Download to read offline
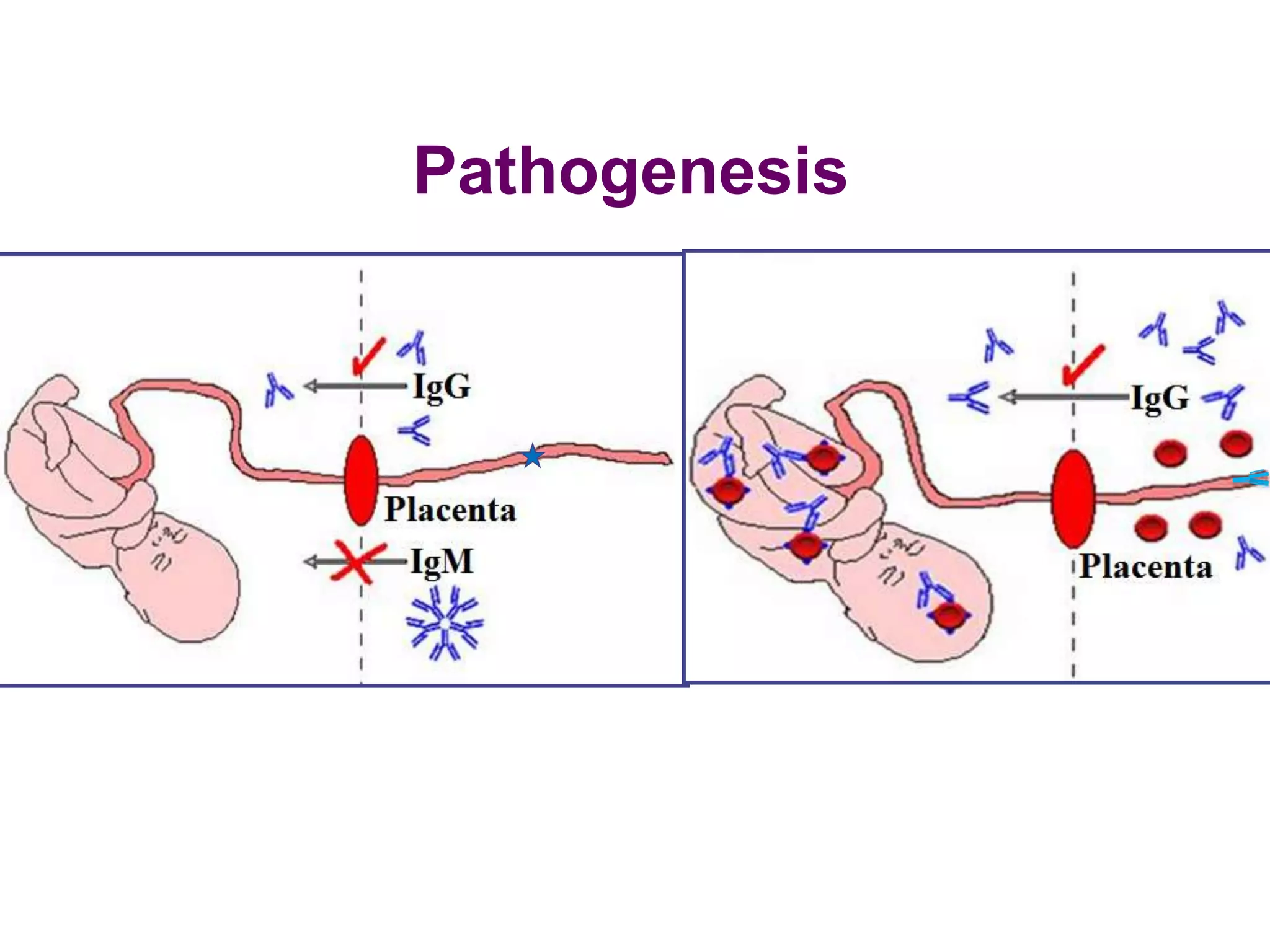
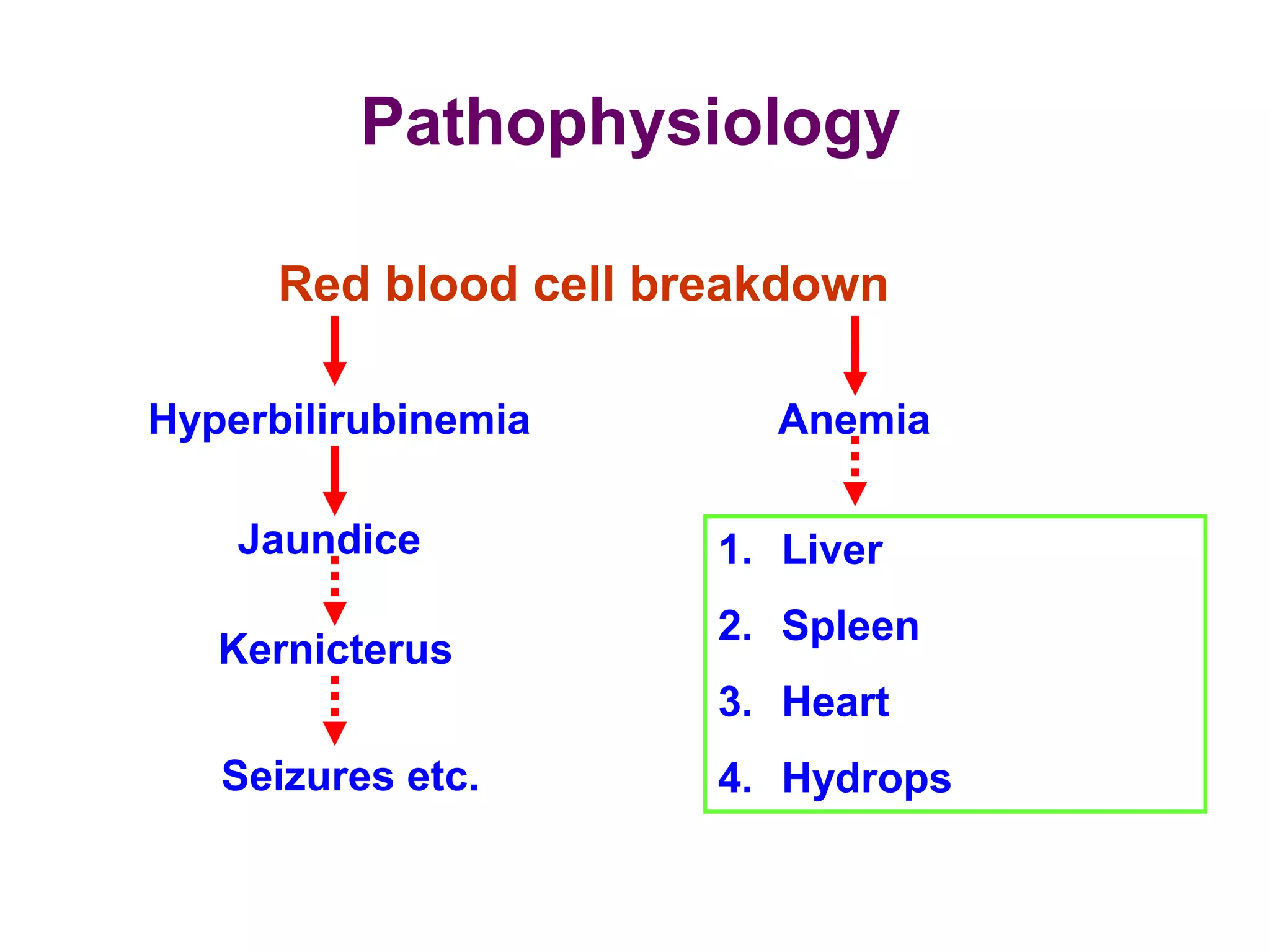

