1. Liver function tests measure three categories: direct hepatocellular damage, cholestasis, and the liver's synthetic ability.
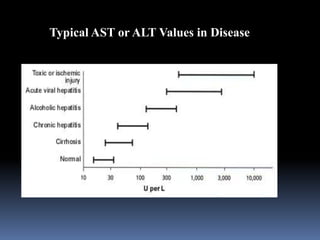
2. Transaminases like AST and ALT are elevated with hepatocyte injury from conditions like hepatitis, toxic injury, or ischemia. One-third of hepatitis C patients can have normal transaminase levels.
3. Cholestasis is reflected in elevated bilirubin and alkaline phosphatase levels, which take longer to rise than AST/ALT in acute bile duct obstruction.






![L8-Liver_Function_Test[1] SF.pptbwdqdbdwub](https://cdn.slidesharecdn.com/ss_thumbnails/l8-liverfunctiontest1sf-250507164033-55d694e3-thumbnail.jpg?width=640&height=640&fit=bounds)