New therapeutic modalities to modulate orthodontic tooth movement. Dental
Press J Orthod. 2014 Nov-Dec;19(6):123-33
150.
150
• LIPUS whichgenerally uses frequencies varying between 0.5 – 1.5 mhz frequency pulses
(with a pulse width of 200 μs) and intensity output of 30 mw/cm2 (which is the output
signal of devices approved for clinical use), 5-20 minutes per day
Angle SR, Sena K, Summer DR, Virdi As. Osteogenic differentiation of rat bone marrow stromal cells by various intensities
of low-intensity pulsed ultrasound. Ultrasonics. 2011;51(3):281-8.
151.
151
• In vivoand in vitro studies have shown the direct effect of LIPUS on bone cells.
• Although the mechanism by which lipus increases the rate of fracture healing is
unclear, it is known that the mechanical strains received by cells are translated
into biochemical events.
152.
152
• LIPUS acceleratesthe differentiation pathway of mesenchymal stem cells in the
osteogenic lineage via activated phosphorylation of MAPK (mitogen-activated protein
kinase) pathways, up-regulation of cyclo-oxygenase-2 (COX-2), prostaglandin E2
(PGE2), altering the OPG/RANKL ratio in the microenvironment and stimulating the
production of bone morphogenetic proteins
153.
153
SMILESONICAAEVO
• The mostrecent entry into the tooth
acceleration market is low-intensity therapeutic
ultrasound—the aevo device, now being
marketed by smilesonica of canada.
• The theory is that increased blood flow in the
pdl would increase the rate of bone remodeling
and tooth movement and also could decrease
root resorption
Proffit
154.
154
The Aevodevice has maxillary and mandibular
mouthpieces with facial and lingual emitters , a coupling gel
for use in the mouthpieces, and a battery-powered energy
source.
It is used with an interface that allows selection of which
treatment zones are activated and monitors patient
compliance so that the doctor knows whether it is being used
and how much.
Proffit
155.
155
C
O
N
C
L
U
S
I
O
N
• Tooth accelerationphenomenon is still a relatively new horizon and researchers have
yet to seek a single most ideal and prudent technique for the patient.
• The surgical techniques have most of the human trials and also show very favorable
and long term effects adding to the stability and retention of the orthodontic therapy.
However the invasiveness and cost of these might make it little less viable option for
the patients.
156.
156
• Microsteoperforation, piezoincisionon the other hand are the least discomforting among all the
surgical procedures and this will make them more commonly used procedures in future.
• Yet at the same time any of these techniques once adapted depending upon clinician’s choice and
patient’s preference; can prove to be immensely beneficial in reducing orthodontic treatment
time.
157.
157
REFERENCES
• Alansari, sarahet al. Biological principles behind accelerated tooth movement.Seminars in orthodontics
2015,volume 21 , issue 3 , 151 - 161
• Krishnan V, davidovitch Z. Cellular, molecular, and tissue-level reactions to orthodontic force. Am J
orthod dentofacial orthop. 2006;129:469.E1–32
• Nimeri et al. Acceleration of tooth movement during orthodontic treatment - a frontier in orthodontics.
Progress in orthodontics 2013, 14:42
158.
158
• Paola castrogiovanniet al. The importance of physical activity in osteoporosis.From the molecular
pathways to the clinical evidence. Histol histopathol (2016) 31: 1183-1194
• Yamaguchi M. RANK/RANKL/OPG during orthodontic tooth movement. Orthod craniofac res. 2009;
12(2):113–9
• Kale S, kocadereli I, atilla P, asan E. Comparison of the effects of 1,25 dihydroxycholecalciferol and
prostaglandin E2 on orthodontic tooth movement. Am J orthod dentofacial orthop. 2004; 125(5):607–14.
159.
159
• Abhijith shettya; anand K. Patil; ameet R.; Prabhdeep K. Sandhu. Local infiltration of vitamin
D3 does not accelerate orthodontic tooth movement in humans. Angle orthodontist 2014
• Liou and huang. Rapid canine retraction through distraction of the periodontal ligament. Am J
orthod dentofacial orthop 1998;114:372-82.
• Xiao, yu, sun, and yeweng.Rapid canine retraction by distraction of the periodontal ligament.
Jco march 2016.
• Sukurica y, karaman a, gurel hg, dolanmaz d. Rapid canine distalization through segmental
alveolar distraction osteogenesis. Angle orthod. 2007; 77(2):226–36.