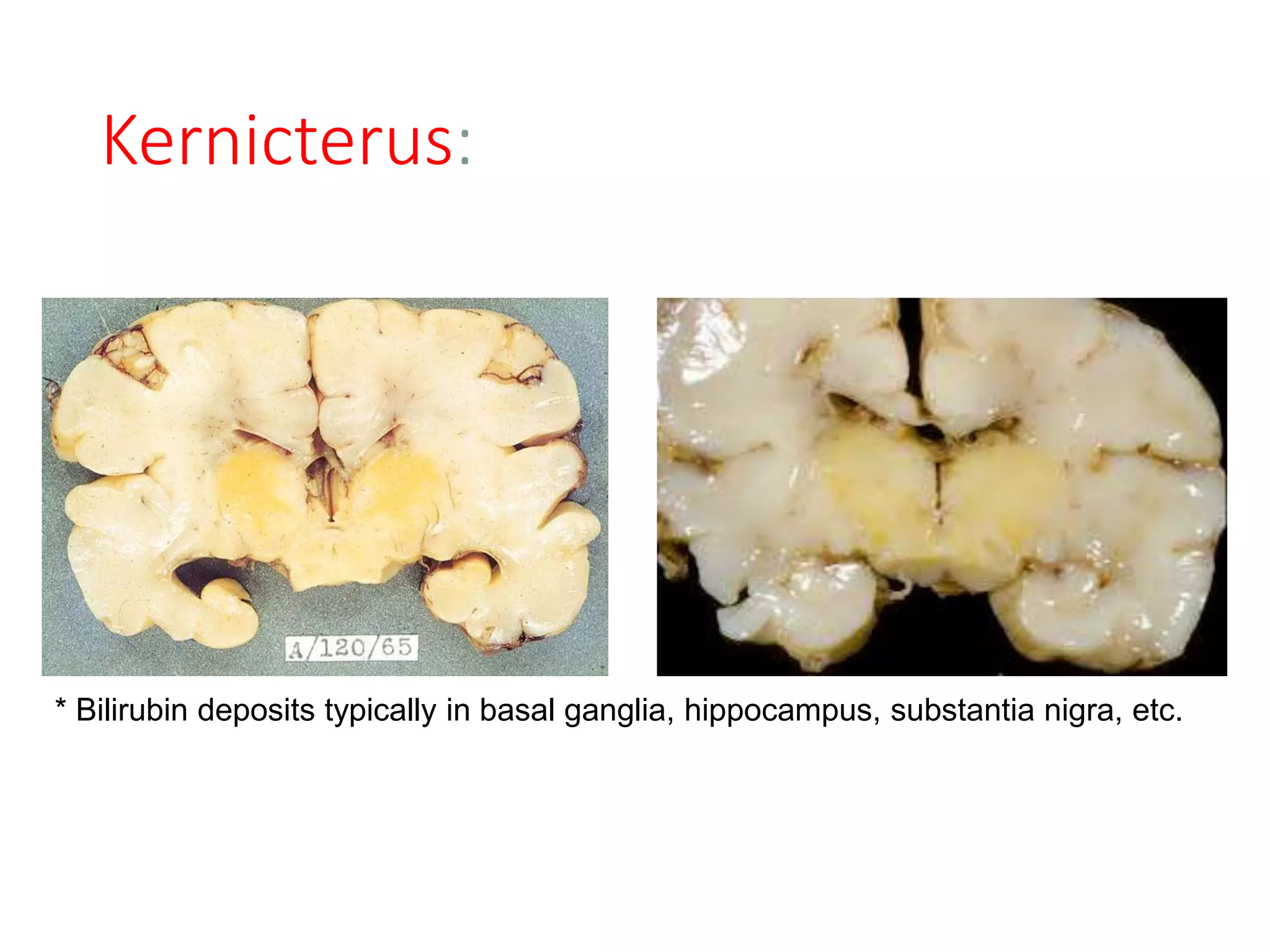
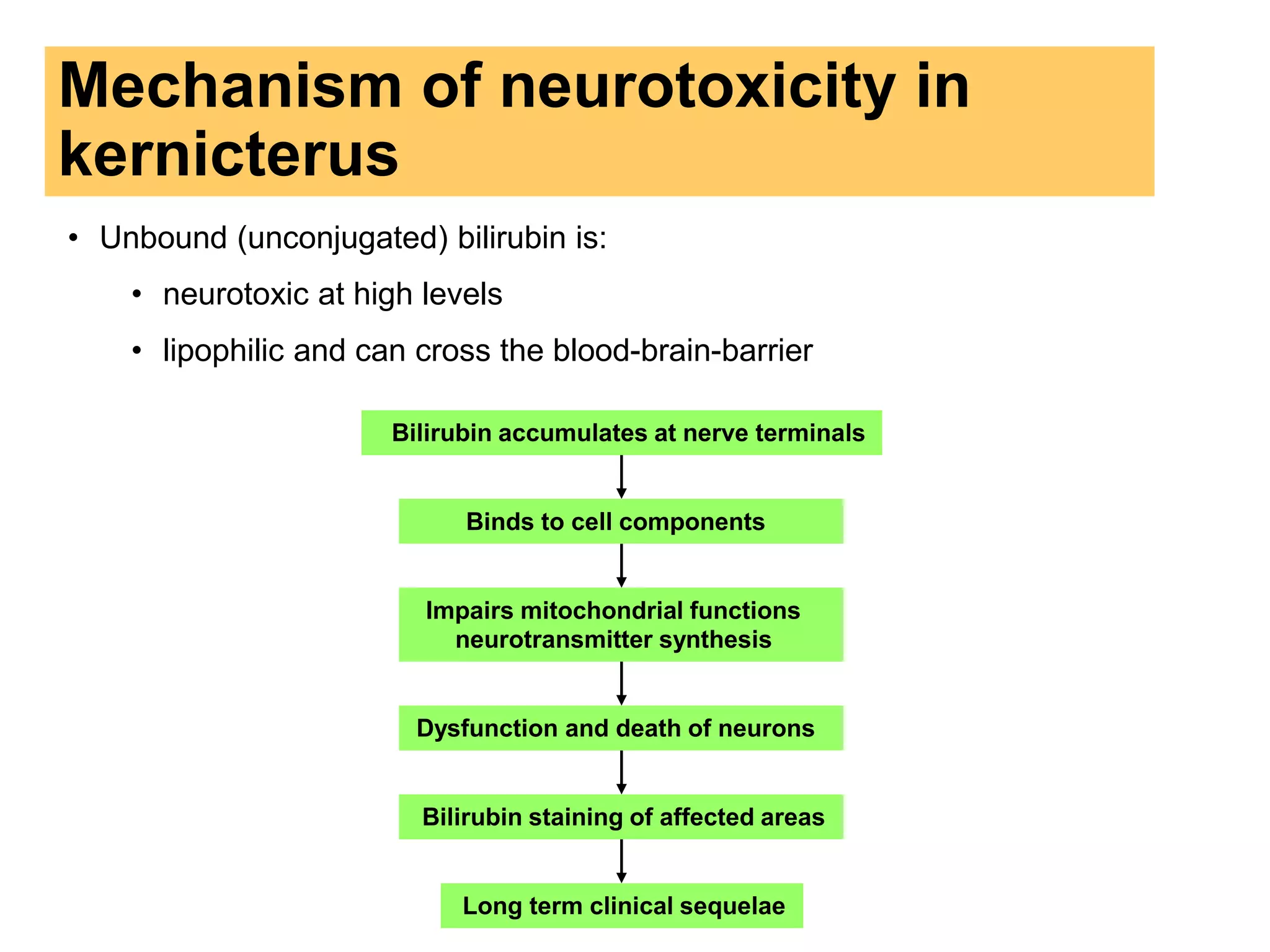


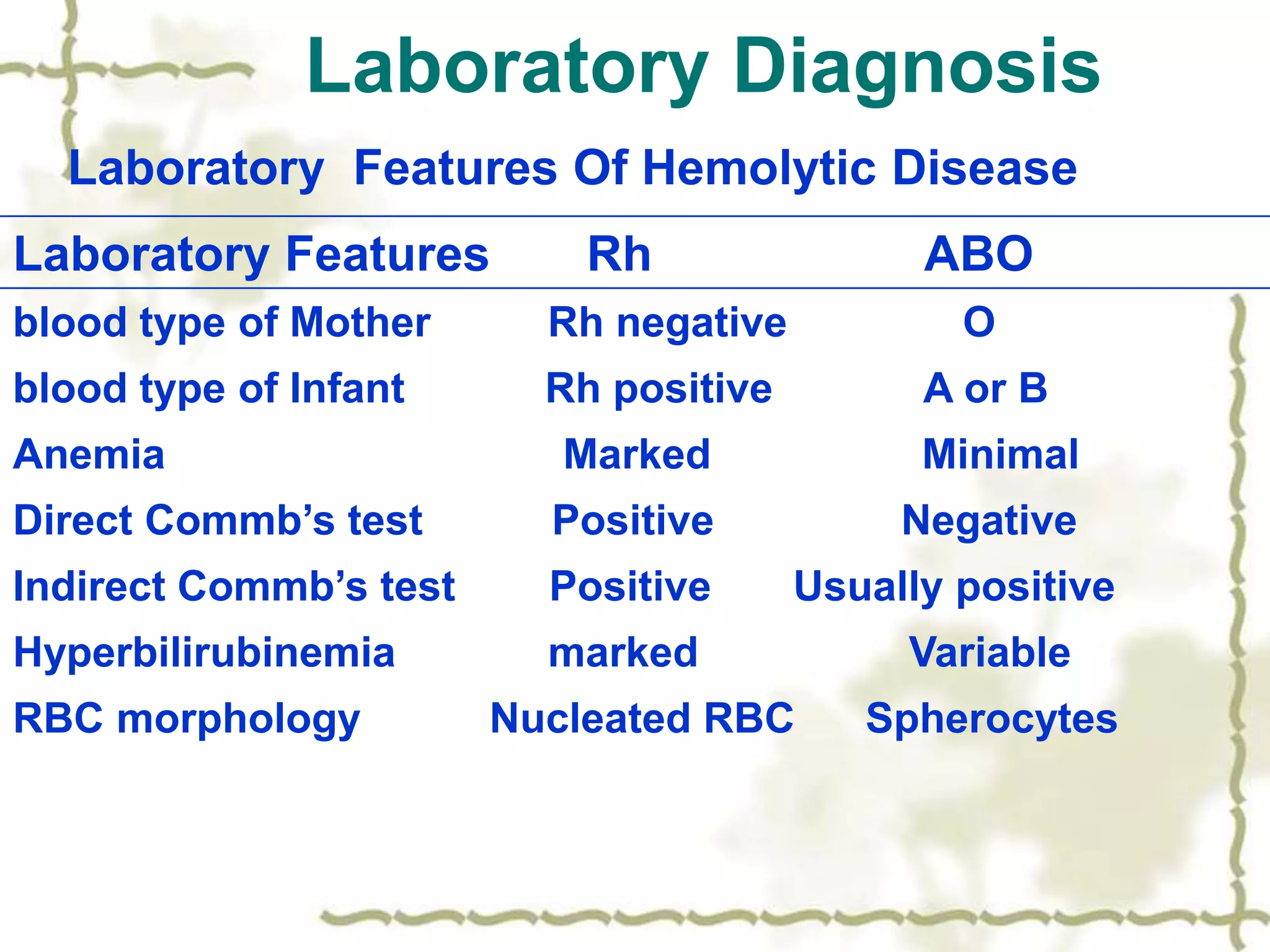



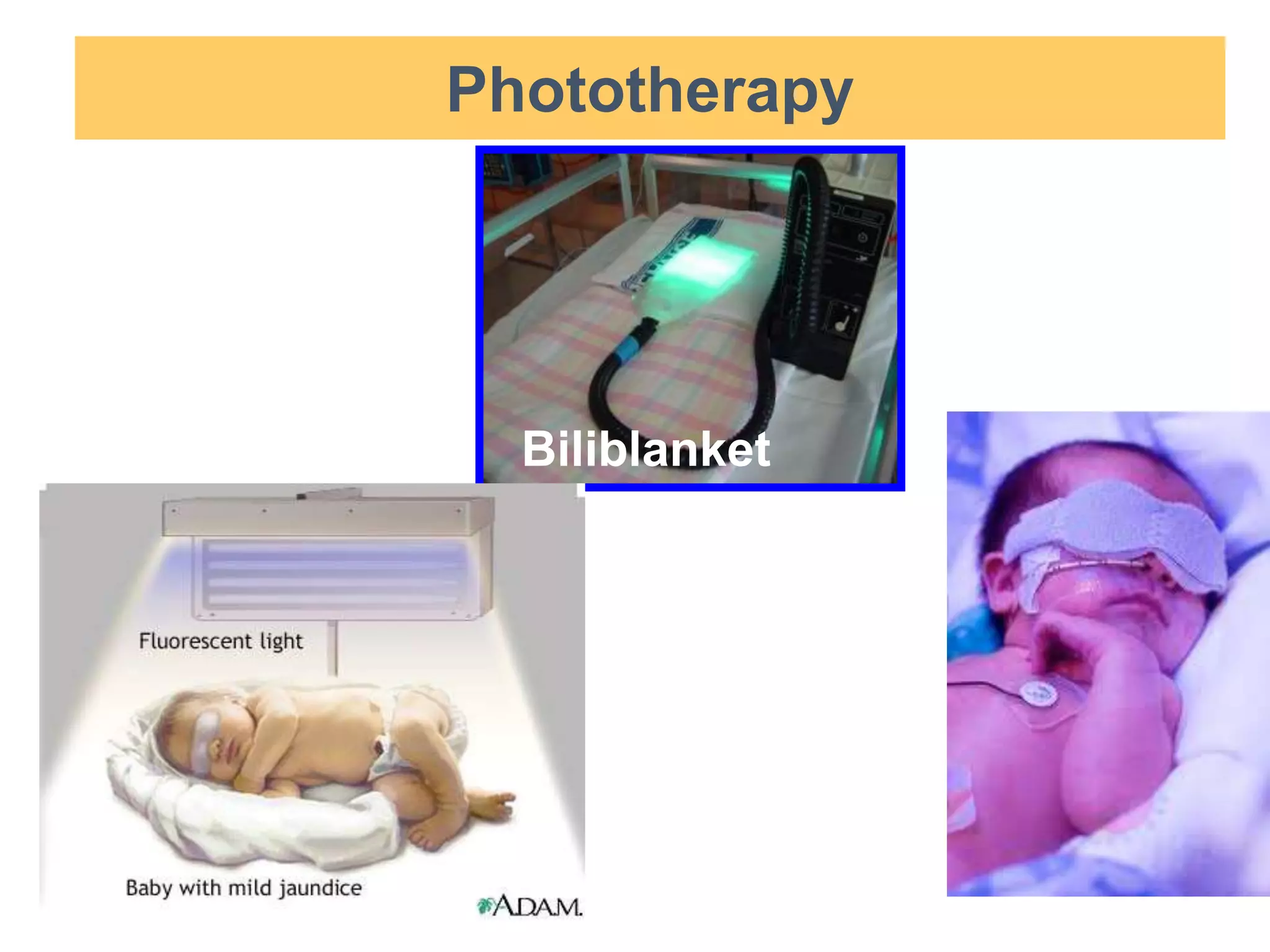
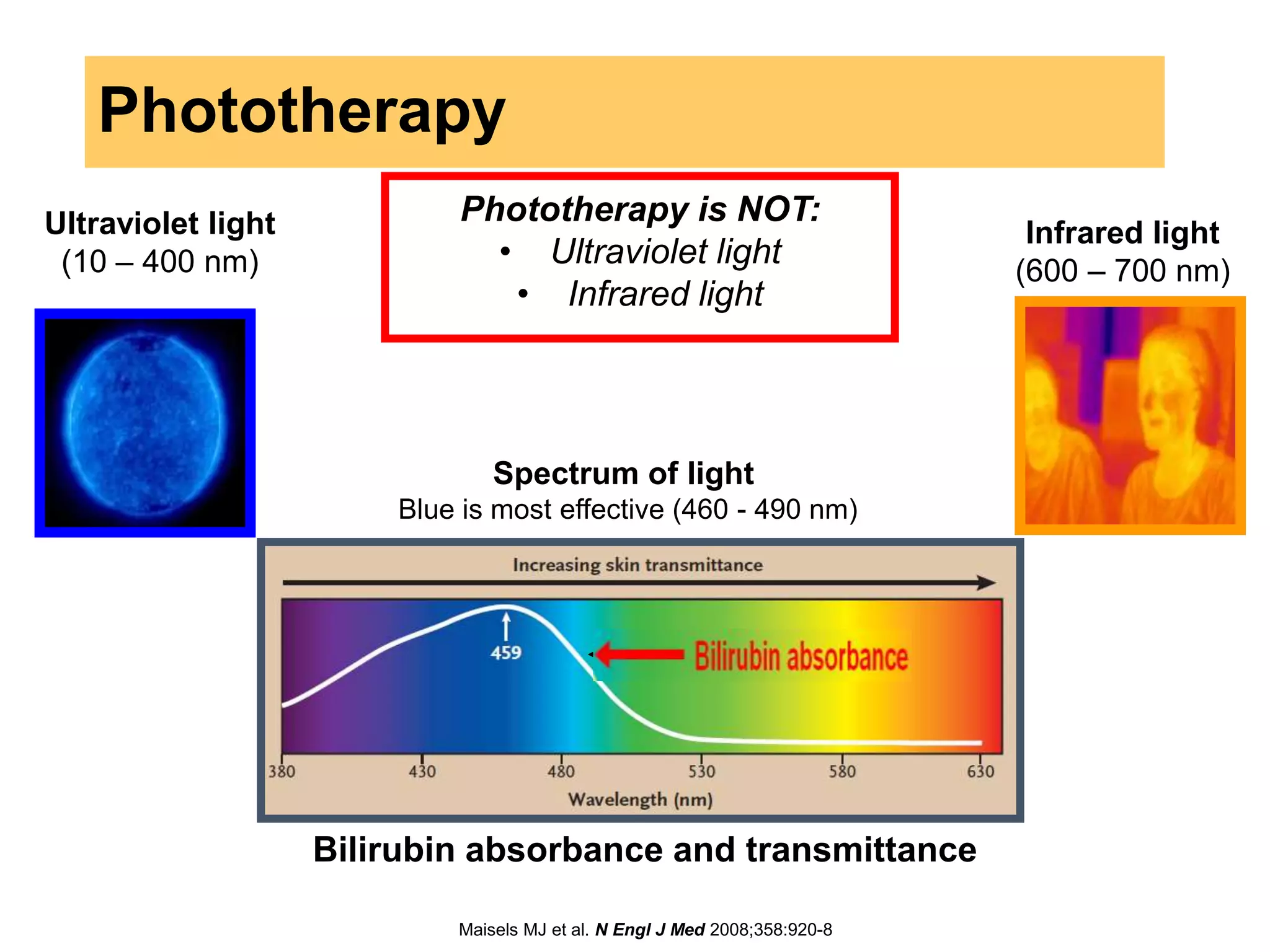