160.
160
• Kurt, gokmeniseri, haluk,kisnisci, reha; ozkaynak, ozkan. Rate of tooth movement and dentoskeletal effects
of rapid canine retraction by dentoalveolar distraction osteogenesis: A prospective study. Am J orthod
dentofacial orthop 2017;152:204-13.
• Almpani k,kantarci a. Surgical methods for the acceleration of the orthodontic tooth movement.Front oral
biol 2016.
• Oliveira d, oliveira b. F, rodrigo VS. Alveolar corticotomies in orthodontics: indications and effects on
tooth movement. Dental press J orthod 2010 july-aug;15(4):144-57.
161.
161
• Verna C.Regional acceleratory phenomenon. Front oral biol.2016;18:28-35.
• Nisha n. Et al. Wilckodontics- A magical wand for rapid success-a review. Annals of international
medical and dental research, vol (1), issue (3)
• Alikhani, mani et al. Micro-osteoperforations: minimally invasive accelerated tooth movement seminars
in orthodontics 2015 volume 21 , issue 3 , 162 – 169
• Pavlin, dubravko et al.Cyclic loading (vibration) accelerates tooth movement in orthodontic patients: A
double-blind, randomized controlled trial. Seminars in orthodontics , volume 21 , issue 3 , 187 – 19
162.
162
• Kolahi j,abrishami m, davidovitch z. Microfabricated biocatalytic fuel cells: a new approach to
accelerating the orthodontic tooth movement. Med hypotheses 2009 sep;73(3):340-1
• Orthodontics: diagnosis and management of malocclusion and dentofacial deformities; om P. Kharbanda;
elsevier third edition
• Contemporary orthodontic proffit, larson, sarver; elsevier; sixth edition
#19 Initial inflammatory response:
Chemokines released early in orthodontic tooth movement are critical for triggering bone resorption. Monocyte chemoattractant protein-1 (MCP-1/CCL2) recruits monocytes from the bloodstream to enter the surrounding tissue where they become tissue macrophages or, importantly to us, osteoclasts [9]. Similarly, CCL3 and [10] and CCL5 (RANTES) [11] released during orthodontic tooth movement lead to osteoclast recruitment and activation.
The primary pro-inflammatory cytokines released during orthodontic tooth movement are IL-1α, IL-1β, TNF-α, and IL-6
Two other classes of inflammatory mediators that are released during orthodontic tooth movement deserve special mention. First are the prostaglandins (PGs), which are derived from arachidonic acid metabolism and can mediate virtually every step of inflammation such as vasodilation, increase vascular permeability, and cellular adhesion. During orthodontic tooth movement, PGs are produced directly (by local cells or by inflammatory cells in response to mechanical stimulation) or indirectly (by cytokines). For example, TNF-α potently stimulates PGE2 formation [13]. PGs act locally where they are generated, and then they spontaneously decay or are enzymatically destroyed [14, 15]. Second are the neuropeptides that partici pate in many stages of inflammation due to orthodontic forces. Neuropeptides are small proteins, such as substance P, that transmit pain signals, regulate vessel tone, and modulate vascular permeability
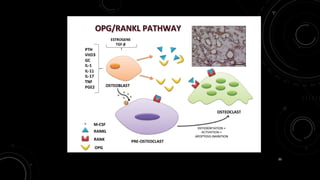
#30 OPG/RANKL pathway in bone remodeling. Osteoblasts produce RANKL, M-CSF OPG, regulators of the bone remodeling. M-CSF and RANKL induce the proliferation and differentiation of mature osteoclasts, respectively. OPG inhibits osteoclast differentiation binding to RANKL and, consequently, blocking binding between RANKL and RANK receptor present on the osteoclast precursor. Micrograph (A), RANKL immunoexpression (IHC-P) of osteoblasts in normal trabecular bone
How :
RANKL(also known as OPGL, ODF, and TRANCE), as a homotrimeric protein, is produced by osteoblasts and some other cells like activated T cells. RANKL has assignments for stimulating preosteoclasts’ differentiation [48], adher ence osteoclasts to bone tissue [49] and their following activation [48, 50], and their maintenance . RANKL, which is a secretion of preosteoblasts, osteoblasts, osteocytes, and periosteal cells [44–46], make RANK activated, which is expressed by os teoclasts and its precursors
RANK is also a homotrimeric transmembrane receptor from the TNF family.
#33 . During orthodontic tooth movement, PGs are produced directly (by local cells or by inflammatory cells in response to mechanical stimulation) or indirectly (by cytokines). For example, TNF-α potently stimulates PGE2 formation [13]. PGs act locally where they are generated, and then they spontaneously decay or are enzymatically destroyed
#49 Rats were divided at random into three groups: a chronic group (n ¼ 23) that received pharmacological treatment for 7 weeks (weeks 1–7), and orthodontic treatment for 3 weeks (weeks 5–7), an acute group (n ¼ 22) that received pharmacological treatment and orthodontic treatment simultaneously for 3 weeks (weeks 5–7), and a control group (n ¼ 19) without any pharmacological treatment but that received orthodontic treatment for 3 weeks (weeks 5–7). All animals were killed at the end of week 7
#55 It was found that these rapid movements are during the initial phases of tooth movement especially in the first week.
#56 Extraction of premolar
Equalizing Socket depth for canine as premolar roots shorter than the canine
Reduction of interdental bone
Vertical grooves made at mesiolingual and mesiobuccal line angles .
All these vertical cuts are joined with an oblique osteotomy at the base to form U-Shape groove.
#88 .A,Pretreatment view of patient undergoing PAOO procedure presenting with severe gingival recession on tooth
B, Composite restoration removed and corticotomies performed.
C, Subepithelial connective tissue graft placed under coronally advanced flap.
D, Two-year postsurgical result.
#92 Corticotomy – involves only outer cortex
Corticotectomy – cortiex & Medullary bone
#96 Surgery results in a substantial increase in alveolar demineralization, a transient and reversible condition. This will result in osteopenia (temporary decrease in bone mineral density). The osteopenia enables rapid tooth movement because teeth are supported by and moved through trabecular bone. As long as tooth movement continues, there is prolongation of RAP. When RAP dissipates, the osteopenia disappears and the radiographic image of normal spongiosa reappears. Then when orthodontic tooth movement is completed, an environment is created that favors alveolar re- mineralization.
#110 The anterior depth is usually 3 mm or less and the posterior is generally 5 mm or 7 mm
#114 Height of application of MOPs should be limited to attached gingiva for patient comfort.
#121 MOPs accelerate target tooth movement. MOPs (red circles) should be applied only around the target tooth to accelerate its rate of movement. When possible MOPs should be applied on both distal and mesial sides of the root to be moved.
Application of MOPs on residual alveolar ridge. When the target tooth is located adjacent to an extraction space, application of MOPs on the residual edentulous area of alveolar bone can increase the rate of movement significantly
#122 MOPs can change location of center of resistance. MOPs reduces the density of alveolar bone, and as a result the center of resistance of a tooth (blue circle) moves occlusally, decreasing the moment generated by force application to the crown (curved blue arrow) .
#123 Position of canine and posterior teeth before canine retraction.
Position of canine and posterior teeth during retraction, showing posterior teeth moved mesially while canine moved distally.
Position of canine and posterior teeth during retraction after application of MOPs (red circles). Posterior teeth moved mesially similar to (b) but the canine retraction increased. The increased distance traveled by the canine during retraction was not accompanied by additional movement of anchor teeth, and it was accomplished by biological anchorage a b
#124 (a) Schematic of tooth before application of force, (b) necrosis (pink area) after force application in the presence of MOPs, (c) large number of osteoclasts (red cells) recruited into the area clear the necrosis faster, (d) tooth movement accomplished without root resorption
#147 Biocatalytic fuel cells (enzyme batteries)-enzyme immobilized on an electrode surface using external substrates (formate or glucose) as the fuel to produce electricity.
We propose the idea of fabricating a system with an enzyme immobilized on an electrode surface using external substrates (for mate or glucose) as the fuel to produce electricity. Organic com pounds are not oxidized efficiently on electrode surface. However, when biocatalysts such as glucose oxidase or formate dehydrogenase are used, the enzyme’s substrate is reduced and electrons are transferred to the anode [5]. Thus, an enzyme battery could be fabricated with the combination of two enzyme elec trodes (Fig. 1). For crafting an integrated enzyme battery, two or more cells can be connected in series. All these individual cells are fabricated on a single silicon wafer and glucose solution is introduced into the cell by the capillary effect








































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