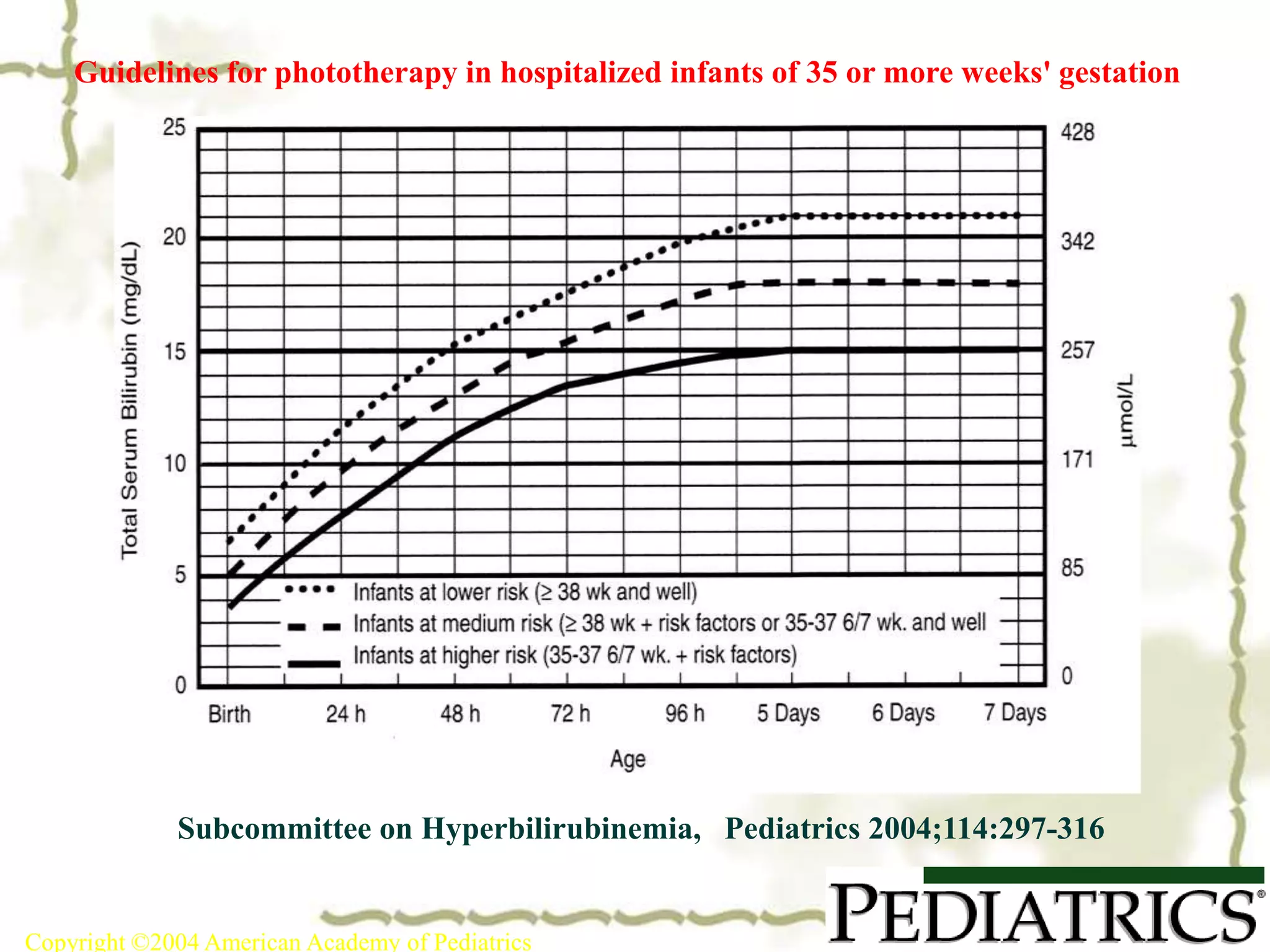






This document discusses ABO incompatibility, which is a type of hemolytic disease caused by a reaction between maternal anti-A or anti-B antibodies and fetal A or B antigens. It is usually milder than Rh incompatibility. The severity of hemolysis is greater in OA incompatibility. Treatment may include phototherapy or exchange transfusion if bilirubin levels are too high.































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)



